Brain stroke treatment when my patient is known case of Hypertension since 15yrs and now my patient landed in icu and is his sbp is 200 mmHg
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ischemic stroke" AND "blood pressure" AND "hypertension" AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have all the information needed for a thorough, clinically structured answer. Here it is:
ICU Management: Acute Brain Stroke + SBP 200 mmHg in a Known Hypertensive
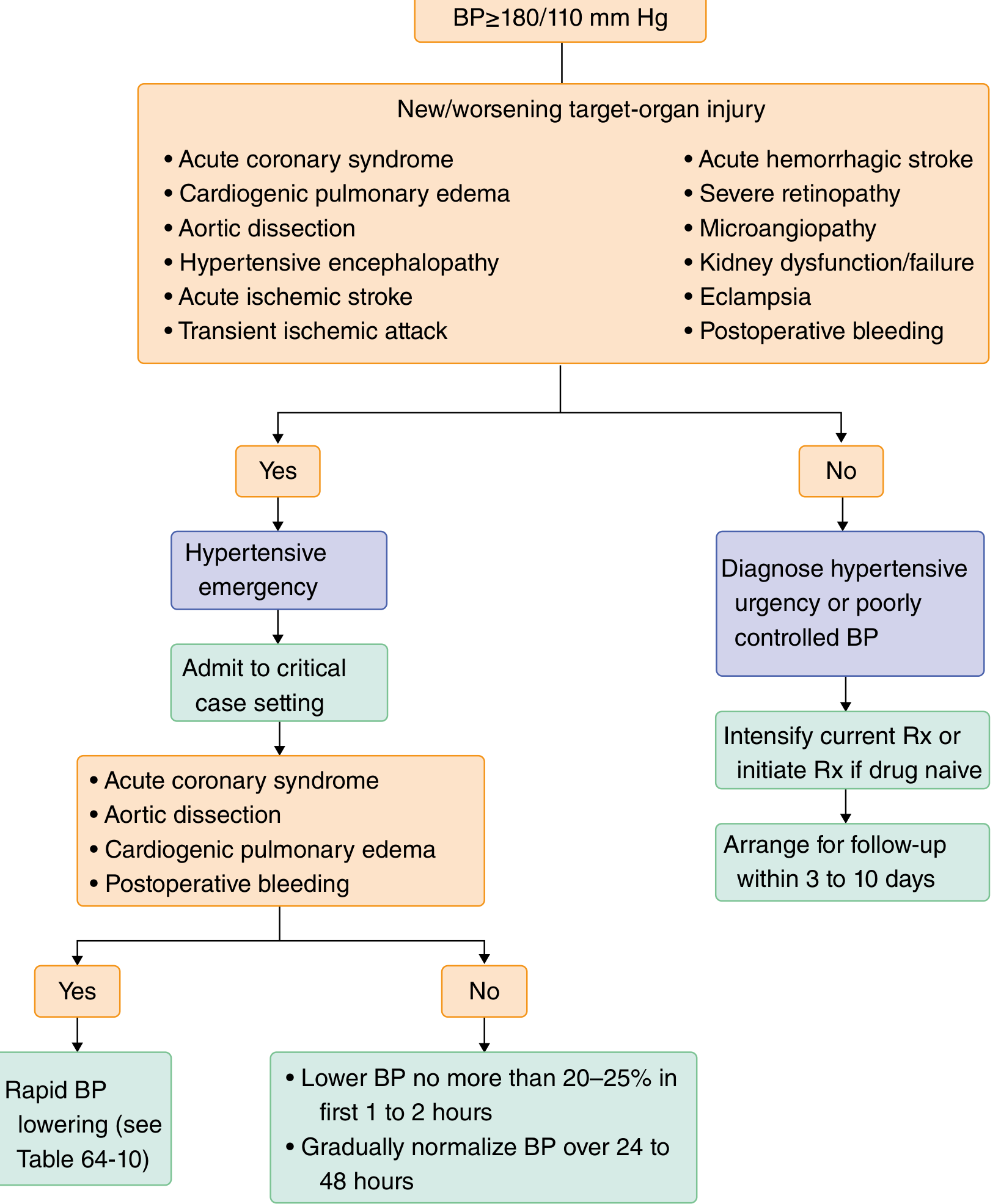
Your patient is a hypertensive emergency with stroke - the first and most important step is to determine the stroke type, as BP management differs fundamentally between ischemic and hemorrhagic stroke.
STEP 1: Immediate Workup (Do First)
| Action | Why |
|---|---|
| Urgent non-contrast CT head | Distinguish ischemic vs. hemorrhagic - cannot treat without this |
| Neurological assessment (GCS, NIHSS) | Establish severity baseline |
| Glucose, CBC, coagulation screen, metabolic panel | Rule out contraindications, identify complications |
| 12-lead ECG | AF is a common cause of cardioembolic stroke |
| Continuous cardiac/BP monitoring | Guide titration |
SCENARIO A: ACUTE ISCHEMIC STROKE (SBP 200 mmHg)
Key Principle: Permissive Hypertension
In a chronic hypertensive patient, the cerebral autoregulation curve is shifted rightward - the ischemic penumbra depends entirely on systemic pressure to maintain perfusion. Aggressive BP lowering can extend the infarct.
"Permissive hypertension allows for maximal cerebral perfusion. Systolic blood pressure >180 mmHg may require treatment, but the optimal MAP goal is between 100 and 140 mmHg."
- Schwartz's Principles of Surgery, 11th Ed.
If Patient IS Eligible for IV tPA (within 4.5 hours of onset):
SBP must be brought below 185 mmHg before tPA can be given (SBP >185 is a contraindication to thrombolysis).
Target: SBP <185 / DBP <110 mmHg
Preferred agents:
- Labetalol 10-20 mg IV over 1-2 min; may repeat or double every 10 min (max 300 mg total)
- Nicardipine IV infusion 5 mg/hr, titrate up by 2.5 mg/hr every 5-15 min (max 15 mg/hr)
After tPA is given, maintain SBP <180 mmHg for 24 hours to reduce hemorrhagic transformation risk.
If Patient is NOT Eligible for tPA:
Only treat if SBP >220 mmHg (AHA/ASA threshold for non-thrombolysis ischemic stroke).
At SBP 200 with no thrombolysis planned: do not aggressively lower BP - allow permissive hypertension. If you do treat, reduce MAP by no more than 15% over the first hour.
Preferred agents (same):
- Labetalol or Nicardipine IV infusion (titratable, predictable)
- Clevidipine IV (ultra-short-acting calcium channel blocker) is an alternative
Avoid:
- Sublingual nifedipine (precipitous uncontrolled drops)
- Nitroprusside (increases ICP via cerebral vasodilation)
- Aggressive diuretics
IV Fluids:
- Use normal saline (0.9% NaCl), not dextrose-containing solutions - glucose worsens neuronal injury in the ischemic penumbra via osmotic shift.
- Target normovolemia.
SCENARIO B: ACUTE HEMORRHAGIC STROKE / ICH (SBP 200 mmHg)
In intracerebral hemorrhage, hematoma expansion occurs in up to 73% within 24 hours - high BP drives this expansion and worsens outcome. BP lowering is more actively indicated here.
"For acute hemorrhagic stroke with SBP >180 mmHg - target: systolic BP 130-180 mmHg. Preferred: Labetalol OR Nicardipine. Timeline: immediate."
- Goldman-Cecil Medicine, International Ed.
Target: SBP 130-180 mmHg (do not drop below 130 - risk of perihematomal ischemia)
Preferred agents:
- Labetalol or Nicardipine IV infusion (as above)
Caveat: If there is elevated ICP (large hematoma, hydrocephalus), CPP = MAP - ICP. Over-lowering BP may critically reduce CPP. In that case, ICP monitoring is essential before setting BP targets.
- Comprehensive Clinical Nephrology, 7th Ed.
BP TARGET SUMMARY TABLE (Goldman-Cecil / ESC)
| Stroke Type | Trigger | Timeline | Target | Preferred Drug |
|---|---|---|---|---|
| Ischemic (no tPA) | SBP >220 | 1 hour | MAP -15% | Labetalol or Nicardipine |
| Ischemic (pre-tPA) | SBP >185 | 1 hour | SBP <185/DBP <110 | Labetalol or Nicardipine |
| Hemorrhagic ICH | SBP >180 | Immediate | SBP 130-180 | Labetalol or Nicardipine |
ICU Algorithm for This Patient (Hypertensive + Stroke, SBP 200)
Additional ICU Management Points
1. Glucose control
- Target euglycemia (140-180 mg/dL in ICU). Both hypoglycemia and hyperglycemia worsen stroke outcomes.
2. Temperature
- Treat fever aggressively (fever increases metabolic demand of penumbra tissue).
3. Antiplatelet / Anticoagulation
- Ischemic (non-tPA): Aspirin 325 mg within 24-48 hrs of CT confirmation of ischemia
- Hemorrhagic: Reverse any anticoagulants immediately (Vitamin K, PCC for warfarin; idarucizumab for dabigatran, andexanet alfa for Xa inhibitors)
4. Airway
- GCS <8 - intubate for airway protection; target PaCO2 35-40 mmHg (avoid hyperventilation unless herniation imminent)
5. Thrombolysis/Thrombectomy
- If ischemic, large vessel occlusion (LVO) confirmed on CTA: mechanical thrombectomy is preferred within 6 hours of onset (up to 24 hrs in selected cases)
- tPA window: 4.5 hours from symptom onset (3 hrs for patients >80, prior stroke + diabetes, anticoagulated, or NIHSS >25)
6. Cerebral edema
- Peaks at days 3-5 post-ischemic stroke. Large MCA or cerebellar infarcts may require decompressive hemicraniectomy.
7. DVT prophylaxis
- Mechanical (compression stockings) immediately; pharmacological prophylaxis with careful risk-benefit in hemorrhagic stroke.
Important Caveat for Your Patient (15-Year Hypertensive)
Long-standing hypertension shifts the autoregulatory curve rightward. This patient's "normal" autoregulation range is higher than a normotensive individual. A BP that looks dangerously elevated at 200 may actually be maintaining adequate cerebral perfusion. Err on the side of caution - avoid rapid drops. Reduce slowly, watch for neurological deterioration with every BP step.
Sources: Schwartz's Principles of Surgery 11e; Goldman-Cecil Medicine International Ed.; Comprehensive Clinical Nephrology 7e; Tintinalli's Emergency Medicine; Plum and Posner's Diagnosis and Treatment of Stupor and Coma. Recent meta-analysis (PMID 38767590) on intensive BP-lowering post-endovascular therapy supports cautious targets.
This is a shared conversation. Sign in to Orris to start your own chat.