E CT explain briefly
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have enough information to write a thorough but concise answer. Let me compile it from all sources.
Electroconvulsive Therapy (ECT)
Definition
ECT is a procedure in which brief electrical currents are applied across the scalp under general anesthesia and muscle relaxation to deliberately induce a bilateral generalized seizure of approximately 1 minute duration. It is one of the most effective treatments in psychiatry.
(Kaplan & Sadock's Synopsis of Psychiatry)
History
| Year | Milestone |
|---|---|
| 1500s | Paracelsus uses camphor (by mouth) to induce seizures for psychiatric illness |
| 1934 | Ladislas von Meduna uses camphor IM for catatonic schizophrenia |
| 1938 | Ugo Cerletti & Lucio Bini administer the first ECT to a delusional patient - full remission after 11 treatments |
| 1940 | First ECT use in the United States |
| 1980s-90s | Standardized guidelines published; refined electrode placement and waveforms to reduce memory side effects |
Indications
Primary (first-line or near first-line):
- Severe, treatment-resistant major depression (most common indication; ~100,000 patients/year in the USA)
- Catatonia
- Severe suicidality (where rapid response is needed)
- Mania unresponsive to medications
- Bipolar depression
- Life-threatening inanition (inability to eat due to psychiatric illness)
Also used for: treatment-resistant schizophrenia (especially with catatonic features), Parkinson's disease with psychiatric comorbidity, neuroleptic malignant syndrome.
Pre-ECT Evaluation
- CBC, serum electrolytes, urinalysis, LFTs
- ECG (cardiovascular assessment)
- Comprehensive medical history and physical examination
- Spinal X-ray not routinely required due to use of modern muscle relaxants
- Informed consent
(Kaplan & Sadock's Synopsis, p. 221)
Technique
- Anesthesia - patient receives general anesthesia (commonly methohexital or propofol) + muscle relaxant (succinylcholine) to prevent physical injury during seizure
- Oxygenation - ventilated by mask
- Electrode placement:
- Bilateral (bitemporal) - most effective, but more cognitive side effects
- Right unilateral - fewer cognitive effects, but dose must be adequately suprathreshold
- Bifrontal - intermediate option
- Stimulus - brief-pulse or ultrabrief-pulse square wave current; dose measured in millicoulombs (charge). Only ~20% of applied charge enters the skull because bone has high impedance.
- Seizure duration goal - approximately 25-60 seconds (both motor and EEG)
- Sessions - typically 3 times per week for 2-4 weeks (total: 6-12 treatments in an acute course)
Mechanism of Action
Not fully understood. Key findings:
- Bilateral generalized seizure is necessary - subconvulsive stimulation is ineffective
- Neurotransmitter effects: downregulation of post-synaptic β-adrenergic receptors (same as antidepressants); effects on serotonin, dopamine, muscarinic/cholinergic systems
- Anticonvulsant effect: raises seizure threshold progressively over the course
- Metabolic changes: during seizure - increased cerebral blood flow, glucose, O2 use, and blood-brain barrier permeability; after seizure - decreased metabolism in frontal lobes (degree correlates with therapeutic response)
- Neuroplasticity: ECT triggers neurogenesis and structural changes, particularly in the hippocampus
- EEG: postictal suppression (60-90 seconds), followed by delta/theta waves, returning to baseline ~30 min later
(Kaplan & Sadock's Synopsis, pp. 2232-2233)
Adverse Effects
| Side Effect | Details |
|---|---|
| Memory impairment | Most significant; both retrograde (months before treatment) and anterograde (new memory storage); usually transient, clears weeks to months post-ECT |
| Post-ictal confusion | Common, resolves within 1 hour |
| Headache | Common, usually mild |
| Muscle aches | Due to succinylcholine |
| Cardiovascular | Brief hypertension and tachycardia during seizure (mediated by autonomic surge) |
| Prolonged seizure | Rare; >3 min = status epilepticus, treated with IV benzodiazepines |
The bilateral electrode placement carries the highest risk of cognitive side effects; right unilateral and ultrabrief pulse width reduce this risk.
Efficacy
- Response rates of 60-80% in treatment-resistant depression
- Faster onset than antidepressants (days, not weeks) - key advantage for suicidal or severely ill patients
- ECT remains the most effective treatment for major depression
- Nobel laureate Paul Greengard proposed renaming it "electrocortical therapy" to reduce stigma around the word "convulsion"
Continuation After ECT
Relapse is common after an acute ECT course without maintenance therapy. Options:
- Continuation pharmacotherapy - combination of nortriptyline + lithium is superior to either alone (landmark 2001 trial)
- Maintenance ECT (monthly or more frequent sessions) for patients who relapse on medications
Sources: Kaplan & Sadock's Synopsis of Psychiatry, pp. 2225-2235; Neuroscience: Exploring the Brain, 5e, pp. 1983-1984; Family Medicine 9e, p. 221
Electron chain transport
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I have all the content I need. Here is the complete answer:
Electron Transport Chain (ETC)
Location
The ETC (except cytochrome c) is embedded in the inner mitochondrial membrane. It is the final common pathway by which electrons from fuel metabolism flow to oxygen, reducing it to water.
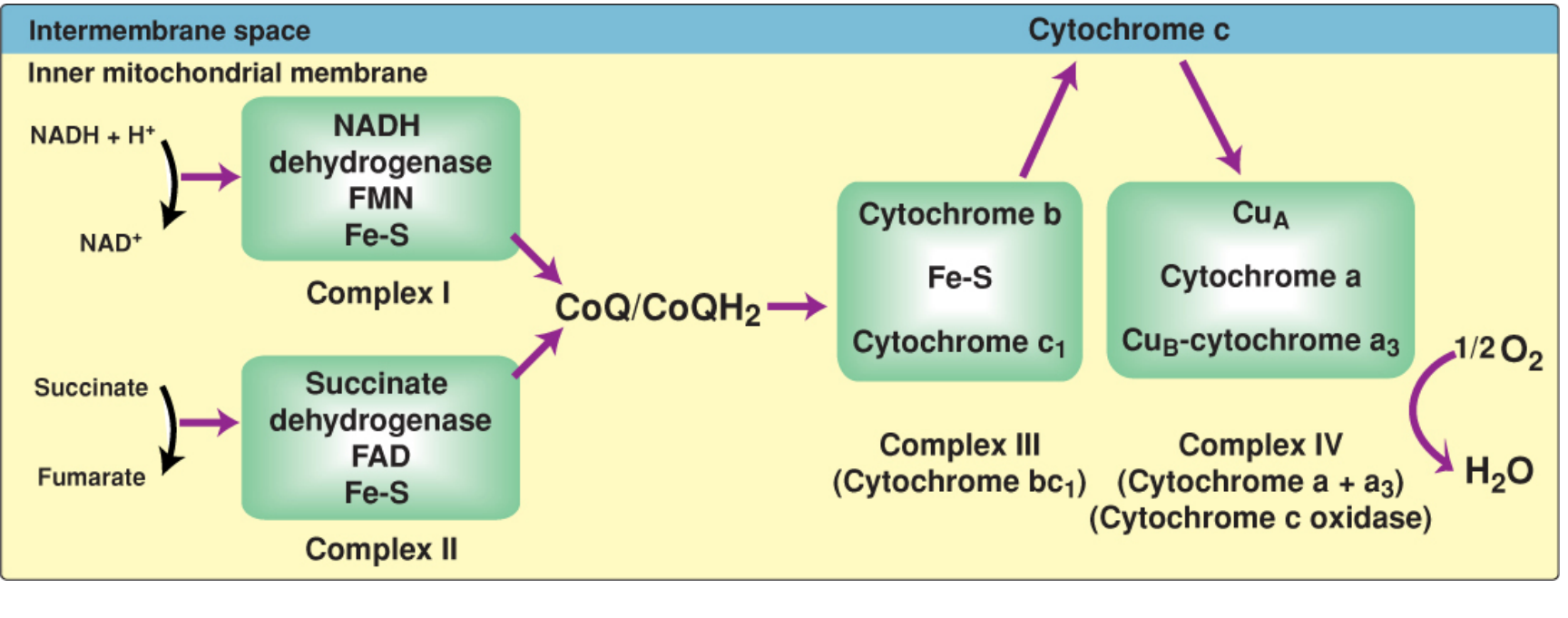
Electron transport chain showing electron flow (magenta arrows) from NADH/FADH2 through Complexes I-IV to O2. - Lippincott's Biochemistry, 8e, p. 228
Overview
Energy-rich fuels (glucose, fatty acids, amino acids) are catabolized to reduce the coenzymes NAD+ and FAD to NADH and FADH2. These then donate electrons to the ETC. As electrons flow "downhill" through successively more positive reduction potentials, the released energy is used to pump H+ across the inner mitochondrial membrane. The resulting proton gradient drives ATP synthesis by ATP synthase (Complex V). This coupling is called oxidative phosphorylation (OXPHOS).
The outer mitochondrial membrane is freely permeable (via porin channels). The inner membrane is impermeable to most ions including H+, which is essential for maintaining the proton gradient.
The Four Complexes
| Complex | Name | Substrates / Cofactors | Protons Pumped (matrix → IMS) | Inhibitors |
|---|---|---|---|---|
| I | NADH dehydrogenase (NADH:CoQ oxidoreductase) | NADH → FMN → Fe-S centers → CoQ | 4 H+ | Rotenone, amobarbital, metformin |
| II | Succinate dehydrogenase | FADH2 → Fe-S → CoQ | 0 (does not span membrane) | Malonate |
| III | Cytochrome bc1 (CoQ:cytochrome c oxidoreductase) | CoQH2 → cyt b → Fe-S → cyt c1 → cyt c | 4 H+ | Antimycin A |
| IV | Cytochrome c oxidase (cytochrome a + a3) | cyt c → CuA → cyt a → CuB-cyt a3 → O2 → H2O | 2 H+ | Cyanide (CN-), CO, H2S, sodium azide (NaN3) |
Key mobile carriers connecting the complexes:
- Coenzyme Q (CoQ / ubiquinone) - lipid-soluble, free to diffuse in membrane; links Complexes I and II to Complex III
- Cytochrome c - small protein in the intermembrane space; shuttles electrons from Complex III to Complex IV
Step-by-Step Electron Flow
NADH → Complex I → CoQ ↘
→ Complex III → Cytochrome c → Complex IV → ½O2 → H2O
FADH2 → Complex II → CoQ ↗
- NADH donates a hydride ion (H-) to Complex I; electrons pass through FMN and Fe-S centers to CoQ. NAD+ is regenerated.
- FADH2 (from succinate dehydrogenase, Complex II) donates electrons directly to CoQ. Since Complex I is bypassed, fewer H+ are pumped (lower ATP yield).
- CoQH2 carries electrons to Complex III, where they pass through cytochrome b, Fe-S center, and cytochrome c1, then to cytochrome c.
- Cytochrome c (in intermembrane space) ferries electrons to Complex IV.
- Complex IV transfers electrons to the final acceptor: O2, reducing it to H2O. The iron in cytochromes alternates between Fe3+ (ferric) and Fe2+ (ferrous) with each electron transfer.
Chemiosmosis and ATP Synthesis (Complex V)
Based on Mitchell's chemiosmotic hypothesis:
- Proton pumping at Complexes I, III, and IV creates an electrochemical proton gradient (high H+ in intermembrane space, low in matrix)
- H+ flow back into the matrix through ATP synthase (F0F1-ATPase, Complex V)
- This drives rotation of the F1 subunit, causing conformational changes in the three αβ subunit pairs (binding change mechanism), synthesizing ATP from ADP + Pi
- The energy-requiring step is actually ATP release from the synthase, not the phosphorylation itself
- ~3 H+ are needed per ATP synthesized
Coupling: Electron transport and ATP synthesis are tightly coupled - one cannot occur without the other. When ATP is not being used, proton back-pressure builds and slows electron transport.
ATP Yield
| Electron Donor | ATP Produced | Why |
|---|---|---|
| NADH | ~2.5 ATP | Enters at Complex I; all 3 pumping complexes used |
| FADH2 | ~1.5 ATP | Enters at Complex II; bypasses Complex I (fewer H+ pumped) |
- Energy released from NADH oxidation: ~53 kcal/mol
- Energy released from FADH2 oxidation: ~41 kcal/mol
- Only ~30% is captured as ATP; the rest is released as heat (this is the body's major source of heat)
Reactive Oxygen Species (ROS)
Electron leakage from the ETC (mainly at Complexes I and III) generates toxic ROS:
- Superoxide (O2-)
- Hydrogen peroxide (H2O2)
- Hydroxyl radicals (OH-)
Cellular defenses: Superoxide dismutase (SOD), catalase, glutathione peroxidase
Cytoplasmic NADH - Shuttle Systems
NADH produced in the cytosol (e.g., during glycolysis) cannot cross the inner mitochondrial membrane. Two shuttles transfer its electrons:
| Shuttle | Enters As | ATP Yield |
|---|---|---|
| Malate-aspartate shuttle (heart, liver) | NADH (mitochondrial) | ~2.5 ATP |
| Glycerol 3-phosphate shuttle (brain, muscle) | FADH2 (mitochondrial) | ~1.5 ATP |
Inhibitors Summary
| Inhibitor | Site | Mechanism |
|---|---|---|
| Rotenone, amobarbital, metformin | Complex I | Block NADH → CoQ transfer |
| Malonate | Complex II | Competitive inhibitor of succinate dehydrogenase |
| Antimycin A | Complex III | Blocks CoQH2 → cytochrome c |
| Cyanide (CN-), CO, H2S, NaN3 | Complex IV | Block O2 reduction (cytochrome a3) |
| Oligomycin | ATP synthase (Complex V) | Blocks H+ channel of F0 subunit |
| 2,4-DNP, aspirin (toxic doses) | Inner membrane | Uncouplers - dissipate H+ gradient; ETC runs but no ATP made (energy released as heat) |
Clinical Relevance
- Ischemia/MI: Lack of O2 halts Complex IV → no H+ pumping → no ATP → mitochondrial swelling → irreversible cell death (necrosis)
- Cyanide poisoning: Blocks Complex IV; cells cannot use O2; treated with hydroxocobalamin or nitrites (form methemoglobin which scavenges CN-)
- Doxorubicin cardiotoxicity: Binds cardiolipin in the inner membrane; inhibits succinate oxidation, inactivates cytochrome oxidase, inhibits ATP synthase → reduced ATP in cardiomyocytes
- Mitochondrial diseases (MELAS, Leigh, MERRF): Mutations in mitochondrial DNA encoding ETC subunits
Sources: Lippincott's Illustrated Reviews: Biochemistry, 8e, pp. 224-237; Basic Medical Biochemistry: A Clinical Approach, 6e, pp. 862-870
This is a shared conversation. Sign in to Orris to start your own chat.