Heart
Reading File
Asking for Preferences
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have everything needed for a thorough, well-illustrated answer. Here is the full summary:
Congenital Heart Disease (CHD)
Overview
Congenital heart defects occur in approximately 8 in 1000 live births and range from hemodynamically trivial to immediately life-threatening. About 10% are associated with genetic syndromes (trisomy 21, Turner's, Noonan's), VACTERL association, or other organ malformations. The remaining 90% result from isolated embryologic abnormalities or undetermined genetic lesions. - Tintinalli's Emergency Medicine, p. 862
The classic classification divides CHD into two broad categories based on physiology:
ACYANOTIC (Left-to-Right Shunts)
These are the most common congenital cardiac malformations. Left-to-right shunting initially causes pulmonary overcirculation without cyanosis. However, prolonged shunting eventually causes pulmonary hypertension and reversal to right-to-left shunting (cyanosis) - this is Eisenmenger syndrome, at which point defects are considered irreversible. This is why early intervention is recommended.
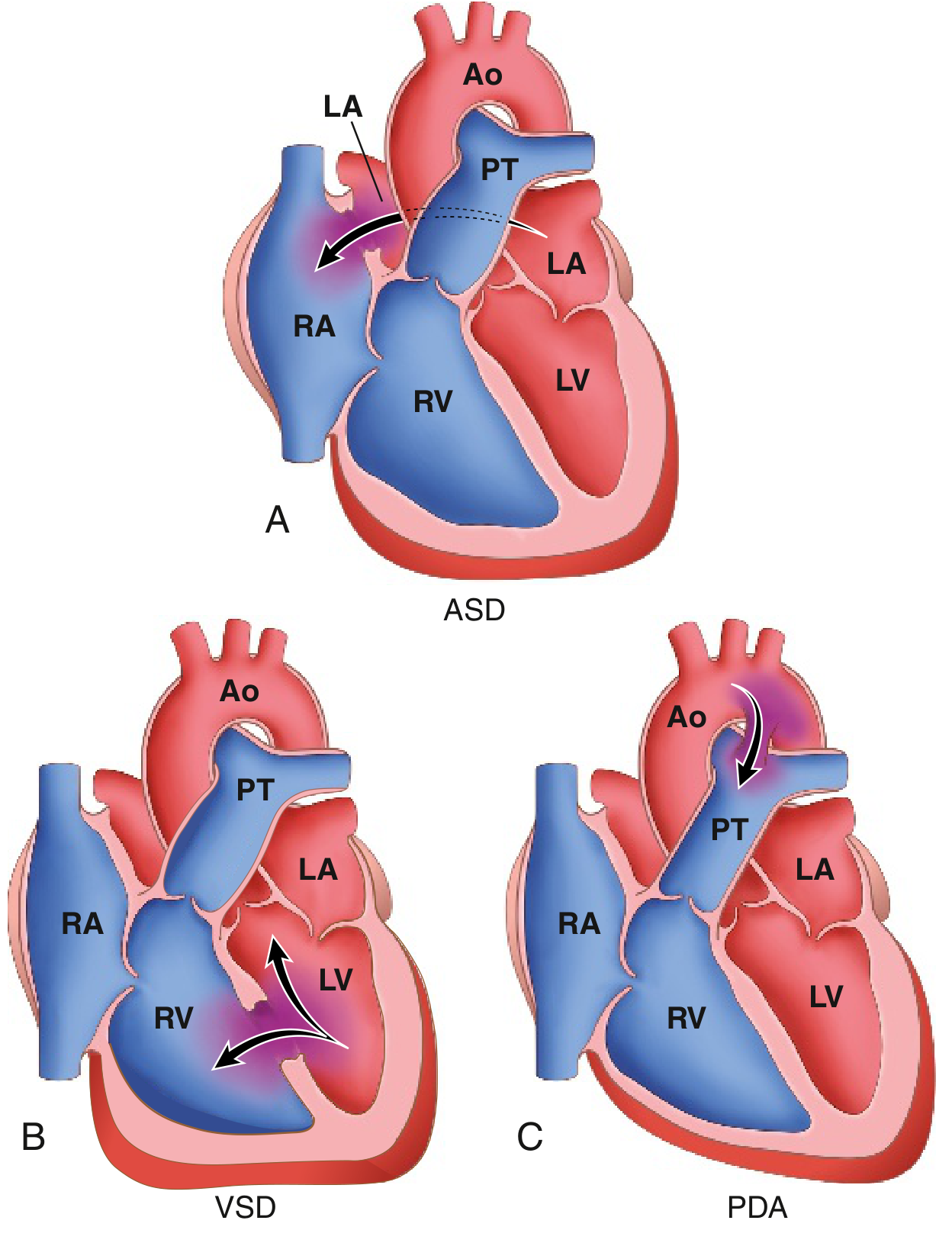
1. Atrial Septal Defect (ASD)
- Abnormal fixed opening in the atrial septum allowing unrestricted blood flow between atria
- Ostium secundum type accounts for ~90% of ASDs - smooth-walled defect near the foramen ovale
- ASDs increase right ventricular and pulmonary outflow volumes
- Contrast with Patent Foramen Ovale (PFO): in 20% of normal individuals the fetal foramen ovale fails to fuse, allowing transient right-to-left flow during straining - can cause paradoxical embolism
- Robbins & Kumar Basic Pathology, p. 348-349
2. Ventricular Septal Defect (VSD)
- Most common congenital heart defect overall
- Causes both increased pulmonary blood flow AND pressure (higher-pressure left-to-right shunt)
- Small VSDs may close spontaneously; large VSDs require surgical or catheter-based closure
- Carries risk of Eisenmenger syndrome if uncorrected
3. Patent Ductus Arteriosus (PDA)
- Failure of the ductus arteriosus (connecting aorta to pulmonary artery in fetal circulation) to close after birth
- Causes aorta-to-pulmonary artery shunting
- Recognized by a classic continuous "machinery" murmur
- Managed with indomethacin (NSAIDs promote closure) or surgical ligation
Acyanotic Obstructive Lesions (no shunt)
- Pulmonary stenosis, aortic stenosis/atresia, and coarctation of the aorta - obstruct blood flow without initial shunting
- Coarctation of aorta: narrowing of the aorta, males affected 2x more often (though females with Turner syndrome frequently have it). Two forms:
- Preductal ("infantile") - hypoplasia of aortic arch proximal to a PDA
- Postductal ("adult") - discrete ridge-like infolding adjacent to the ligamentum arteriosum
- Robbins & Kumar Basic Pathology, p. 350
CYANOTIC (Right-to-Left Shunts) - "The Five Ts"
Cyanotic CHDs cause mixing of deoxygenated and oxygenated blood or direct right-to-left shunting. Clinically apparent cyanosis requires 3-5 mg/dL of deoxygenated hemoglobin (O2 sat ~70-80%). - Tintinalli's Emergency Medicine, p. 862
The five Ts are:
| Disease | Key Feature |
|---|---|
| Tetralogy of Fallot (ToF) | Most common cyanotic CHD after infancy; ~10% of all CHD |
| Transposition of Great Arteries (TGA) | 5-8% of CHD; most common presenting in the newborn period |
| Truncus Arteriosus | Single arterial trunk from both ventricles |
| Tricuspid anomalies | Tricuspid atresia, Ebstein's anomaly |
| Total Anomalous Pulmonary Venous Return (TAPVR) | All pulmonary veins drain into right heart |
Tetralogy of Fallot (ToF)
The four components:
- Large VSD
- Right ventricular outflow obstruction (pulmonic stenosis, valvular or supravalvular)
- Overriding aorta (aorta sits over the VSD)
- Right ventricular hypertrophy
The degree of cyanosis depends on severity of right ventricular outflow obstruction. Severe pulmonic stenosis creates a right-to-left shunt with decreased pulmonary blood flow. The feared complication is "tet spells" - hypercyanotic episodes triggered by crying, feeding, or defecation. Auscultation: loud systolic ejection murmur at lower-left sternal border, loud single S2, aortic ejection click. - Tintinalli's Emergency Medicine, p. 863
Transposition of Great Arteries (TGA)
- Aorta arises from the right ventricle; pulmonary artery from the left ventricle (discordant connection)
- Creates two separate, parallel circulations - incompatible with postnatal life unless a shunt (VSD, PFO, or PDA) allows oxygenated blood to reach the aorta
- VSD present in 1/3 of cases
- Dominant manifestation is cyanosis from birth
- Requires emergent surgical repair within the first few days of life (arterial switch operation)
- Robbins & Kumar Basic Pathology, p. 349
Key Comparison: Acyanotic vs. Cyanotic
| Feature | Acyanotic (L→R shunt) | Cyanotic (R→L shunt) |
|---|---|---|
| Initial cyanosis | Absent | Present from birth |
| Pulmonary blood flow | Increased | Decreased (usually) |
| Risk | Eisenmenger syndrome later | Hypoxia, polycythemia |
| Examples | ASD, VSD, PDA, coarctation | ToF, TGA, truncus arteriosus |
Genetic Associations Worth Noting
- Trisomy 21 (Down syndrome) - ASD, VSD, atrioventricular canal defect
- Turner syndrome (45, X) - Coarctation of aorta, bicuspid aortic valve
- Noonan syndrome - Pulmonary stenosis, hypertrophic cardiomyopathy
- DiGeorge syndrome (22q11 deletion) - Truncus arteriosus, interrupted aortic arch, ToF
- Maternal rubella - PDA, pulmonary artery stenosis, ASD
Sources: Robbins & Kumar Basic Pathology; Tintinalli's Emergency Medicine; Braunwald's Heart Disease
This is a shared conversation. Sign in to Orris to start your own chat.