Blumer shelf
Reading File
Searching the Web
Blumer shelf sign rectal examination clinical significance
Finding Sources
Reading Web Page
https://en.wikipedia.org/wiki/Blumer%27s_shelf
Reading File
Reading File
Here is a complete summary of the Blumer shelf (also written as Blumer's shelf or "rectal shelf of Blumer"):
Blumer's Shelf (Rectal Shelf of Blumer)
What it is
Blumer's shelf is a palpable finding on digital rectal examination (DRE) - or sometimes vaginal examination - consisting of hard, shelf-like nodularity felt anteriorly and extraluminally in the anterior rectal wall. It indicates that tumor has metastasized to the pouch of Douglas (rectouterine pouch in females, rectovesical pouch in males).
Mechanism
Metastatic tumor cells from an abdominal cancer "drop" by gravity through the peritoneal cavity and implant in the most dependent peritoneal recess - the pouch of Douglas. Over time these deposits grow into a firm, palpable mass that can be felt on rectal (or vaginal) exam as a hard, shelf-like protrusion anteriorly above the prostate or cervix.
Associated Cancers
Most commonly a sign of:
- Gastric carcinoma (the classic and most common cause)
- Pancreatic carcinoma
- Lung carcinoma
- Colorectal carcinoma (direct spread or drop metastases)
It is also associated with any abdominal malignancy capable of peritoneal spread.
Clinical Context - Signs of Advanced/Incurable Disease
Blumer's shelf belongs to a constellation of physical findings that indicate advanced, typically incurable disease in gastric cancer. These include:
- Sister Joseph's nodule - periumbilical lymph node metastasis
- Virchow's node - left supraclavicular node (Troisier's sign)
- Krukenberg tumor - ovarian metastasis
- Blumer's shelf - pouch of Douglas metastasis (rectal shelf)
As stated in Schwartz's Principles of Surgery: "Physical examination typically is normal. Other than signs of weight loss, specific positive physical findings usually indicate incurability." - Schwartz's Principles of Surgery, 11th Ed.
And from Sleisenger and Fordtran's Gastrointestinal and Liver Disease: "Other sites of spread include periumbilical lymph nodes (Sister Joseph nodule), left supraclavicular sentinel nodes (Virchow node), the pouch of Douglas (rectal shelf of Blumer), and the ovaries (Krukenberg tumor)." - Sleisenger & Fordtran's GI and Liver Disease
Diagnostic Value
- Low sensitivity for detecting peritoneal metastases (many cases are missed on DRE)
- High specificity - a positive finding strongly suggests peritoneal carcinomatosis
- The sign is a clinical shortcut; modern staging uses CT/MRI/PET and diagnostic laparoscopy, which are far more sensitive
- A positive Blumer's shelf typically changes management by confirming M1 disease (peritoneal metastasis = Stage IV), making curative resection unlikely
Eponym
Named after George Blumer (1858-1940), an American physician who described the sign in the context of rectal palpation in patients with gastric and pelvic malignancies.
Signs and symptoms of peptic perforation and it’s management
Finding Sources
Searching the Web
peptic ulcer perforation signs symptoms management 2024
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have everything needed. Here is a comprehensive, textbook-sourced answer:
Perforated Peptic Ulcer - Signs, Symptoms & Management
Epidemiology
Despite widespread use of PPIs and H. pylori eradication therapy, the incidence of perforated peptic ulcer has changed little. There has been a steady shift toward elderly female patients, with NSAIDs implicated as the predominant cause. Most perforations are anterior duodenal ulcers. - Bailey & Love's Short Practice of Surgery, 28th Ed.
Signs and Symptoms
Onset
- Sudden, excruciating abdominal pain - the patient can often give the exact time of onset; classically described as "a blow to the stomach"
- Pain is initially epigastric, rapidly becoming generalised as gastric/duodenal contents spread through the peritoneal cavity
- May be preceded by a history of peptic ulcer disease or NSAID use
Peritoneal Irritation (Chemical, then Bacterial)
- Initially a chemical peritonitis from gastric acid and duodenal secretions
- Within hours, bacterial peritonitis supervenes, with clinical deterioration
- Board-like (rigid) abdomen - the hallmark sign; involuntary guarding
- Rebound tenderness on gentle examination
- Abdomen does not move with respiration
- Patient lies still and is reluctant to move due to pain
Systemic Features
- Tachycardia and signs of shock early on
- Pyrexia - usually appears hours after the event (not at onset)
- Nausea and vomiting - not a prominent feature (once or twice at most)
- Fluid sequestration into the third space of inflamed peritoneum can be significant
Atypical Presentations
- Elderly patients and those on steroids may present with a less dramatic picture - reduced rigidity, blunted pain response
- Fluid tracking down the right paracolic gutter can mimic acute appendicitis (pain in epigastrium AND right iliac fossa)
- Some perforations seal spontaneously (sealed perforation), presenting with gradually settling pain
"The classical presentation of perforated duodenal ulcer is instantly recognisable... The abdomen exhibits a board-like rigidity, and the patient is disinclined to move because of the pain." - Bailey & Love, 28th Ed.
Investigations
| Investigation | Finding |
|---|---|
| Erect CXR | Free gas under diaphragm in ~50-80% of cases |
| CT abdomen (gold standard) | Free intraperitoneal air, fluid - most accurate |
| Serum amylase | May be mildly elevated (not as high as pancreatitis) |
| FBC, U&E, LFTs, Group & Save | Baseline; assess for infection and metabolic derangement |
| Urine pregnancy test | Women of childbearing age |
Erect CXR showing free air under the right diaphragm in a perforated duodenal ulcer:
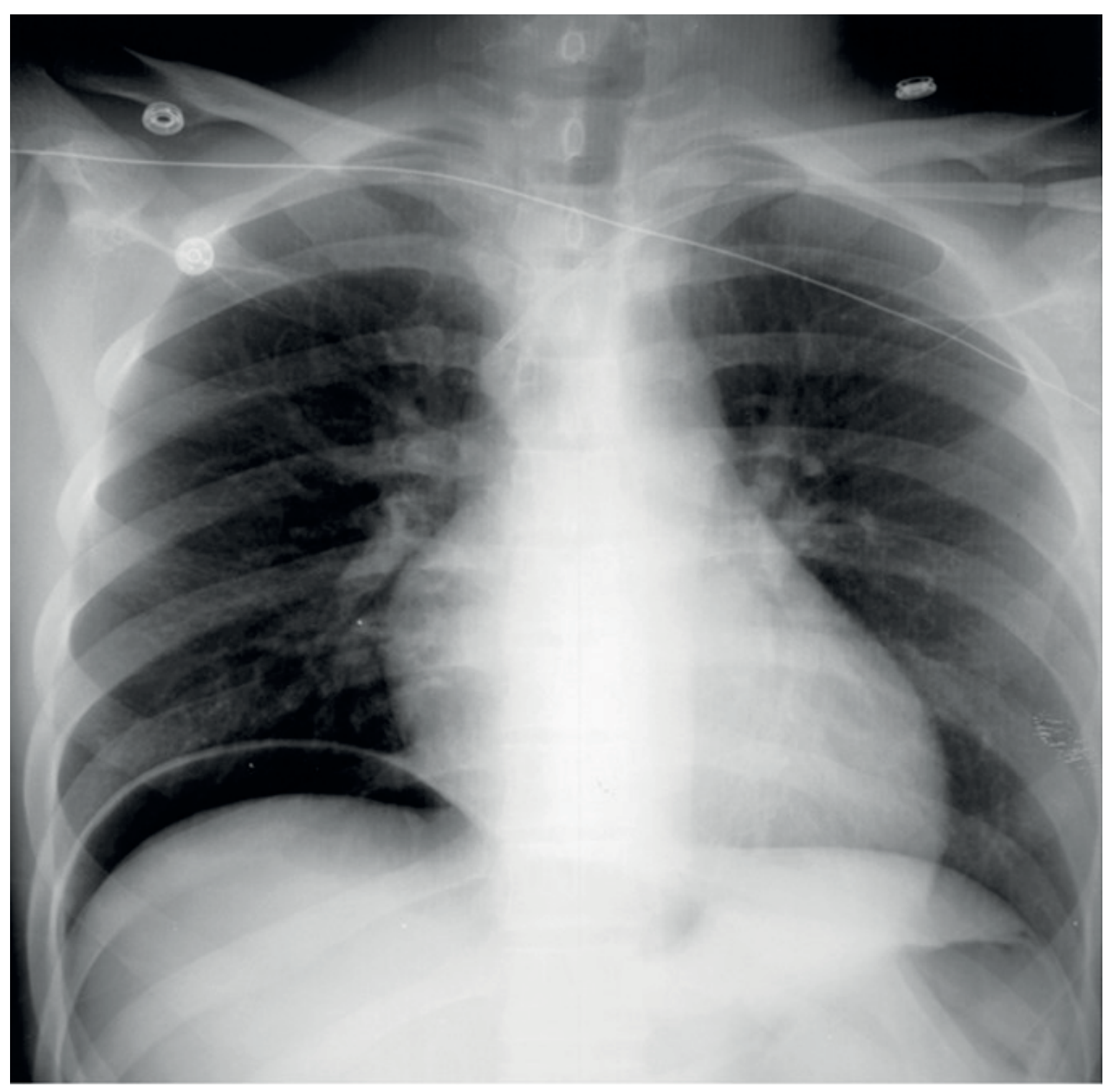
Note: Serum amylase can be elevated after peptic perforation but levels are not usually as high as in acute pancreatitis; CT usually differentiates both. - Bailey & Love
Management
Step 1: Immediate Resuscitation (All Patients)
- IV access + aggressive fluid resuscitation with isotonic fluids (third-space losses can be massive)
- IV analgesia - do NOT withhold; adequate analgesia actually makes signs clearer, not obscures them
- IV broad-spectrum antibiotics
- Nasogastric tube (decompress stomach, keep empty)
- Urinary catheter (monitor urine output)
- IV PPI (omeprazole/pantoprazole)
- NPO (nil by mouth)
Step 2: Operative Management (Majority of Cases)
Surgery is the treatment of choice in nearly all cases of perforated peptic ulcer.
Approaches:
- Laparoscopy (preferred if expertise available) - lower wound infection, less analgesic requirement, shorter hospital stay, faster return to activity; mortality equivalent to open
- Open laparotomy (upper midline incision) - when laparoscopy not feasible
Operative Steps:
- Thorough peritoneal toilet - most important step; remove all fluid, food debris, and gastric content
- Closure of perforation:
- Duodenal perforation: Close with sutures in transverse direction (pyloroplasty fashion); reinforce with an omental (Graham) patch
- When primary closure is difficult, omental patch alone can seal the leak
- Gastric ulcer perforation: Excise and close if possible - to exclude malignancy
- Massive perforation not amenable to simple closure: Distal gastrectomy + Roux-en-Y reconstruction
"The most important component of the operation is a thorough peritoneal toilet to remove all of the fluid and food debris." - Bailey & Love, 28th Ed.
"Current reports advocate omental patch closure, often laparoscopically, with postoperative anti-H. pylori therapy." - Mulholland & Greenfield's Surgery, 7th Ed.
Step 3: Postoperative Care
- Nasogastric suction to keep stomach empty
- IV PPI / oral PPI as soon as tolerating - promote ulcer healing
- H. pylori eradication - MANDATORY; ~80% of perforated peptic ulcers are H. pylori positive; without eradication, up to 80% recur and 10% reperforate
- Monitor for complications (leak, abscess, ileus)
Non-Operative (Conservative) Management
Appropriate only in a minority of carefully selected patients:
- Small leak with relatively mild peritoneal contamination
- Radiologic evidence (contrast study) that the perforation has already sealed
- Absence of clinical peritonitis
- Regimen: IV fluids, NGT suction, IV antibiotics, IV PPI
- Any deterioration = immediate surgery
"Nonoperative management is appropriate only if there is objective evidence that the leak has sealed (i.e., radiologic contrast study), and in the absence of clinical peritonitis." - Schwartz's Principles of Surgery, 11th Ed.
Prognostic Factors / Mortality Predictors
Mortality correlates most strongly with:
- Preoperative shock
- Coexisting medical illness
- Perforation present for >48 hours before surgery (surgical delay is a critical determinant)
- ASA score
- PULP score (Peptic Ulcer Perforation score)
Long-term Management After Recovery
-
H. pylori test and treat (if not done at surgery)
-
PPI long-term - especially if NSAID use must continue
-
Stop NSAIDs or switch to a COX-2 inhibitor + PPI
-
Patients who have perforated once are at risk of reperforaiton - aggressive secondary prevention is essential
-
Bailey & Love's Short Practice of Surgery, 28th Ed.
-
Schwartz's Principles of Surgery, 11th Ed.
-
Mulholland & Greenfield's Surgery, 7th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.