3rd nerve palesey
Reading File
Finding Sources
Searching PubMed
"oculomotor nerve palsy" AND etiology
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Now I have comprehensive information to provide a thorough answer. Let me compile it.
Third Nerve (Oculomotor) Palsy
Anatomy of the Oculomotor Nerve
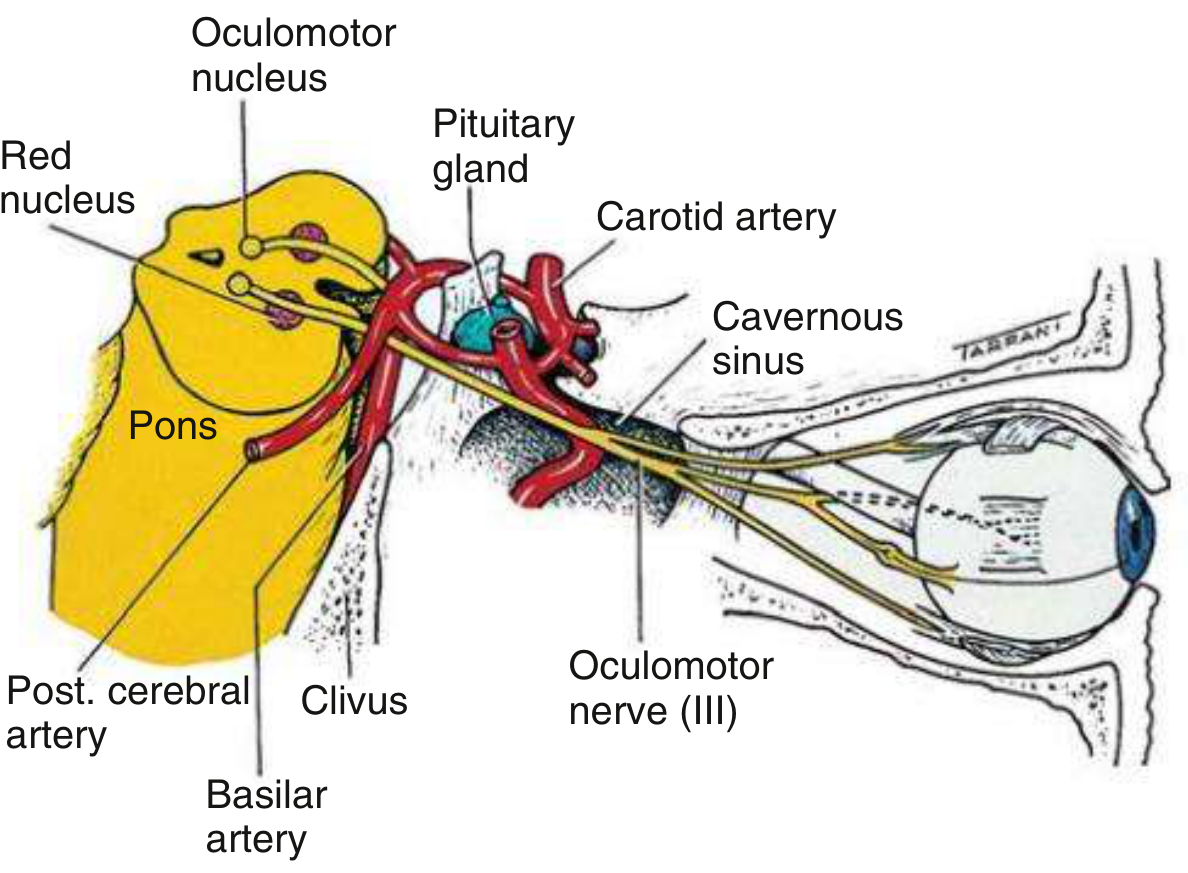
The third cranial nerve (CN III) travels a long course from nucleus to orbit, and the level of the lesion determines the clinical picture.
Nuclear complex (midbrain, level of superior colliculus):
- The levator subnucleus is unpaired and midline - a nuclear lesion causes bilateral ptosis
- Each superior rectus subnucleus innervates the contralateral superior rectus - a nuclear lesion causes contralateral (not ipsilateral) superior rectus weakness
- Medial rectus, inferior rectus, and inferior oblique subnuclei are ipsilateral
Fasciculus (through midbrain tegmentum): fibres pass through the red nucleus and cerebral peduncle, giving rise to classic brainstem syndromes (see below).
Subarachnoid/basilar course: nerve passes between the posterior cerebral artery and superior cerebellar artery, then runs parallel to the posterior communicating artery (PCoA) - making it vulnerable to aneurysmal compression here.
Cavernous sinus: CN III runs in the lateral wall, above CN IV. It divides into superior and inferior branches before entering the orbit through the superior orbital fissure.
Classic Clinical Features of a Complete Third Nerve Palsy
| Finding | Cause |
|---|---|
| Profound ptosis | Weakness of levator palpebrae |
| Eye deviated "down and out" | Unopposed lateral rectus (CN VI) and superior oblique (CN IV) |
| Dilated, unreactive pupil (mydriasis) | Loss of parasympathetic (Edinger-Westphal nucleus) input |
| Cycloplegia (loss of accommodation) | Loss of ciliary muscle innervation |
| Diplopia | Misalignment of visual axes |
A partial palsy may produce any combination of these findings. In primary position, the intact superior oblique also causes intorsion of the eye.
Pupil - The Most Clinically Critical Feature
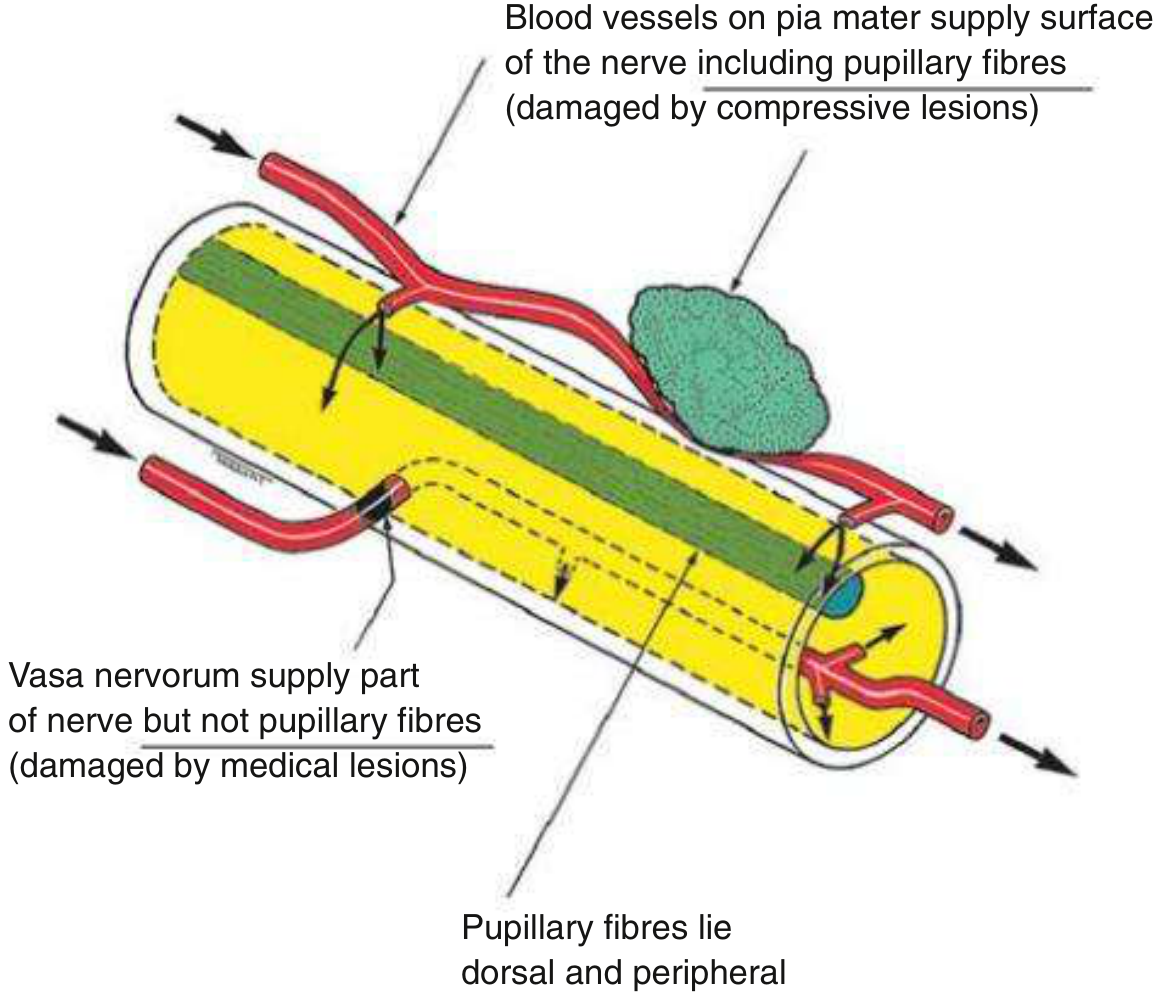
The parasympathetic pupillomotor fibres lie superficially in the superomedial nerve trunk, supplied by pial vessels. The main motor trunk is supplied by the vasa nervorum (intrinsic vasculature).
Surgical (compressive) lesions (aneurysm, uncal herniation, tumor):
- Compress the pial vessels and superficial pupillary fibres first
- Typically produce a pupil-involved (dilated, fixed) palsy
- This is a medical emergency
Medical (ischaemic) lesions (diabetes, hypertension):
- Infarct the vasa nervorum, damaging the central nerve trunk
- Superficial pupillomotor fibres are spared - pupil-sparing palsy
- Pain is often present (in ~2/3 of cases) even with ischaemia, so pain alone does not differentiate aetiology
Key caveat: Up to one-third of microvascular palsies may have mild relative pupil involvement (~0.8 mm anisocoria) with a reactive pupil. A completely fixed, dilated pupil with total ophthalmoplegia is the most specific sign of compression. Modern guidelines recommend emergent non-invasive vascular neuroimaging (CTA or MRA) for all third nerve palsies to exclude a PCoA aneurysm, regardless of pupil status.
Causes by Location
Nuclear (rare)
- Vascular disease, primary tumors, metastases
- Classic finding: bilateral ptosis + contralateral superior rectus weakness
- WEBINO syndrome (wall-eyed bilateral internuclear ophthalmoplegia) if bilateral medial rectus subnuclei involved
Fascicular (midbrain) - Associated Brainstem Syndromes
| Syndrome | Structures Involved | Features |
|---|---|---|
| Weber's | Cerebral peduncle | Ipsilateral CN III palsy + contralateral hemiparesis |
| Benedikt's | Red nucleus | Ipsilateral CN III palsy + contralateral tremor/chorea/athetosis |
| Nothnagel's | Superior cerebellar peduncle | Ipsilateral CN III palsy + cerebellar ataxia |
| Claude's | Red nucleus + superior cerebellar peduncle | Combination of Benedikt + Nothnagel |
Subarachnoid/Basilar
- PCoA aneurysm - most feared cause; acute, painful, pupil-involving. Compression only accounts for ~6% of all acute third nerve palsies but is immediately life-threatening
- Uncal herniation - trauma, mass lesion; compresses nerve over tentorial edge; starts with miosis then progresses to mydriasis and complete palsy
- Meningitis, subarachnoid haemorrhage, tumor, infarction
Cavernous Sinus
- Typically involves multiple cranial nerves (CN III, IV, VI, V1)
- Causes: carotid aneurysm, carotid-cavernous fistula, cavernous sinus thrombosis, pituitary adenoma, meningioma, Tolosa-Hunt syndrome, herpes zoster
- Diabetes is a common cause here (microvascular ischaemia)
Orbital Apex
- Involvement of CN III + IV + VI + V1 + optic nerve
- Plus orbital signs: proptosis, chemosis, conjunctival injection
- Causes: idiopathic orbital inflammation (IgG4), mucormycosis/aspergillosis (diabetics/immunosuppressed), tumor
Isolated Third Nerve Palsy - Clinical Approach
- Pupil-involved + complete ophthalmoplegia → aneurysm until proven otherwise → emergent CTA/MRA
- Pupil-sparing in an older patient with DM/HTN → microvascular ischaemia likely → CTA/MRA still recommended; ESR/CRP/CBC in elderly (exclude temporal arteritis)
- Partial palsy → must image regardless; partial involvement does not exclude aneurysm
- Pain → does NOT distinguish aneurysmal from ischaemic (present in ~2/3 of both)
- Expected resolution for microvascular palsy: 8-12 weeks spontaneously. If no resolution or new findings appear, reconsider the diagnosis
Aberrant Regeneration
Aberrant regeneration occurs when regenerating axons misroute to the wrong target muscle or iris.
Classic signs:
- Pseudo-von Graefe sign: eyelid elevation on downgaze or adduction (lid-gaze dyskinesis)
- Pupil-gaze dyskinesis: pupil constricts on downgaze or adduction (not light)
Important rule:
- After trauma or PCoA aneurysm compression - aberrant regeneration is expected
- Primary aberrant regeneration (no prior acute palsy) = almost always indicates a slowly growing parasellar lesion (cavernous sinus meningioma or internal carotid aneurysm) - requires neuroimaging
- Aberrant regeneration never follows microvascular ischaemia - if it appears in a presumed ischaemic palsy, imaging is mandatory
Key Differentials to Remember
- Myasthenia gravis: variable ptosis and ophthalmoplegia, fluctuating; pupil never involved; Tensilon test/AChR antibodies
- Thyroid ophthalmopathy: proptosis, lid retraction, restrictive pattern; pupil normal
- Ophthalmoplegic migraine (rare): recurrent, resolves over weeks-months; diagnosed in children with multiple prior episodes; do not diagnose de novo in adults
Sources: Kanski's Clinical Ophthalmology 10th Ed. | Adams and Victor's Principles of Neurology, 12th Ed. | Harrison's Principles of Internal Medicine 22nd Ed. | Bradley and Daroff's Neurology in Clinical Practice | The Wills Eye Manual
Localization
Localization
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.