Here is the complete, exam-ready answer for all 15 topics:
Anatomy Exam Answers - Complete Guide
1. Thalamic Nuclei [2011]
The thalamus is a paired ovoid gray matter structure forming the lateral wall of the 3rd ventricle. It is divided by the Y-shaped internal medullary lamina into three main nuclear groups.
Classification of Thalamic Nuclei
A. Relay (Specific) Nuclei
| Nucleus | Main Input | Main Output | Function |
|---|
| Ventral Posterior Lateral (VPL) | Medial lemniscus, spinothalamic tract | Somatosensory cortex | Relays spinal somatosensory inputs |
| Ventral Posterior Medial (VPM) | Trigeminal lemniscus, taste | Somatosensory + taste cortex | Relays cranial nerve sensory + taste |
| Lateral Geniculate (LGN) | Retina | Primary visual cortex (area 17) | Vision relay - "Lateral = Light" |
| Medial Geniculate (MGN) | Inferior colliculus | Primary auditory cortex (area 41/42) | Audition relay - "Medial = Music" |
| Ventral Lateral (VL) | Globus pallidus, deep cerebellar nuclei | Motor, premotor, supplementary motor cortex | Relays basal ganglia + cerebellar outputs |
| Ventral Anterior (VA) | Substantia nigra reticulata, GPi | Frontal lobe (widespread) | Motor relay for basal ganglia |
B. Association Nuclei (diffuse projections)
- Pulvinar - largest thalamic nucleus; input from superior colliculus; projects to parietotemporo-occipital association cortex; behavioral orientation to relevant stimuli
- Mediodorsal (MD) - input from amygdala, olfactory cortex; projects to prefrontal cortex; limbic/affective functions
- Lateral Dorsal nucleus - functions with anterior nuclei
C. Anterior Nuclear Group
- Input from mammillary body (via mammillothalamic tract) and hippocampus
- Projects to cingulate gyrus
- Part of Papez circuit; emotion and memory
D. Intralaminar Nuclei (within internal medullary lamina)
- Centromedian nucleus - input from globus pallidus, deep cerebellar nuclei; projects to striatum and motor cortex
- Parafascicular nucleus - pain modulation
- Function: maintain conscious alertness (ARAS relay)
E. Reticular Nucleus - thin shell of neurons; receives from all thalamic nuclei; sends inhibitory (GABA) fibers back to thalamus; acts as a gating mechanism
F. Midline Nuclei - hypothalamus, limbic connections; project to amygdala, hippocampus
Source: Neuroanatomy through Clinical Cases, 3rd Ed., Table 7.3, p. 308; Kenhub Thalamic Nuclei
2. Boundaries and Communications of the 3rd Ventricle [2010]
The 3rd ventricle is a narrow, slit-like cavity in the diencephalon, lying in the midline between the two thalami.
Boundaries
- Roof - fornix, choroid plexus of the 3rd ventricle, ependyma
- Floor - optic chiasma (anteriorly), tuber cinereum, infundibulum, mammillary bodies, posterior perforated substance, tegmentum of midbrain
- Anterior wall - lamina terminalis, anterior commissure
- Posterior wall - posterior commissure, pineal body (habenular commissure above, posterior commissure below)
- Lateral walls - medial surface of thalamus (the two thalami are joined by the interthalamic adhesion/massa intermedia in ~70% of people), hypothalamus below the hypothalamic sulcus
Communications
- Anterosuperiorly - communicates with each lateral ventricle via the interventricular foramen of Monro (one on each side)
- Posteroinferiorly - communicates with the 4th ventricle via the cerebral aqueduct (of Sylvius) through the midbrain
Recesses
- Optic recess - above optic chiasma
- Infundibular recess - extends into infundibular stalk
- Pineal recess - between the two pineal stalks
- Suprapineal recess - above pineal body
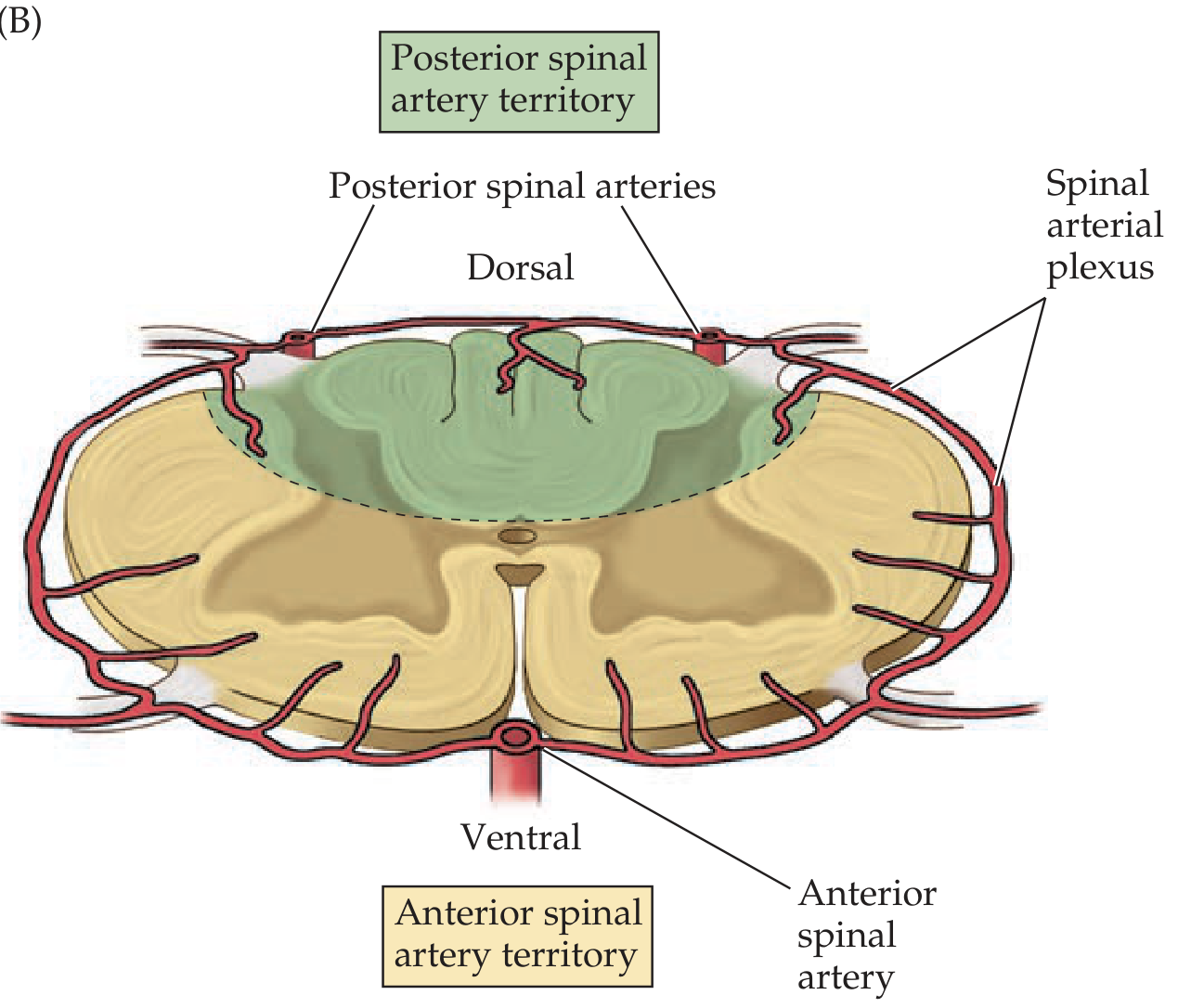
3. Blood Supply of the Spinal Cord [2017]
Arterial Supply
Longitudinal Arteries:
- Anterior Spinal Artery (ASA) - formed by fusion of branches from both vertebral arteries; runs in the anterior median fissure; supplies anterior 2/3 of cord (anterior horn, anterolateral funiculus, spinothalamic tracts, corticospinal tracts)
- Posterior Spinal Arteries (PSA, x2) - arise from vertebral or PICA; run along posterolateral sulci; supply posterior 1/3 (posterior columns, dorsal horn)
Radicular Arteries (segmental feeders):
- 31 segmental branches enter the spinal canal, but only 6-10 reach the cord as radicular arteries
- Artery of Adamkiewicz (Arteria radicularis magna) - most important; typically arises from left intercostal/lumbar vessels at T9-T12 (sometimes L1-L2); provides major supply to lower thoracic and lumbosacral cord
- Spinal arterial plexus (vasocorona) surrounds the cord connecting anterior and posterior systems
Venous Drainage
- 6 longitudinal venous channels (anterior and posterior median veins + 4 anterolateral/posterolateral veins)
- Drain via intervertebral veins into the internal vertebral venous plexus (Batson's plexus)
Clinical significance: Anterior spinal artery syndrome = loss of motor function + pain/temperature below lesion, with preserved proprioception/vibration (posterior columns spared)
Source: Neuroanatomy through Clinical Cases, 3rd Ed., p. 472-477
4. Speech Areas of the Brain [2015, 2018 supple]
Motor Speech Area (Broca's Area)
- Location: Inferior frontal gyrus (pars triangularis + pars opercularis), Brodmann areas 44 and 45, left hemisphere (dominant)
- Function: Speech production and articulation - controls the coordinated muscular activity for speaking
- Damage (Broca's aphasia): Non-fluent, effortful speech with intact comprehension; "telegraphic" speech; patient knows what they want to say but cannot say it fluently
Sensory Speech Area (Wernicke's Area)
- Location: Posterior part of superior temporal gyrus, Brodmann area 22, left hemisphere
- Function: Speech comprehension (understanding spoken and written language)
- Damage (Wernicke's aphasia): Fluent speech but with paraphasia (wrong words/neologisms), poor comprehension; patient is unaware of errors
Arcuate Fasciculus
- A bundle of white matter fibres connecting Broca's and Wernicke's areas
- Damage: Conduction aphasia - fluent speech, good comprehension, but poor repetition
Angular Gyrus (Area 39)
- At the junction of temporal-parietal-occipital lobes
- Important for reading and writing; damage causes alexia with agraphia
Supplementary Motor Area (SMA)
- Medial surface of frontal lobe (area 6)
- Initiates speech; damage causes mutism/transcortical motor aphasia
Key Teaching Points for Exams
- All speech areas are in the left (dominant) hemisphere in ~97% of right-handers
- Broca's = motor/expressive aphasia (problem with output)
- Wernicke's = sensory/receptive aphasia (problem with input/comprehension)
- Both areas connected by arcuate fasciculus
5. Motor Neurons of the Spinal Cord [2010 supple]
Alpha Motor Neurons (Lower Motor Neurons)
- Located in the anterior horn of spinal cord gray matter
- Large multipolar neurons forming Rexed lamina IX
- Send myelinated axons (alpha fibers) via ventral roots to innervate extrafusal muscle fibers
- Each motor neuron innervates multiple muscle fibers = motor unit
Gamma Motor Neurons
- Also in anterior horn, smaller than alpha neurons
- Innervate intrafusal muscle fibers (muscle spindle fibers)
- Regulate sensitivity of muscle spindle (proprioception)
- Co-activated with alpha neurons (alpha-gamma co-activation)
Upper vs. Lower Motor Neuron Distinctions
| Feature | UMN | LMN |
|---|
| Location | Cortex, corticospinal tracts | Anterior horn, ventral root |
| Tone | Increased (spasticity) | Decreased (flaccidity) |
| Reflexes | Hyperreflexia | Hyporeflexia/areflexia |
| Weakness | Less severe | More severe/wasting |
| Babinski | Present | Absent |
| Fasciculations | Absent | Present |
| Atrophy | Mild (disuse) | Severe (denervation) |
Renshaw Cells
- Inhibitory interneurons in the anterior horn
- Activated by collaterals of alpha motor neuron axons
- Provide recurrent inhibition back onto the same motor neuron (feedback control)
Topographic Organization (Somatotopy)
- Medial motor neurons innervate axial/trunk muscles
- Lateral motor neurons innervate distal limb muscles
6. Corpus Callosum [2011 supple]
The corpus callosum is the largest white matter commissure, connecting the two cerebral hemispheres.
Parts (Anterior to Posterior)
- Rostrum - thin anterior part, connects orbital frontal lobes
- Genu - curves anteriorly; connects prefrontal cortex (frontal forceps minor)
- Body (Trunk) - largest part; connects frontal, parietal lobes
- Splenium - posterior thickening; connects occipital, posterior temporal, parietal lobes (forceps major, tapetum)
Relations
- Superior surface - cingulate gyrus runs above it (separated by callosal sulcus); median longitudinal stria
- Inferior surface - septum pellucidum (between genu and fornix); body of fornix
- Anterior - genu curves under to form rostrum, then connects to lamina terminalis
- Posterior - splenium overhangs the pineal body and midbrain
Functions
- Interhemispheric transfer of sensory, motor, and cognitive information
- Coordinates activities between hemispheres
- Important for bimanual coordination
Corpus Callosum Agenesis
- May be partial or complete
- Can be silent or associated with intellectual disability, seizures
- Associated with Dandy-Walker malformation, lissencephaly
- Detected on MRI: absent corpus callosum, widely spaced parallel ventricles ("bat wing" appearance), colpocephaly
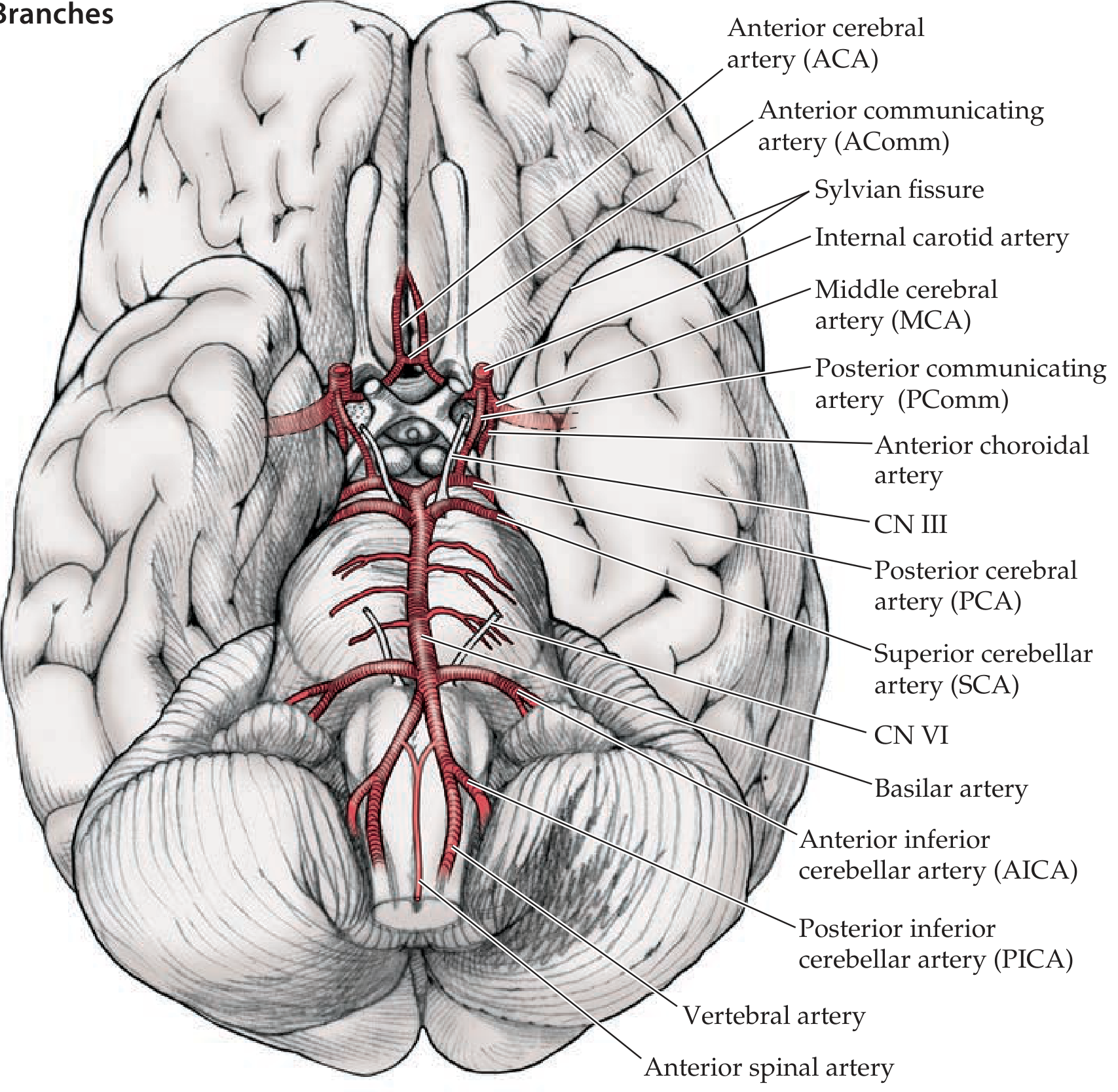
7. Circle of Willis [2014 supple]
The Circle of Willis (circulus arteriosus cerebri) is the anastomotic ring at the base of the brain that connects the anterior (carotid) and posterior (vertebrobasilar) circulations.
Components (from anterior, clockwise)
- Anterior communicating artery (AComm) - connects the two ACAs
- Anterior cerebral artery (ACA) x2 - terminal branch of ICA; supplies medial frontal and parietal lobes
- Internal carotid artery (ICA) x2 - enters from below
- Posterior communicating artery (PComm) x2 - connects ICA to PCA; joins anterior and posterior circulations
- Posterior cerebral artery (PCA) x2 - terminal branches of basilar artery; supplies occipital lobes, medial temporal
- Basilar artery - formed by union of both vertebral arteries; not technically in the circle but feeds it
Additional Branches Noted
- Middle cerebral artery (MCA) - largest branch of ICA (not part of circle itself)
- Anterior choroidal artery - from ICA
- Superior cerebellar artery (SCA)
- Anterior inferior cerebellar artery (AICA)
- Posterior inferior cerebellar artery (PICA)
Clinical Importance
- Allows collateral flow if one vessel is occluded
- A complete circle is present in only ~34% of individuals (variants are common)
- Common site of berry/saccular aneurysms: AComm (most common), PComm, MCA bifurcation
- PComm aneurysm classically causes CN III palsy (compresses oculomotor nerve)
Source: Neuroanatomy through Clinical Cases, 3rd Ed., p. 417
8. Fornix [2017 supple]
The fornix is the principal output pathway of the hippocampal formation, part of the limbic system.
Structure
- A C-shaped white matter tract that arches from the hippocampus around the thalamus to the hypothalamus
- Bilateral (one from each hippocampus); the two limbs join and partially decussate at the midline forming the hippocampal commissure (psalterium)
Parts (following the fiber from posterior to anterior)
- Fimbria - begins on the medial surface of the hippocampus
- Crus of fornix (crura) - the two crura emerge from the fimbria and arch forward
- Body of fornix - two crura join below the corpus callosum (septum pellucidum lies between them and corpus callosum)
- Columns of fornix - at the anterior end of the body, the fornix divides into two columns that curve downward
- Pre-commissural fibers - pass anterior to anterior commissure to septal nuclei
- Post-commissural fibers - pass posterior to anterior commissure to mammillary bodies of hypothalamus (main destination)
Connections (Summary)
- From: Hippocampus, subiculum, entorhinal cortex
- To: Mammillary bodies (main), anterior thalamic nucleus, septal nuclei, hypothalamus
Papez Circuit
Hippocampus → Fornix → Mammillary bodies → Mammillothalamic tract → Anterior thalamic nucleus → Cingulate gyrus → Cingulum → Entorhinal cortex → Hippocampus
Clinical: Damage to Fornix
- Bilateral damage causes anterograde amnesia (difficulty forming new memories)
- The fornix runs in the floor of the lateral ventricle; may be damaged during surgery near the third ventricle
9. Medial Medullary Syndrome [2017 supple]
Also called Dejerine's syndrome. Results from occlusion of the anterior spinal artery or paramedian branches of the vertebral artery, causing infarction of the medial medulla.
Structures Affected and Features
| Structure Damaged | Clinical Feature |
|---|
| Corticospinal tract (pyramid) | Contralateral hemiplegia/hemiparesis (spares face) |
| Medial lemniscus | Contralateral loss of proprioception, vibration, and discriminative touch (from body) |
| Hypoglossal nerve (CN XII) fibers | Ipsilateral LMN tongue paralysis (tongue deviates toward lesion) |
Key: "Medial = 3 M's" mnemonic
- Motor (corticospinal pyramid)
- Medial lemniscus
- Motor of tongue (CN XII)
Differences from Lateral Medullary Syndrome
- Medial: contralateral hemiplegia + contralateral dorsal column loss + ipsilateral tongue palsy
- Lateral (Wallenberg): Horner's, dysphagia, ipsilateral ataxia, alternating sensory loss (spinothalamic crossed, trigeminal ipsilateral), NO hemiplegia
10. Third Ventricle of Brain [2018 supple]
(See Topic 2 above for Boundaries and Communications - this is the same topic with a broader scope)
Additional Points for "Third Ventricle" Questions
Development: Derived from the cavity of the prosencephalon (forebrain vesicle)
Choroid Plexus of 3rd Ventricle:
- Hangs from the roof between the two thalami
- Produced by invagination of pia mater + ependyma
- Produces cerebrospinal fluid (CSF)
Clinical Correlates:
- Obstruction at foramen of Monro → obstructive hydrocephalus affecting one or both lateral ventricles (colloid cyst is a common cause)
- Obstruction at cerebral aqueduct → non-communicating hydrocephalus (bilateral lateral + 3rd ventricle dilation, 4th ventricle normal)
- Hypothalamic tumors (craniopharyngioma) arise near the floor of 3rd ventricle
- Pineal tumors compress the aqueduct causing Parinaud syndrome (loss of upward gaze)
11. Pia Mater of the Spinal Cord [2018 supple]
The pia mater is the innermost, most delicate meningeal layer, closely investing the spinal cord surface.
Structure
- Thin, highly vascular, transparent membrane
- Closely adherent to the surface of the spinal cord and cannot be separated from it without damage
- Composed of flattened mesothelial cells and collagen fibers
Specializations of the Spinal Pia Mater
-
Denticulate (Dentate) Ligaments
- Bilateral serrated lateral extensions of pia mater
- Run between dorsal and ventral roots, attaching laterally to the dura mater
- 21 pairs total (from C1 to just above L1)
- Function: anchor and suspend the spinal cord within the dural tube, preventing excessive movement
-
Filum Terminale (Internum)
- At the conus medullaris (L1-L2), the pia mater continues as the filum terminale internum
- Thin thread (~20 cm long) of pia + glial tissue
- Extends through the lumbar cistern to the tip of the dural sac at S2, then as the filum terminale externum (coccygeal ligament) to the coccyx
- Function: anchors the spinal cord inferiorly
-
Anterior Median Fissure - pia dips into the anterior median fissure, carrying with it the anterior spinal artery
Relation to Dentate Ligament (Exam Point)
- Denticulate ligaments lie in the coronal plane, dividing the subarachnoid space into anterior and posterior compartments
- Useful surgical landmark during spinal surgery
12. Sensory and Motor Speech Areas of the Brain [2022]
(See Topic 4 for detailed coverage - this is essentially the same topic)
Summary Table
| Area | Location | Brodmann | Function | Lesion |
|---|
| Broca's (motor) | Inferior frontal gyrus | 44, 45 | Speech production/articulation | Non-fluent aphasia |
| Wernicke's (sensory) | Posterior superior temporal gyrus | 22 | Speech comprehension | Fluent aphasia, poor comprehension |
| Angular gyrus | TPO junction | 39 | Reading, writing, semantics | Alexia + agraphia |
| Supramarginal gyrus | Parietal | 40 | Phonological processing | Conduction aphasia (sometimes) |
| Arcuate fasciculus | White matter tract | - | Connects Broca's + Wernicke's | Conduction aphasia (poor repetition) |
| SMA | Medial frontal | 6 | Speech initiation | Mutism, transcortical motor aphasia |
13. Lateral Medullary Syndrome (Wallenberg Syndrome) - Anatomical Basis [2025]
Vascular Cause
Most commonly due to vertebral artery occlusion (atherothrombosis); less often PICA occlusion. Causes infarction of a wedge-shaped area of lateral medulla (posterior to inferior olivary nucleus) + inferior cerebellum.
Clinical Features with Anatomical Basis
| Clinical Feature | Structure Damaged | Location |
|---|
| Ipsilateral facial pain/temperature loss | Spinal nucleus + tract of CN V | Posterolateral medulla |
| Contralateral body pain/temperature loss | Spinothalamic tract (already crossed) | Anterolateral medulla |
| Dysphagia, dysarthria, hoarseness | Nucleus ambiguus (CN IX, X) | Lateral medulla |
| Ipsilateral Horner syndrome (miosis, ptosis, anhidrosis) | Descending sympathetic fibers (hypothalamospinal) | Posterolateral tegmentum |
| Vertigo, nausea, vomiting, nystagmus | Vestibular nuclei (inferior + medial) | Lateral medulla |
| Ipsilateral limb ataxia, falling toward lesion | Inferior cerebellar peduncle (restiform body) | Lateral medulla |
| Hiccups | Dorsolateral medulla (respiratory centers) | Rare |
| Ipsilateral soft palate paresis, loss of gag | Nucleus ambiguus | CN IX, X |
Key Examination Point: Crossed Sensory Loss
- Face ipsilateral (CN V nucleus is ipsilateral) + body contralateral (spinothalamic tract already crossed in cord)
- Motor system (pyramids) is NOT affected (pyramids are medial, not lateral)
- Posterior columns (vibration/proprioception) are NOT affected (medial location)
Diagnostic Triad
Horner syndrome + Ipsilateral ataxia + Contralateral hypalgesia = Lateral medullary infarction
Source: Localization in Clinical Neurology, 8e, p. 5609-5670; Adams & Victor's Principles of Neurology, 12th Ed., p. 816
14. Cross Section of Midbrain at Superior Colliculus + Weber Syndrome [2025]
Cross Section of Midbrain at Level of Superior Colliculus
SUPERIOR COLLICULUS (roof/tectum)
| |
Central Gray Matter (PAG)
|
____________________
| TEGMENTUM |
| Red nucleus (large) |
| CN III nucleus |
| Medial lemniscus |
| Spinothalamic tract |
| Medial longitudinal |
| fasciculus (MLF) |
| CN III fibers (exit |
| medially through |
| tegmentum) |
|____________________|
|
SUBSTANTIA NIGRA (pars compacta + pars reticulata)
|
CEREBRAL PEDUNCLE (CRUS CEREBRI)
[lateral = fibers to cortex / corticospinal tract medial 3/5]
[Corticospinal = middle 3/5; Corticopontine = medial 1/5 + lateral 1/5]
|
INTERPEDUNCULAR FOSSA
Key Structures at This Level:
- Tectum (roof): Superior colliculi (visual reflex centers)
- Tegmentum: Red nucleus, CN III nucleus + fibers, MLF, substantia nigra, decussation of superior cerebellar peduncle (at inferior colliculus level), reticular formation, medial lemniscus, spinothalamic tract
- Cerebral peduncle (Basis pedunculi/Crus cerebri): Corticospinal, corticobulbar, and corticopontine fibers
- CN III exits between cerebral peduncles (through interpeduncular fossa), passes between PCA and SCA, travels in the wall of cavernous sinus
Weber Syndrome
Definition: A midbrain stroke syndrome causing superior alternating hemiplegia - ipsilateral CN III palsy with contralateral hemiparesis.
Lesion Site: Ventromedial midbrain - affects the cerebral peduncle (crus cerebri) and CN III fibers (oculomotor fascicles in the interpeduncular cistern)
Blood Supply: Occlusion of paramedian mesencephalic branches or peduncular perforating branches of the posterior cerebral artery (PCA)
Clinical Features:
| Feature | Anatomical Basis |
|---|
| Ipsilateral CN III palsy (ptosis, mydriasis, "down and out" eye) | CN III fibers pass through/near the cerebral peduncle |
| Contralateral hemiplegia/hemiparesis | Corticospinal fibers in the cerebral peduncle (cross in medullary pyramids) |
| No cerebellar signs | Red nucleus and cerebellum spared (compare Benedikt syndrome) |
Comparison with Benedikt Syndrome:
- Benedikt = CN III palsy + contralateral tremor/ataxia (red nucleus + CN III, deeper tegmental lesion)
- Weber = CN III palsy + contralateral hemiplegia (peduncle lesion)
Source: StatPearls - Weber Syndrome (NIH); Wikipedia; Neuroanatomy
15. Klinefelter Syndrome [2025]
Definition
Male hypogonadism in an individual with at least two X chromosomes and one or more Y chromosomes. Classic karyotype: 47, XXY.
Genetics
- Results from non-disjunction of sex chromosomes during meiosis
- Maternal and paternal non-disjunction contribute equally
- ~15% show mosaicism (e.g., 46,XY/47,XXY) - mosaics have milder features
- Advanced maternal age is a risk factor (but less strongly than in trisomy 21)
Clinical Features
- Only consistent finding: Hypogonadism
- Body habitus: Tall, long lower limbs; eunuchoid proportions (span > height; lower segment > upper segment)
- Testes: Markedly small (2 cm); firm due to hyalinization of seminiferous tubules
- Gynecomastia - in ~50%
- Reduced facial, body, and pubic hair
- Azoospermia/oligospermia - infertility in virtually all (unless mosaic)
- Decreased serum testosterone, elevated serum FSH and LH (hypergonadotropic hypogonadism)
- Mild intellectual disability / verbal skill deficits (variable)
Histopathology
- Hyalinization and fibrosis of seminiferous tubules (ghost tubules)
- Leydig cells appear prominent/hyperplastic
- Absent/markedly reduced spermatogenesis
Associated Conditions
- Metabolic syndrome, type 2 diabetes (insulin resistance)
- Mitral valve prolapse (~50% of adults)
- 20-30x increased risk of extragonadal germ cell tumors (mediastinal teratoma)
- Increased risk of breast cancer (20x above normal males)
- Increased autoimmune diseases (SLE, RA)
- Osteoporosis (due to hypogonadism)
Diagnosis
- Karyotype (gold standard)
- Hormonal: Low testosterone, high FSH/LH
- Testicular biopsy: hyalinized tubules
Treatment
- Testosterone replacement (improves secondary sexual characteristics, bone density, mood, libido)
- Does NOT restore fertility (sperm retrieval via TESA + ICSI may help mosaics)
- Psychological support
Source: Robbins & Kumar Basic Pathology, p. 128
Quick Reference Summary Table
| Topic | Key Mnemonic / Recall Point |
|---|
| Thalamic nuclei | LGN = Lateral Light; MGN = Medial Music; VPL = Spine; VPM = Face |
| 3rd ventricle | Monro anteriorly, Sylvius posteriorly |
| Spinal blood supply | 1 anterior + 2 posterior spinal arteries; Artery of Adamkiewicz at T9-T12 |
| Speech | Broca's = 44/45 (motor); Wernicke's = 22 (sensory) |
| Corpus callosum | Rostrum, Genu, Body, Splenium (R-G-B-S) |
| Circle of Willis | ACA + AComm + ICA + PComm + PCA (complete ring in only 34%) |
| Fornix | Hippocampus → Mammillary body → Anterior thalamus → Cingulate = Papez circuit |
| Medial medullary | 3 M's: Motor (pyramid), Medial lemniscus, Motor of tongue (CN XII) |
| Lateral medullary | Horner + ipsilateral ataxia + contralateral hemihypalgesia; NO hemiplegia |
| Weber syndrome | Ventromedial midbrain; CN III (ipsilateral) + hemiplegia (contralateral) |
| Klinefelter | 47,XXY; small testes + gynecomastia + infertility; high FSH/LH |
| Pia mater | Denticulate ligaments (21 pairs) + filum terminale |