TEE views complete notes with echo and ecg interrelation
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching the Web
TEE views complete guide 20 standard views echo ECG correlation ASE
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive content. Let me compile the complete notes:
TEE Views - Complete Notes with Echo and ECG Interrelation
Sources: Barash Clinical Anesthesia 9e, Miller's Anesthesia 10e, Textbook of Clinical Echocardiography (Otto)
PART 1: FUNDAMENTALS OF TEE
What is TEE?
Transesophageal echocardiography (TEE) places an ultrasound transducer inside the esophagus and stomach, immediately posterior to the heart. Because no lung or chest wall intervenes between the probe and the heart, TEE produces higher resolution images than transthoracic echocardiography (TTE), especially for posterior structures (left atrium, mitral valve, descending aorta, pulmonary veins).
TEE is the preferred intraoperative modality because it does not interfere with the surgical field. TTE is preferred outside the OR. TEE may be required outside the OR when: body habitus is unfavorable, dressings or drains limit chest-wall access, or the left atrial appendage (LAA) needs direct assessment.
PART 2: PROBE MECHANICS AND IMAGE PLANE ROTATION
The TEE probe tip sits in the esophagus or stomach. The ultrasound crystal array can rotate electronically from 0° through 180°, changing the "cut" through the heart without moving the probe tip.
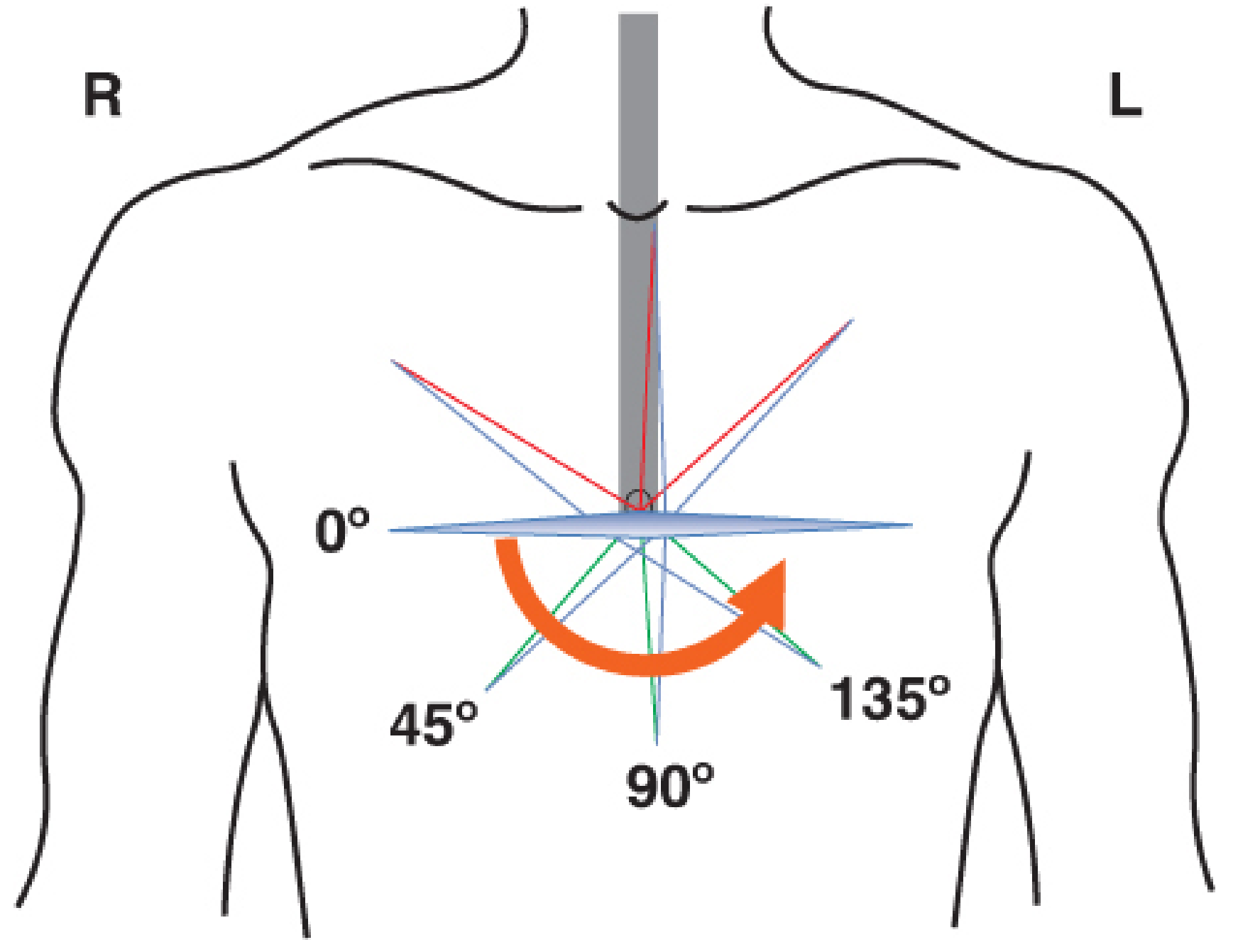
Key angles used clinically:
- 0° = transverse / horizontal plane
- 45° = oblique (RV inflow-outflow)
- 90° = sagittal / vertical plane
- 120-135° = long-axis / oblique
Probe position terminology
| Term | Meaning |
|---|---|
| Advance | Push probe deeper (stomach direction) |
| Withdraw | Pull probe back (mouth direction) |
| Turn left/right | Rotate the whole probe shaft |
| Anteflex / retroflex | Flex tip anteriorly or posteriorly |
| Leflex / rightflex | Flex tip left or right |
Three Primary Positions (ASE/SCA 2013 - 28 views total)
| Position | Depth from teeth | Structures imaged |
|---|---|---|
| Upper esophageal (UE) | ~20-25 cm | Aortic arch, pulmonary artery, SVC |
| Midesophageal (ME) | ~30-40 cm | All four chambers, valves, aortic root |
| Transgastric (TG) | ~40-45 cm | LV cross-section, papillary muscles, LVOT |
| Deep transgastric (dTG) | ~45-50 cm | LVOT, aortic valve, 5-chamber view |
PART 3: COMPREHENSIVE TEE VIEWS (ASE/SCA Guidelines)
The 2013 ASE/SCA guidelines define 28 standard views (expanded from the original 1999 set of 20). The focused "basic" study uses 12 key views as described below.
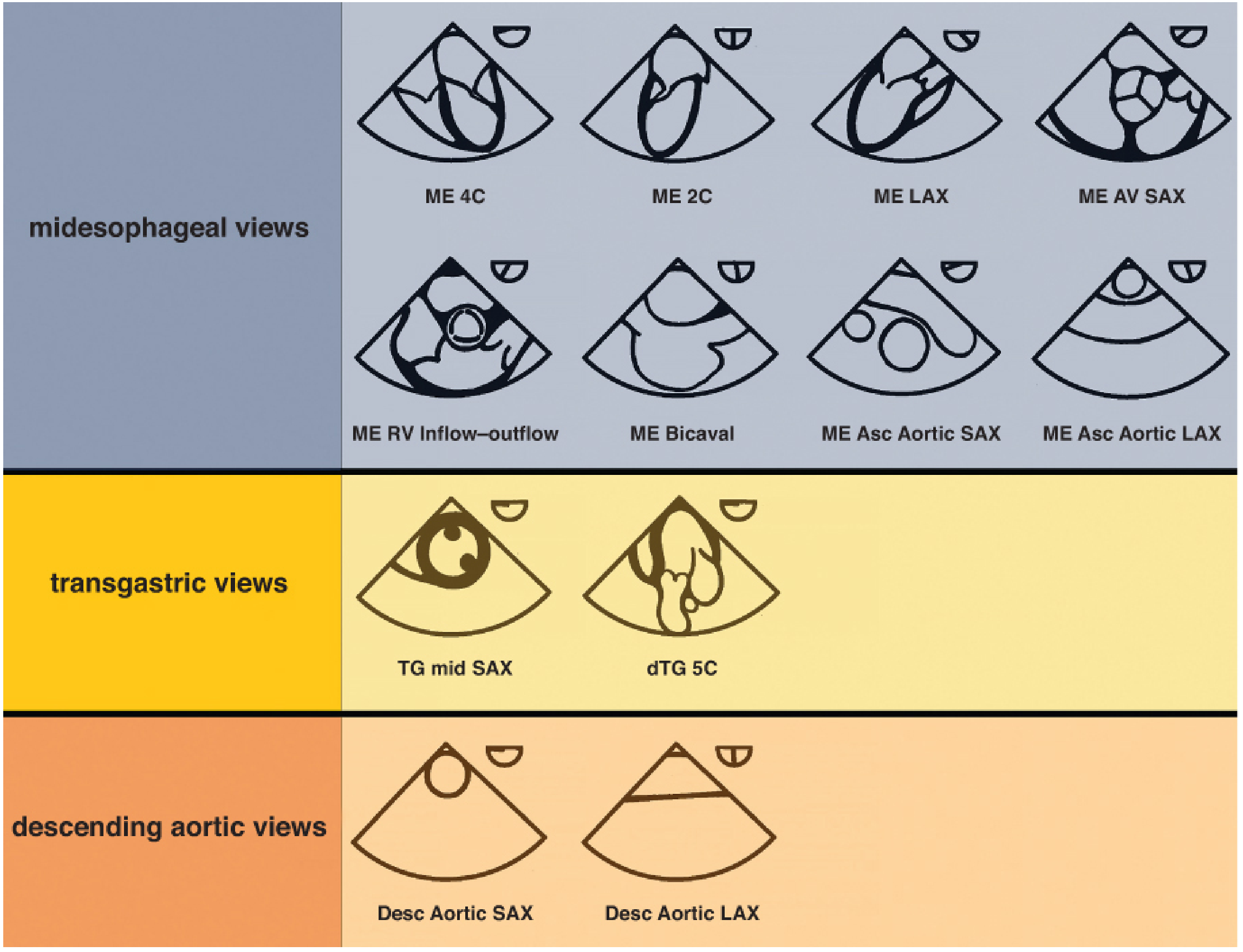
GROUP A: MIDESOPHAGEAL (ME) VIEWS
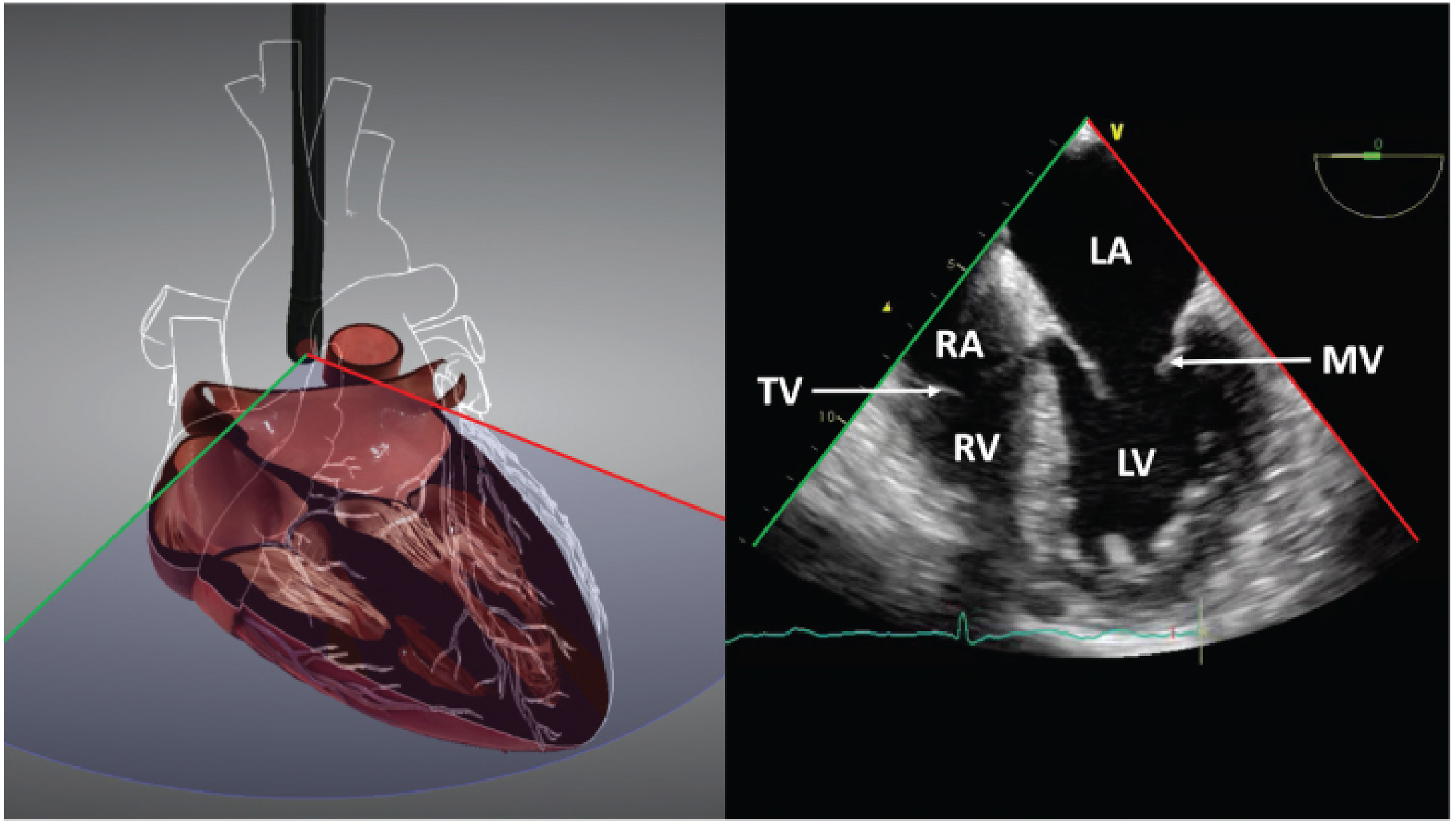
1. ME Four-Chamber View (ME 4C) — 0°
Acquisition: Advance probe 35-40 cm, plane at 0°, retroflex to eliminate foreshortening and open the LV apex.
Structures seen: RA, RV, LA, LV, mitral valve (MV), tricuspid valve (TV), interatrial septum (IAS), interventricular septum (IVS).
Best for:
- Biventricular size and systolic/diastolic function
- LV septal and lateral wall motion
- MV and TV function
- Atrial and ventricular septal integrity
ECG correlation: The QRS onset marks end-diastole (maximum LV cavity size). Peak systolic contraction of all four walls is seen at the T wave end. In the ME 4C view, monitor the septal and lateral walls - these correspond to:
- Lateral wall: left circumflex (LCx) territory → ECG changes in I, aVL, V5-V6
- Septal wall: LAD territory → ECG changes in V1-V4
2. ME Two-Chamber View (ME 2C) — ~90°
Acquisition: From ME 4C, rotate plane to ~90°; turn probe left/right to center LV apex.
Structures seen: LA, LV (inferior and anterior walls), left atrial appendage (LAA), coronary sinus (CS) in inferior AV groove, posteromedial papillary muscle.
Best for:
- LV inferior and anterior wall motion
- LAA thrombus (key pre-cardioversion screen)
- MV in orthogonal plane
ECG correlation:
- Inferior wall: RCA territory → ST elevation in II, III, aVF
- Anterior wall: LAD territory → ST changes in V3-V5
3. ME Long-Axis View (ME LAX) — ~120-135°
Acquisition: From ME 2C, rotate plane to ~120-135°. Equivalent to TTE parasternal long-axis (PLAX).
Structures seen: LA, LV, MV (anterior and posterior leaflets), LVOT, aortic valve (AV), proximal ascending aorta.
Best for:
- LV anterior-septal and inferolateral wall function
- LVOT assessment (dimension for stroke volume calculation)
- Aortic valve morphology and stenosis/regurgitation
- Proximal ascending aorta
ECG correlation:
- Anteroseptal wall: LAD → V1-V4
- Inferolateral (posterior): LCx → I, aVL, V5-V6 or RCA in some patients
4. ME Aortic Valve Short-Axis View (ME AV SAX) — ~30-45°
Acquisition: From ME LAX, withdraw probe slightly and reduce angle to ~30-45°. The AV appears in cross-section as a circle ("Mercedes-Benz" pattern of 3 cusps).
Structures seen: Aortic valve (all 3 cusps: RCC, LCC, NCC), RVOT, pulmonary valve, interatrial septum, proximal coronary ostia, tricuspid valve.
Best for:
- AV morphology (tricuspid vs bicuspid)
- AV orifice area planimetry in AS
- Commissure orientation before TAVR
- RVOT and pulmonary valve assessment
ECG note: AV cusps open at QRS (systole begins) and close at T wave completion.
5. ME Aortic Valve Long-Axis View (ME AV LAX) — ~120-135°
Acquisition: Similar to ME LAX but centered on the AV rather than MV.
Structures seen: LVOT, aortic valve, sinuses of Valsalva, sino-tubular junction, proximal ascending aorta.
Best for:
- Aortic root dimensions
- AI jet characterization
- TAVI planning
6. ME Mitral Commissural View (ME MC) — ~60°
Acquisition: From ME AV SAX, advance probe and increase angle to ~60°.
Structures seen: Both mitral commissures (anterolateral and posteromedial), all three scallops of posterior leaflet visible.
Best for:
- MV commissure pathology
- Mitral stenosis (commissural fusion)
- Pre- and post-mitral repair
7. ME Bicaval View — ~90-110°
Acquisition: From ME 4C, rotate plane to ~90-110° and turn probe rightward.
Structures seen: SVC (top), IVC (bottom), RA, interatrial septum, right pulmonary veins, Eustachian valve, crista terminalis.
Best for:
- Interatrial septum anatomy (ASD, PFO, septal defects)
- Caval cannula positioning (cardiac surgery)
- Catheter/device guidance (ASD closure, TAVR, pacemaker leads)
- Right atrial masses
8. ME RV Inflow-Outflow View — ~60-90°
Acquisition: Rotate plane to ~60-90° and turn probe slightly rightward from ME 4C.
Structures seen: RV inflow (TV), RV body, RVOT, pulmonary valve, proximal pulmonary artery — all in a "wrap-around" view.
Best for:
- RV size and function
- TV and pulmonary valve assessment
- RV outflow tract
- Pericardial effusion (anteriorly)
9. ME Ascending Aortic Short-Axis View (ME Asc Ao SAX) — 0°
Acquisition: Withdraw probe to upper esophagus (~25-30 cm), plane at 0°.
Structures seen: Ascending aorta in cross-section, SVC, pulmonary artery.
10. ME Ascending Aortic Long-Axis View (ME Asc Ao LAX) — ~90-120°
Acquisition: From ME Asc Ao SAX, rotate to 90-120°.
Structures seen: Ascending aorta in longitudinal section.
Best for (both ascending aortic views):
- Aortic dissection (type A)
- Atheroma assessment
- Measurement of ascending aortic diameter
GROUP B: TRANSGASTRIC (TG) VIEWS
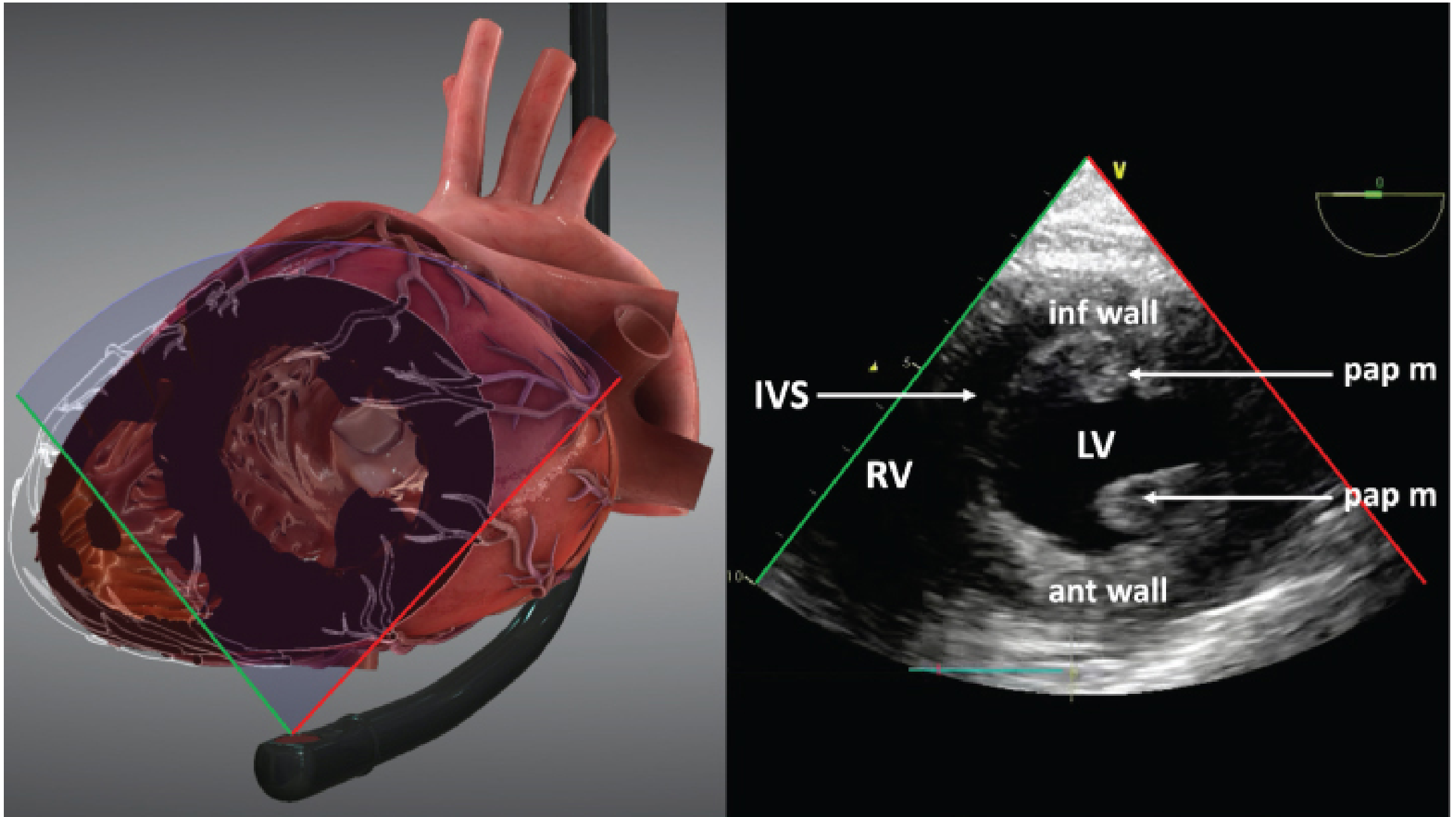
11. TG Mid Short-Axis View (TG Mid SAX) — 0°
Acquisition: Advance probe into stomach (~40-45 cm), anteflex to bring LV into view at 0°. The plane cuts through the LV at the papillary muscle level.
Structures seen: LV (circular cross-section), RV, IVS, anterolateral and posteromedial papillary muscles, all 6 mid LV segments simultaneously.
Best for:
- Global LV systolic function (most important intraoperative monitoring view)
- Regional wall motion abnormalities - all three coronary territories visible simultaneously
- LV preload assessment (end-diastolic area)
- Papillary muscle function
ECG-Echo correlation - CRITICAL VIEW:
The TG Mid SAX is the premier view for real-time ischemia monitoring because all three coronary territories appear simultaneously:
| Wall segment (TG mid SAX) | Coronary artery | ECG leads |
|---|---|---|
| Anterior (top of image) | LAD | V3-V5 |
| Anteroseptal | LAD | V1-V2 |
| Inferior (bottom of image) | RCA | II, III, aVF |
| Inferoseptal | RCA (or LAD) | II, III, V1-V2 |
| Inferolateral / posterior | LCx | I, aVL, V5-V6 |
| Anterolateral | LCx or LAD | I, aVL, V4-V5 |
Key principle: New regional wall motion abnormality (RWMA) on echo precedes ST changes on ECG by approximately 2-4 minutes in experimental ischemia - echo is more sensitive for acute ischemia detection. The sequence is: diastolic dysfunction → systolic dysfunction (RWMA) → ECG changes → symptoms (angina or pain).
12. Deep Transgastric Five-Chamber View (dTG 5C) — 0°
Acquisition: Advance probe fully into stomach (~45-50 cm), maximally anteflex ("deep TG"), plane at 0°.
Structures seen: LV, RV, LA (five-chamber orientation), LVOT, aortic valve, ascending aorta.
Best for:
- CW Doppler through LVOT and aortic valve (best alignment for LVOT VTI and peak aortic velocity)
- Stroke volume calculation
- TAVI post-procedure assessment
- LV outflow tract obstruction (LVOTO)
GROUP C: DESCENDING AORTIC VIEWS
13. Descending Aorta Short-Axis View (Desc Ao SAX) — 0°
Acquisition: From any ME position, turn probe leftward (counterclockwise) until the circular descending aorta appears. At 0°, it appears in cross-section.
14. Descending Aorta Long-Axis View (Desc Ao LAX) — ~90°
Acquisition: From Desc Ao SAX, rotate to ~90°.
Best for (both):
- Aortic dissection (type B)
- Atheroma grading (Grades 1-5 by ASE)
- Aortic aneurysm
- Wire/catheter/IABP placement guidance
UPPER ESOPHAGEAL (UE) VIEWS
15. UE Aortic Arch Long-Axis View — 0°
Acquisition: Withdraw probe to ~20-25 cm, plane at 0°.
Structures seen: Aortic arch in long-axis (horseshoe curve).
16. UE Aortic Arch Short-Axis View — ~90°
Acquisition: From UE LAX, rotate to ~90°.
Structures seen: Aortic arch in cross-section, left subclavian artery, main pulmonary artery, ductus remnant.
17. UE Pulmonary Artery / Pulmonary Vein Views — ~0-90°
Structures seen: Main PA, left PA, right PA, pulmonary veins, SVC, left and right atria.
Best for:
- Pulmonary embolism
- Pulmonary hypertension monitoring
- Pulmonary vein flow for diastolic function
PART 4: THE 17-SEGMENT LV MODEL AND CORONARY TERRITORY MAPPING
The LV is divided into 17 segments (AHA model) - 6 basal, 6 mid, 4 apical, plus apical cap. Each TEE view visualizes a subset of these segments.
| Level | Segments | TEE view |
|---|---|---|
| Basal (6) | Anterior, anteroseptal, inferoseptal, inferior, inferolateral, anterolateral | TG basal SAX, ME views |
| Mid (6) | Same walls at papillary muscle level | TG mid SAX |
| Apical (4) | Anterior, septal, inferior, lateral | ME 4C, ME 2C, ME LAX |
| Apical cap (1) | Apex only | ME views (foreshortened in TEE) |
Coronary Territory to ECG Lead Mapping
| Coronary artery | LV walls supplied | ECG leads |
|---|---|---|
| LAD | Anterior, anteroseptal, apical cap, apical anterior, apical septal | V1-V6 (especially V3-V5) |
| RCA | Inferior (basal), inferoseptal (basal/mid), RV free wall | II, III, aVF |
| LCx | Lateral (all levels), inferolateral | I, aVL, V5-V6 |
Important caveat: There is anatomical variability - the LAD may supply mid-inferoseptal in some, and RCA or LCx may share the inferolateral territory depending on dominance.
PART 5: ECHO-ECG INTERRELATION IN CLINICAL PRACTICE
Timing of Echo Events Relative to ECG
| ECG event | Mechanical correlate seen on echo |
|---|---|
| P wave | Atrial contraction - LA/RA squeeze; mitral valve moves toward LV |
| QRS complex | Onset of ventricular systole - MV closes; semilunar valves open |
| T wave end | End of ventricular repolarization - aortic/pulmonary valve closes |
| Diastole (T to next P) | MV and TV open; ventricular filling begins |
ISOVOLUMIC CONTRACTION (IVC)
- ECG: After QRS onset
- Echo: Mitral valve closed, aortic valve still closed, LV wall thickening beginning
- Timing measured on M-mode
ISOVOLUMIC RELAXATION (IVR)
- ECG: After T wave
- Echo: Both valves closed, LV pressure falling, no filling yet
- Prolonged IVR = impaired relaxation (Grade I diastolic dysfunction)
Diastolic Function - Echo-ECG Timing
Doppler of mitral inflow (pulsed wave, sampled at MV tips):
- E wave = early passive filling (corresponds to rapid ventricular relaxation after T wave)
- A wave = late active filling (corresponds to P wave of next beat - atrial contraction)
| Diastolic grade | E/A ratio | DT (ms) | IVRT (ms) | Echo finding | ECG association |
|---|---|---|---|---|---|
| Normal | 1-2 | 160-200 | 60-100 | Normal | Normal |
| Grade I (impaired relaxation) | <1 | >200 | >100 | Reduced E, dominant A | LVH on ECG, strain pattern |
| Grade II (pseudonormal) | 1-2 | 160-200 | 60-100 | PV S<D; E/e'>14 | Often LVH |
| Grade III (restrictive) | >2 | <160 | <60 | High E, no A | Tall P waves, AF common |
ST Changes and RWMA Correlation
Echo is more sensitive than ECG for ischemia. The cascade of ischemia:
- Metabolic change (lactate, adenosine)
- Diastolic dysfunction (impaired LV relaxation on TDI/echo - first sign)
- Systolic dysfunction (RWMA on echo - wall becomes hypokinetic, then akinetic)
- ECG changes (ST depression/elevation)
- Symptoms (angina)
This means in the operating room or ICU, a new RWMA on TG mid SAX precedes ST changes on the ECG monitor - giving earlier warning of ischemia.
Grading of Regional Wall Motion
| Grade | Description | ECG likelihood |
|---|---|---|
| Normal/hyperkinetic | >30% systolic thickening | No ischemic changes |
| Hypokinetic | Reduced thickening (10-30%) | May have subtle ST changes |
| Akinetic | No/minimal thickening (<10%) | ST changes usually present |
| Dyskinetic | Paradoxical outward motion | Marked ECG changes/STEMI pattern |
Conduction Abnormalities on ECG Affecting Echo Interpretation
| ECG abnormality | Echo finding |
|---|---|
| LBBB | Paradoxical septal motion (septum moves opposite to normal); may mimic RWMA; speckle tracking needed |
| RBBB | Septal motion abnormal (early); RV enlargement may be seen |
| Paced rhythm | Dyskinetic septal motion due to abnormal activation sequence |
| AF | No A wave on mitral Doppler; LAA thrombus risk |
| 1st degree AV block | Prolonged PR → prolonged E-A fusion; elevated LV filling pressures |
| Complete heart block | Cannon A waves on tricuspid/mitral Doppler (atria contracting against closed valves) |
| WPW | Pre-excitation → regional wall motion artifact mimicking RWMA |
PART 6: FOCUSED TRANSTHORACIC ECHO VIEWS (FoCUS) for Comparison
The five standard FoCUS views correlate with TEE views:
| TTE View | TEE Equivalent | Probe Window |
|---|---|---|
| Parasternal long-axis (PLAX) | ME LAX (~120-135°) | 3rd-5th ICS, left sternal border |
| Parasternal short-axis (PSAX) | TG mid SAX (0°) | Same as PLAX, probe rotated 90° |
| Apical four-chamber (A4C) | ME 4C (0°) | 5th ICS, mid-axillary line |
| Subcostal four-chamber (S4C) | No direct equivalent | Sub-xiphoid |
| Subcostal IVC (SIVC) | ME Bicaval (~90°) | Sub-xiphoid |
PART 7: SPECIAL APPLICATIONS WITH ECHO-ECG RELEVANCE
Stress Echocardiography
Stress echo (dobutamine or exercise) is particularly valuable when the resting ECG is non-diagnostic (LBBB, paced rhythm, LVH with repolarization changes, pre-excitation). Echo detects new or worsening RWMA as the ischemic endpoint, independent of ECG changes.
Cardiac Arrhythmias Assessment by TEE
- AF: ME Bicaval and ME 2C views to visualize LAA for thrombus before cardioversion
- VT storms: Assess LV function and look for structural substrate (scar = akinetic/dyskinetic segment correlating with Q waves on ECG)
- Sinus node dysfunction: No structural abnormality usually; RA size may be increased
Pulmonary Hypertension
- ECG: RAD, RVH (R>S in V1), P pulmonale, RBBB
- Echo: RV enlargement (>2/3 LV size in ME 4C), D-shaped septum in diastole (volume overload) or throughout cardiac cycle (pressure overload), TR jet velocity >3.4 m/s (estimated RVSP >50 mmHg)
Cardiac Tamponade
- ECG: Low voltage, electrical alternans (alternating QRS amplitude)
- Echo: RA collapse in systole, RV diastolic collapse, IVC plethora (no collapse with inspiration), "swinging heart"
Aortic Stenosis
- ECG: LVH pattern (Sokolow criteria), strain pattern (ST depression, T inversion in V5-V6, I, aVL)
- Echo: Reduced AV cusp excursion in ME AV SAX; high velocity jet (>4 m/s by CW Doppler from dTG 5C); mean gradient >40 mmHg = severe
PART 8: SYSTEMATIC TEE EXAMINATION SEQUENCE
Recommended order (depth-based, ASE):
- ME 4C → biventricular function, MV, TV, septa
- ME 2C → inferior/anterior walls, LAA
- ME LAX → LVOT, AV, MV in orthogonal plane
- ME AV SAX → AV morphology, RVOT, coronary ostia
- ME AV LAX → aortic root dimensions
- ME MC → MV commissures
- ME Bicaval → IAS, SVC, IVC, right PV
- ME RV inflow-outflow → RV, TV, RVOT, pulmonary valve
- ME Asc Ao SAX/LAX → ascending aorta
- TG mid SAX → LV function monitor, RWMA
- TG 2C or TG LAX → LV walls in additional planes
- dTG 5C → Doppler of LVOT/AV
- Desc Ao SAX + LAX → aorta from arch to celiac
- UE Asc Ao / Arch views → arch, great vessels
PART 9: KEY MEMORY TRICKS
| View | Angle | Mnemonic |
|---|---|---|
| ME 4C | 0° | "Zero = Four" (0° gives 4 chambers) |
| ME 2C | 90° | "90 = Two" (rotate 90° → 2 chambers) |
| ME LAX | 120-135° | "120-135 = Long" |
| ME AV SAX | 30-45° | "30-45 = Aorta X-section" |
| ME Bicaval | 90-110° | "90 + right turn = bicaval" |
| TG Mid SAX | 0° in stomach | "Stomach, zero, circle" |
| dTG 5C | 0° deep stomach | "Deepest, 0°, five chambers" |
SUMMARY TABLE: ALL 12 FOCUSED TEE VIEWS
| # | View | Angle | Depth | Key Structures | Coronary / ECG relevance |
|---|---|---|---|---|---|
| 1 | ME 4C | 0° | 35-40 cm | LA, RA, LV, RV, MV, TV | Lateral (LCx) + Septal (LAD) |
| 2 | ME 2C | ~90° | 35-40 cm | LA, LV (inf/ant), LAA | Inferior (RCA) + Anterior (LAD) |
| 3 | ME LAX | 120-135° | 35-40 cm | LV, LVOT, MV, AV, aorta | Anteroseptal (LAD) + Inferolateral (LCx) |
| 4 | ME AV SAX | 30-45° | 30-35 cm | AV cusps, RVOT, PV, IAS | AV timing with QRS |
| 5 | ME AV LAX | 120-135° | 30-35 cm | Aortic root, LVOT | Aortic root pathology |
| 6 | ME MC | ~60° | 35 cm | MV commissures | MV lesion localization |
| 7 | ME Bicaval | 90-110° | 30-35 cm | SVC, IVC, RA, IAS | RAD on ECG → check RV |
| 8 | ME RV I/O | 60-90° | 30-35 cm | RV, TV, RVOT, PV | RVH/RBBB on ECG |
| 9 | ME Asc Ao SAX | 0° | 25-30 cm | Ascending aorta (XS) | Aortic dissection |
| 10 | ME Asc Ao LAX | ~90° | 25-30 cm | Ascending aorta (long) | Aortic dissection |
| 11 | TG mid SAX | 0° | 40-45 cm | LV (all 6 mid segments), RV | All 3 coronary territories - primary ischemia monitor |
| 12 | dTG 5C | 0° | 45-50 cm | LV, LVOT, AV, aorta | Doppler LVOT VTI, AV velocity |
References: Barash Clinical Anesthesia 9e, p. 2201-2215; Miller's Anesthesia 10e, p. 4982-4990; Textbook of Clinical Echocardiography (Otto), p. 112; ASE/SCA 2013 Guidelines for Comprehensive TEE Examination.
This is a shared conversation. Sign in to Orris to start your own chat.