Acute pte evaluation
Reading File
Finding Sources
Searching PubMed
"pulmonary embolism"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive, well-illustrated answer. Here is the full response:
Acute Pulmonary Thromboembolism (PTE) - Evaluation
Overview
PE can present anywhere on a spectrum from asymptomatic to sudden cardiovascular collapse. Evaluation follows a structured pathway: recognize suspicion → estimate pretest probability (PTP) → selective testing → imaging when indicated → risk stratify the confirmed diagnosis.
1. Clinical Presentation
The clinical presentation is highly variable. Any ED visit involving dyspnea, chest pain, palpitations, syncope, or unexplained malaise could represent PE - but this does not mean every such patient requires full workup.
| Symptom | Frequency in PE |
|---|---|
| Dyspnea | 75-80% (most common) |
| Chest pain (pleuritic or vague) | ~67% |
| Cough / hemoptysis | Less common; suggests pulmonary infarction |
| Unilateral leg swelling | <30%, but relatively specific when present |
| Syncope | <5% of syncope patients have PE, but it can be the sole presentation |
| Fever | Usually low-grade; >38.6°C suggests infection instead |
Key point: the most common symptom (dyspnea) is absent in 20-25% of patients with PE. Do not rule out PE simply because a classic symptom is missing. - Rosen's Emergency Medicine, 9e
2. Step 1 - Determine Pretest Probability (PTP)
This is the single most important first step. It determines whether and what testing is needed.
Wells Score for PE
| Clinical Feature | Points |
|---|---|
| Previous PE or DVT | 1.5 |
| Heart rate >100 bpm | 1.5 |
| Recent surgery or immobilization (within 4 weeks) | 1.5 |
| Clinical signs of DVT (calf swelling/tenderness) | 3 |
| Hemoptysis | 1 |
| Active cancer (treated within 6 months or palliative) | 1 |
| Alternative diagnosis less likely than PE | 3 |
Interpretation:
- Score 0-1: Low probability (~3-5%)
- Score 2-6: Moderate probability (~20-30%)
- Score >6: High probability (~60-80%)
- Binary: ≤4 = PE unlikely; >4 = PE likely
Note: The "alternative diagnosis" criterion gives this tool a subjective element that empowers clinical judgment - this is a feature, not a bug. - Rosen's Emergency Medicine, 9e
Revised Geneva Score (fully objective - no subjective items)
Includes: age >65, prior DVT/PE, surgery/fracture <1 month, active cancer, unilateral lower limb pain, hemoptysis, HR 75-94 or ≥95, pain on deep palpation of lower limb + unilateral edema.
Gestalt
Unstructured clinical gestalt (low <15%, moderate 15-40%, high >40%) is also validated and may actually be the most accurate method among experienced clinicians.
3. Step 2 - Diagnostic Algorithm
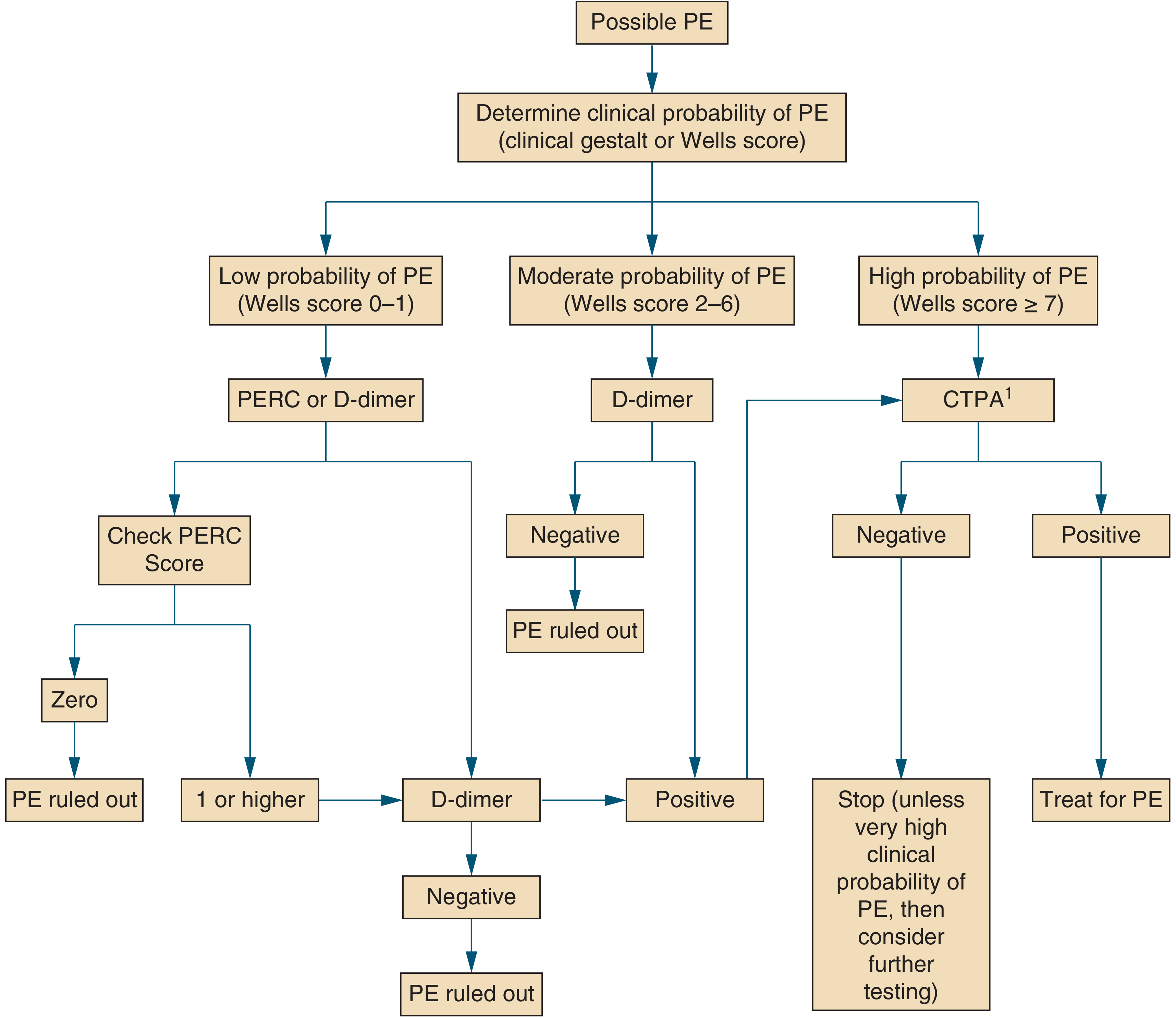
Fig. Proposed algorithm for evaluation of suspected PE - Symptom to Diagnosis, 4e
PERC Rule (PE Rule-Out Criteria)
For patients with low gestalt PTP, apply PERC. If all 8 criteria are met (score = 0), PE can be excluded without further testing:
- Age < 50
- Pulse < 100
- SpO2 > 94%
- No unilateral leg swelling
- No hemoptysis
- No recent trauma or surgery
- No prior PE/DVT
- No hormone use (OCP/HRT)
ACEP, ACP, and ASH guidelines all endorse the PERC rule. - Tintinalli's Emergency Medicine, 9e
4. Step 3 - D-Dimer Testing
D-dimer is a sensitive but non-specific screening test. It works by detecting fibrin degradation products from clot lysis.
- Sensitivity: 95-98% for PE
- Specificity: 40-55%
- NPV: 99-100% when PTP is low-to-moderate
Use D-dimer when PTP is non-high (Wells ≤6 or gestalt <40%). A negative result excludes PE without imaging.
Age-Adjusted D-Dimer Threshold
Standard cutoff: 500 ng/mL. In patients ≥50 years, use:
Age × 10 ng/mL as the threshold for positivity
This increases the proportion of patients who avoid CTPA by 10-20% in those >70 years, while maintaining >95% sensitivity. - Rosen's Emergency Medicine, 9e
YEARS Algorithm
Uses 3 questions (DVT signs, hemoptysis, PE most likely diagnosis):
- 0 YEARS criteria: D-dimer threshold raised to 1000 ng/mL
- ≥1 YEARS criteria: use standard 500 ng/mL threshold
- Validated in multicenter study; reduced CTPA by 14%. Also adapted for pregnancy.
Causes of False-Positive D-Dimer
Age >70, pregnancy, active malignancy, surgery within prior week, liver disease, rheumatoid arthritis, infections, trauma.
Causes of False-Negative D-Dimer
Symptoms >5 days, small clots, isolated calf thrombosis, lipemia, subacute/chronic PE.
5. Step 4 - Pulmonary Vascular Imaging
Order imaging when PTP is high or D-dimer is positive.
CT Pulmonary Angiography (CTPA) - First-Line
- Sensitivity/Specificity: 90-95% on multidetector CT
- PE appears as hypodense filling defects in contrast-opacified pulmonary arteries
- "Saddle PE" = clot straddling the bifurcation of main pulmonary arteries
- PE described by most proximal location (main, lobar, segmental, subsegmental)
- "Massive PE" is a physiologic/hemodynamic diagnosis, not a CT-size diagnosis; preferred term is "high-risk PE"

Axial CTPA showing circular filling defect in right middle lobar pulmonary artery (arrowheads) and segmental artery filling defect (arrow) - Tintinalli's Emergency Medicine, 9e
V/Q Scan
- Alternative to CTPA (preferred in: pregnancy, contrast allergy, renal failure)
- Normal perfusion scan: ~100% sensitive for excluding PE
- High-probability result (≥2 wedge-shaped defects with normal ventilation): >80% probability of PE
- All other results are non-diagnostic
- V/Q SPECT has pooled sensitivity 96%, specificity 97% - superior to planar V/Q
Bedside Ultrasound
- DVT found on lower limb US = equivalent to a PE diagnosis → initiate treatment
- Emergency physician-performed: 86-96% sensitive, 93-97% specific vs. radiology US
- Negative US does NOT exclude PE (fewer than 50% of PE patients have detectable DVT)
- Point-of-care echo: RV:LV ratio >1:1 in diastole raises suspicion for PE (and worsens prognosis)
MRI
- Zero radiation - considered for pregnant patients
- Pooled sensitivity ~75%, specificity ~80% → not first-line
6. ECG Findings in Acute PE
ECG is non-specific but can provide supportive evidence, especially for high-risk PE:
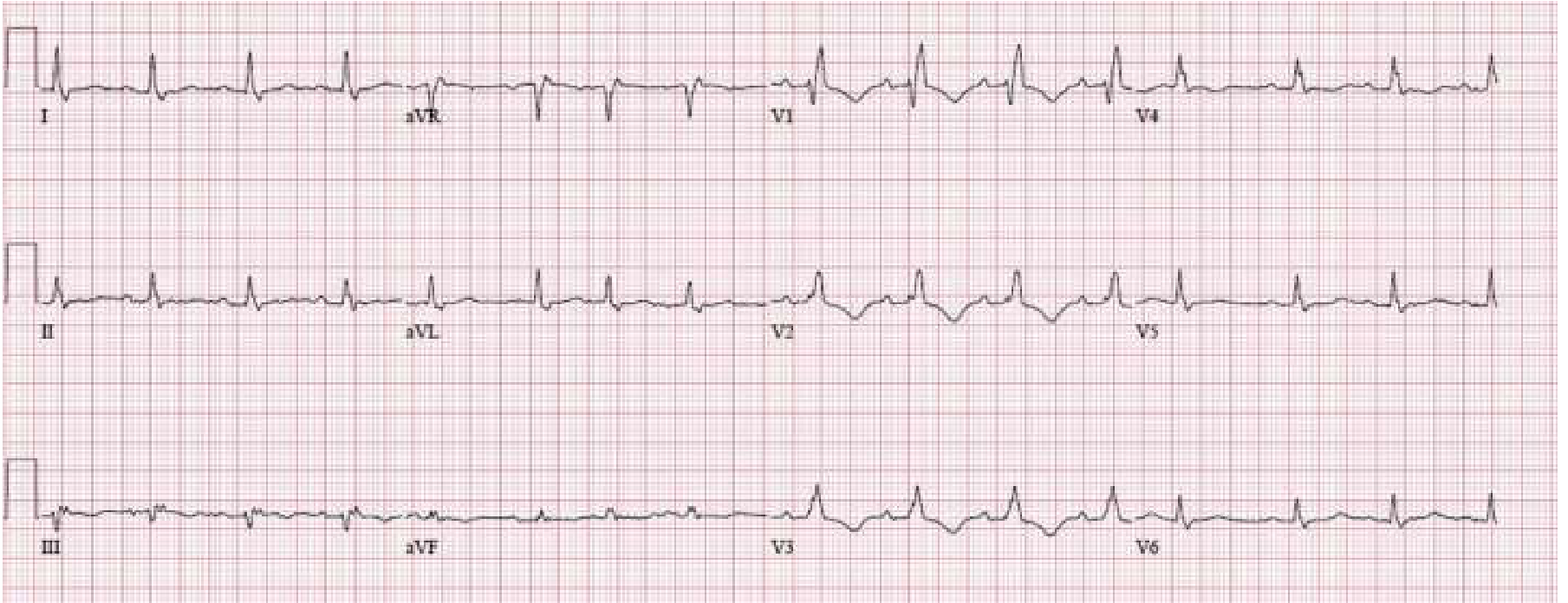
ECG showing S1Q3T3 pattern, new complete RBBB, and deep T-wave inversions V1-V3 - signs of acute RV strain/cor pulmonale. These findings indicate right ventricular dysfunction and carry poor prognosis. - Rosen's Emergency Medicine, 9e
Common ECG findings in PE (none pathognomonic):
- Sinus tachycardia (most common)
- S1Q3T3: S wave in lead I, Q wave and T-wave inversion in lead III
- New RBBB
- T-wave inversions V1-V4
- Right axis deviation
7. Risk Stratification of Confirmed PE
Once PE is confirmed, risk stratify to guide management:
AHA/ESC Classification
| Category | Definition | 30-day Mortality |
|---|---|---|
| High-Risk (Massive) | Hemodynamically unstable (SBP <90, or drop ≥40 mmHg for >15 min, or need for vasopressors) | 15-50% |
| Intermediate-Risk (Submassive) | Hemodynamically stable + RV dysfunction (echo/CTPA) and/or elevated troponin/BNP | 3-15% |
| Low-Risk | Hemodynamically stable, no RV dysfunction, normal biomarkers | <1-3% |
PESI and Simplified PESI (sPESI)
The PESI is the most extensively validated tool for predicting 30-day mortality:
| Predictor | Original PESI | sPESI |
|---|---|---|
| Age | Age in years | +1 if >80 |
| Male sex | +10 | - |
| Cancer | +30 | +1 |
| Heart failure | +10 | +1 (combined) |
| Chronic lung disease | +10 | (combined) |
| HR ≥110/min | +20 | +1 |
| SBP <100 mmHg | +30 | +1 |
| RR ≥30/min | +20 | - |
| Temp <36°C | +20 | - |
| Altered mental status | +60 | - |
| SpO2 <90% | +20 | +1 |
PESI Classes:
- Class I (≤65 pts): 0-1.6% mortality (very low)
- Class II (66-85): 1.7-3.5% (low)
- Class III (86-105): 3.2-7.1% (moderate)
- Class IV (106-125): 4-11.4% (high)
- Class V (>125): 10-24.5% (very high)
sPESI = 0: Low risk. sPESI ≥1: High risk. - Sabiston Textbook of Surgery, 7e
Biomarkers for Risk Stratification
- Troponin I/T: RV myocardial injury marker; elevated = worse prognosis even in hemodynamically stable patients
- BNP/NT-proBNP: RV pressure overload marker; elevated = unfavorable prognosis
- Echo findings: RV:LV ratio >1.0, TAPSE <15 mm = poor prognosis
8. Risk Stratification → Treatment Matrix
| Risk | Criteria | Action |
|---|---|---|
| Low | Hemodynamically stable, no RV dysfunction | DOAC (preferred), consider discharge (Hestia criteria) |
| Intermediate-low | Stable + PESI high + troponin negative | Anticoagulate, admit, monitor |
| Intermediate-high | Stable + RV dysfunction + troponin positive | Anticoagulate (heparin), activate PERT, monitored bed/ICU, consider thrombolysis |
| High | Hemodynamically unstable | UFH, PERT activation, systemic thrombolysis or thromboembolectomy, ICU |
PERT (Pulmonary Embolism Response Team): Multidisciplinary team activated for intermediate-high and high-risk PE; includes emergency medicine, pulmonology, cardiology, and cardiac surgery. - Rosen's Emergency Medicine, 9e
Quick Reference Summary
Possible PE?
↓
Assess PTP (Wells / Gestalt)
↓
Low PTP → PERC: all 0? → Stop (no PE)
≥1? → D-dimer
↓
Moderate PTP → D-dimer
Negative → PE excluded
Positive → CTPA
↓
High PTP → CTPA directly
↓
CTPA positive → Risk stratify (hemodynamics + RV + troponin + PESI)
→ Treat accordingly
Sources: Rosen's Emergency Medicine 9e | Tintinalli's Emergency Medicine 9e | Sabiston Textbook of Surgery 7e | Symptom to Diagnosis 4e | Murray & Nadel's Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.