As a Nurse How will evaluate on going CPR Victim in Your Hospital এই প্রশ্নের উত্তর টেক্সটবুক based কি হবে? যাতে প্রফেসর accept করে?
Reading File
Finding Sources
Finding Sources
Searching PubMed
CPR monitoring assessment quality resuscitation
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
I now have comprehensive, professor-grade textbook material. Let me compile the full answer.
Ongoing CPR Evaluation: Nurse's Role in the Hospital Setting
A Textbook-Based Answer for Academic Submission
1. Initial Recognition and Team Activation
The first step before CPR begins is recognizing the arrest. Per Tintinalli's Emergency Medicine (Table 22-1), the AHA Chain of Survival for in-hospital cardiac arrest (IHCA) begins with:
- Recognition - assess for unresponsiveness, absence of normal breathing, gasping
- Immediate activation of the emergency response system (Code Blue/Crash team call)
- Immediate high-quality CPR
- Rapid defibrillation
- Advanced life support and post-arrest care
"Management of cardiac arrest occurs in an orchestrated effort by a health care team led by a clinician who can monitor the efficacy and response to therapeutic interventions."
- Rosen's Emergency Medicine, p. 79
2. Evaluating the Quality of Ongoing Chest Compressions
This is the most critical ongoing assessment during CPR. According to multiple authoritative sources, the nurse must continuously monitor the following benchmarks:
High-Quality CPR Parameters (AHA/ACLS Standards)
| Parameter | Target Value |
|---|---|
| Compression rate | 100-120 compressions/min |
| Compression depth | 5-6 cm (2-2.5 inches) in adults |
| Chest recoil | Full recoil between each compression (no leaning) |
| Compression fraction | At least 80% (CPR performed 80 of every 100 seconds of pulseless interval) |
| Ventilation rate | 10 breaths/min (1 breath every 6 seconds after advanced airway) |
| Compression interruption | < 10 seconds |
"Important benchmarks of quality CPR include compression rate 100-120 compressions/min, compression depth 5-6 cm, compression fraction at least 80%, full chest recoil between compressions, and a ventilation rate of 10 breaths/min."
- Rosen's Emergency Medicine, p. 79
"Slow compression rates, inadequate depth of compression, and substantial pauses are the norm. An approach to push hard, push fast, minimize interruptions, allow full chest recoil, and don't overventilate can markedly improve myocardial, cerebral, and systemic perfusion."
- Miller's Anesthesia, 10th Edition, p. 11299
Nursing Actions for Quality Control:
- Switch compressors every 2 minutes (or when fatigued) to prevent degradation in quality
- Use CPR feedback devices (force sensors/accelerometers) when available - these provide real-time verbal feedback on rate and depth
- Call out deviations - if depth is inadequate, verbally cue: "Push harder"
3. ECG/Rhythm Monitoring and 2-Minute Cycle Checks
After every 2-minute CPR cycle, the nurse participates in or supports a rhythm check:
Systematic Approach (Tintinalli's Table 22-2):
- Step 3: Pulse check (healthcare provider only) - maximum 10 seconds - if no pulse, resume immediately
- Step 4: Continue 30:2 compression-to-ventilation ratio (until advanced airway placed)
- Step 5: Apply defibrillator as soon as available
- Step 6: Continue CPR between rhythm checks, restart compressions immediately after defibrillation
Per Rosen's Emergency Medicine:
- VF/pVT - defibrillate immediately, then resume CPR for 2 minutes before next rhythm check
- PEA/Asystole - focus on CPR quality + reversible causes (H's and T's)
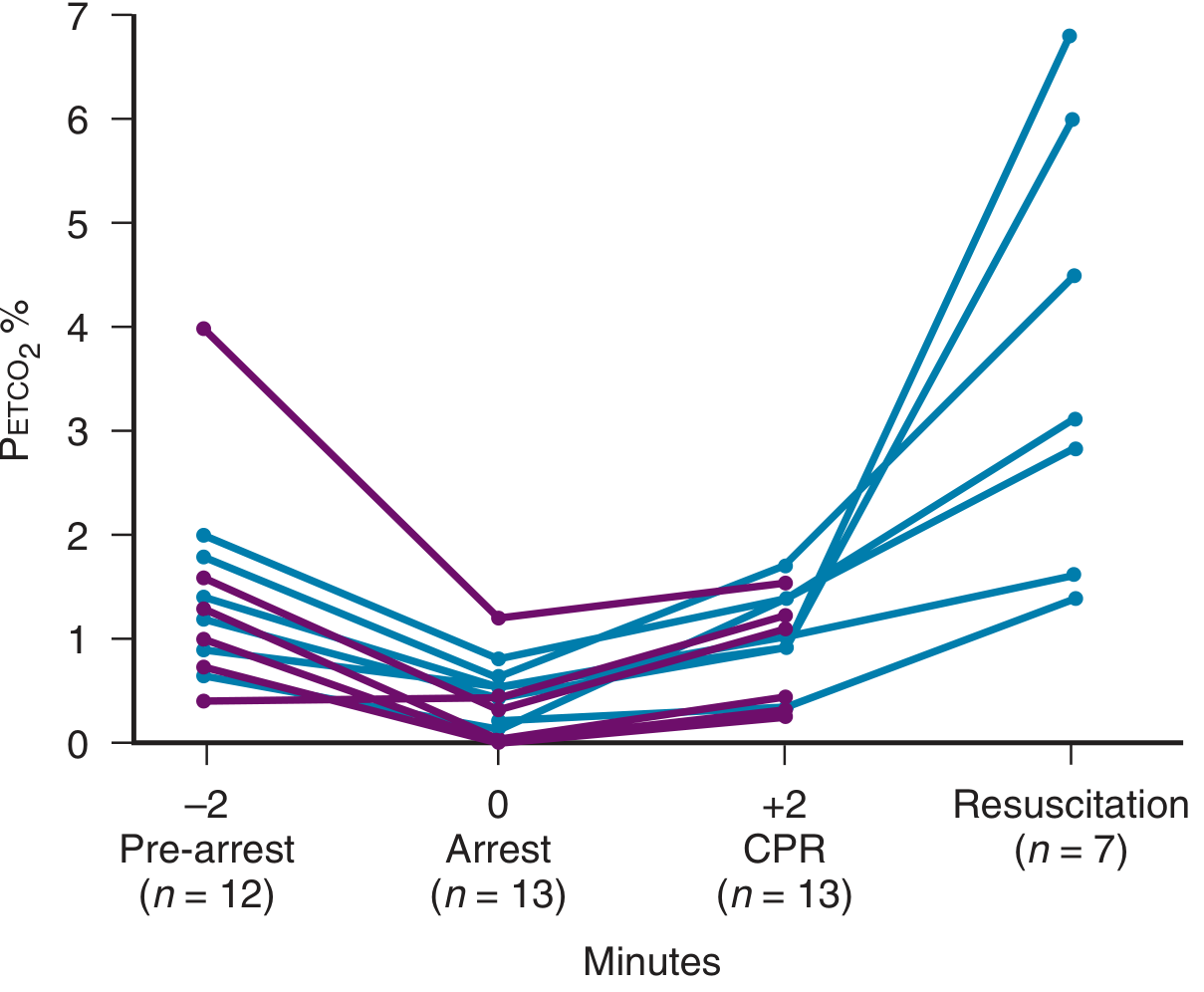
4. End-Tidal CO₂ (PETCO₂) Monitoring - Key Evaluation Tool
ETCO₂ is the most objective, non-invasive method of evaluating CPR effectiveness in a hospital setting.
What the Nurse Evaluates:
| PETCO₂ Finding | Clinical Interpretation |
|---|---|
| Low (< 10 mmHg) at 20 min after ACLS | Predicts death; consider terminating resuscitation |
| Gradually rising | Indicates improving CPR quality / cardiac output |
| Sudden sharp peak (spike) | Earliest sign of ROSC - may occur before palpable pulse |
| Normal capnogram waveform present | Confirms ET tube in trachea (not esophagus) |
"A peak in PETCO2 is the earliest sign of return of spontaneous circulation (ROSC) and may occur before palpable or measurable hemodynamic signs (pulse or blood pressure). When the heart is restarted, the dramatic increase in cardiac output...leads to a rapid increase in PETCO2."
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 72
"PETCO2 levels of 10 mm Hg or lower measured 20 minutes after the initiation of advanced cardiac life support accurately predicted death."
- Roberts and Hedges', p. 73
This is shown in the PETCO₂ pattern during CPR:
5. Monitoring for Return of Spontaneous Circulation (ROSC)
The nurse evaluates for ROSC without stopping compressions unnecessarily. Signs include:
| Sign | Assessment Method |
|---|---|
| Sudden PETCO₂ spike | Capnography (earliest sign) |
| Palpable pulse | Carotid/femoral pulse check (max 10 sec) |
| Blood pressure reading | Arterial line (if in place) or NIBP |
| Spontaneous movement or breathing | Visual observation |
| Organized rhythm on monitor | ECG/cardiac monitor |
| Pupillary response changes | Neurological assessment |
"Restoration of adequate cardiac function is the defining factor of ROSC. Restoration of good neurologic function is the defining metric of a successful resuscitation."
- Rosen's Emergency Medicine, p. 79
6. Evaluating Reversible Causes - The H's and T's
Throughout ongoing CPR, the nurse assists the team in identifying and treating reversible causes:
| H's | T's |
|---|---|
| Hypovolemia | Tension pneumothorax |
| Hypoxia | Tamponade (cardiac) |
| Hydrogen ion (acidosis) | Toxins/overdose |
| Hypo/Hyperkalemia | Thrombosis - pulmonary |
| Hypothermia | Thrombosis - coronary (MI) |
7. Airway and Ventilation Assessment
- Confirm ET tube placement via ETCO₂ waveform and bilateral breath sounds
- Once advanced airway secured: deliver 1 breath every 6 seconds (10/min) without pausing compressions
- Avoid hyperventilation - it reduces cardiac output during CPR
- O₂ saturation via pulse oximetry (note: unreliable during arrest due to low perfusion)
"Hyperventilation during CPR should be avoided, as it is associated with reduced cardiac output during CPR."
- Rosen's Emergency Medicine, p. 80
8. Medications During CPR - Nurse's Documentation and Evaluation
The nurse (often the medication nurse role in the crash team) evaluates medication response:
- Epinephrine 1 mg IV/IO every 3-5 minutes (vasopressor for all rhythms)
- Amiodarone 300 mg IV for refractory VF/pVT (then 150 mg if needed)
- Sodium bicarbonate for documented severe acidosis or hyperkalemia
The nurse records the time of each drug administration, documents rhythm before and after defibrillation, and tracks elapsed resuscitation time.
9. Factors Affecting CPR Outcome (for Evaluation Framing)
Per Miller's Anesthesia (10th ed.), key factors influencing resuscitation outcome include:
- Pre-existing condition of the patient
- Environment (in-hospital vs. out-of-hospital)
- Initial ECG rhythm detected
- Duration of no-flow time (time without CPR or spontaneous circulation)
- Quality of life-supporting therapies during resuscitation
- Quality of post-resuscitation care
10. Summary Evaluation Checklist (Professor-Acceptable Format)
A nurse evaluating ongoing CPR monitors:
- Responsiveness level - unresponsive, no breathing, no pulse confirmed
- Compression quality - rate 100-120/min, depth 5-6 cm, full recoil, fraction ≥80%
- Rhythm - every 2-minute check (VF/pVT = shock; PEA/asystole = continue CPR + treat cause)
- PETCO₂ - rising = good CPR; spike = ROSC; <10 mmHg at 20 min = poor prognosis
- Airway - tube confirmed, ventilation rate 10/min, no hyperventilation
- Medications - epinephrine timing, antiarrhythmics as indicated
- Signs of ROSC - ETCO₂ spike, palpable pulse, BP, spontaneous movement
- Reversible causes - H's and T's actively addressed
- Time tracking - elapsed CPR time, drug times, shock times documented
- Team fatigue - compressor switch every 2 minutes
References (Textbook Citations for Professor):
- Rosen's Emergency Medicine, 10th Ed. - Chapter 5: Cardiac Arrest
- Tintinalli's Emergency Medicine, 9th Ed. - Chapter 22: CPR (Tables 22-1, 22-2, 22-3)
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, 7th Ed. - ETCO₂ Monitoring
- Miller's Anesthesia, 10th Ed. - Chapters 31, 34: Cardiac Arrest and Resuscitation Quality
Function of growth hormone
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have excellent, comprehensive textbook content from multiple authoritative sources. Let me compile the full answer.
Functions of Growth Hormone (GH / Somatotropin)
1. What is Growth Hormone?
Growth hormone (GH), also called somatotropin, is a polypeptide hormone synthesized and secreted by the somatotroph cells of the anterior pituitary gland. It is the most abundant anterior pituitary hormone.
"Growth hormone has multiple metabolic actions on liver, muscle, adipose tissue, and bone, as well as growth-promoting actions in virtually every other organ."
- Costanzo Physiology, 7th Ed., p. 416
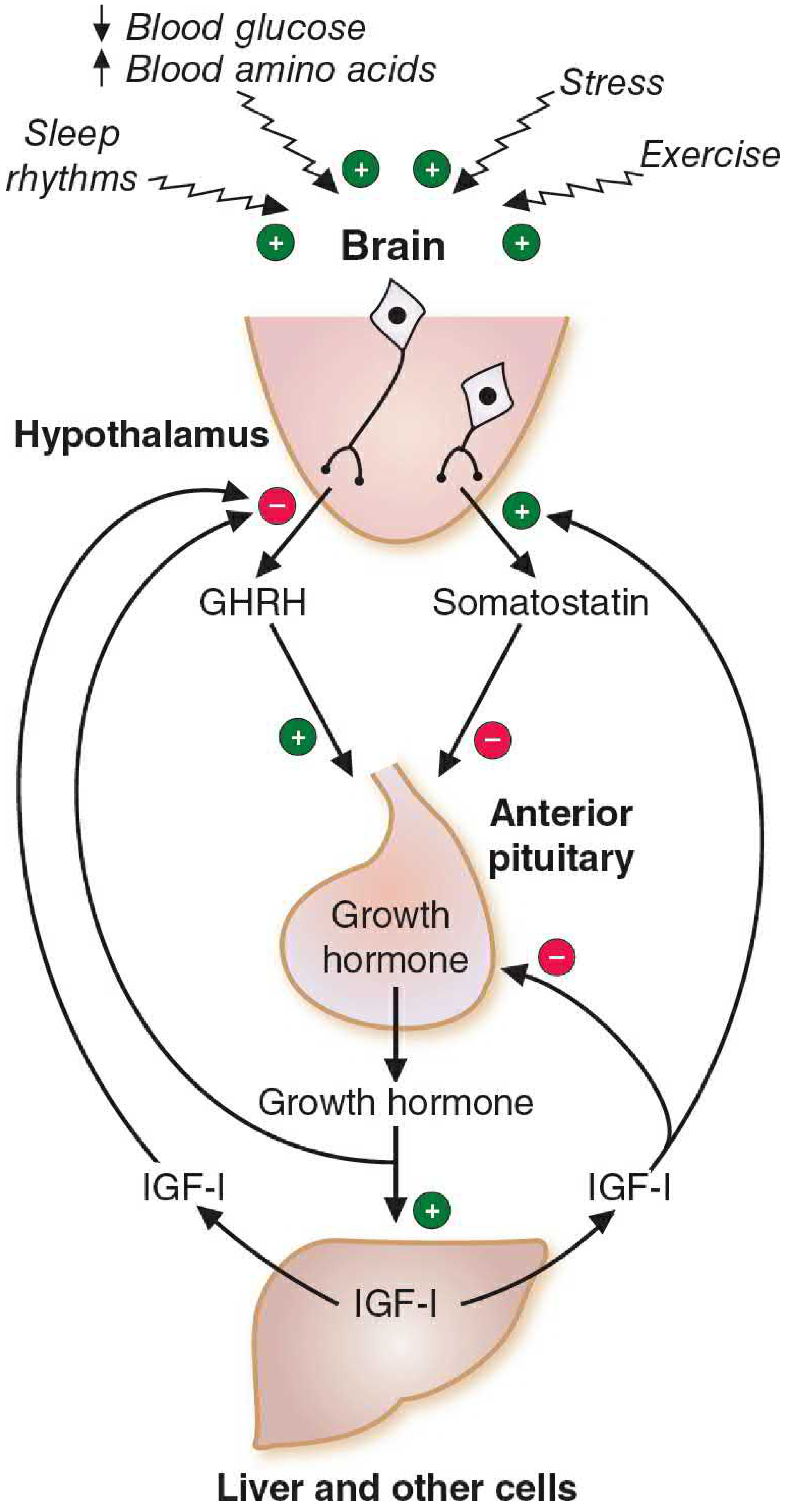
2. Regulation of GH Secretion
Hypothalamic Control (Two-Pathway System):
| Factor | Effect on GH |
|---|---|
| GHRH (Growth Hormone-Releasing Hormone) | Stimulates GH synthesis and secretion via cAMP + IP₃/Ca²⁺ second messengers |
| Somatostatin (SRIF) | Inhibits GH secretion by blocking GHRH action via Gi protein → ↓cAMP |
Stimulatory vs. Inhibitory Factors (Costanzo Physiology, Table 9.4):
| Stimulatory Factors | Inhibitory Factors |
|---|---|
| Hypoglycemia (↓ blood glucose) | Hyperglycemia (↑ blood glucose) |
| Fasting / starvation | ↑ Free fatty acids |
| Exercise | Obesity |
| Stress (trauma, fever, anesthesia) | Somatostatin |
| Puberty hormones (estrogen, testosterone) | IGF-1 / Somatomedins (negative feedback) |
| Stage III & IV sleep | Senescence |
| α-Adrenergic agonists | β-Adrenergic agonists |
| Arginine | Pregnancy |
Secretion Pattern:
- Released in a pulsatile manner (~every 2 hours)
- Largest burst: within 1 hour of falling asleep (stage III/IV NREM sleep)
- Peaks during puberty (driven by estrogen in females, testosterone in males)
- Declines with aging (senescence)
Negative Feedback Loops (3 loops):
- GHRH inhibits its own secretion (ultrashort-loop)
- IGF-1 (somatomedin C) inhibits GH from anterior pituitary
- GH + IGF-1 stimulate somatostatin from hypothalamus → inhibits GH
3. Mechanism of Action
GH acts through two pathways:
Direct Action (via GH Receptors):
- GH receptors are on skeletal muscle, liver, adipose tissue, and many other cells
- Receptor is a tyrosine kinase-associated receptor (Janus kinase / JAK-STAT pathway)
- Activates STAT transcription factors, MAP kinase pathway, and AKT pathway depending on tissue
Indirect Action (via IGF-1 / Somatomedins):
- GH stimulates the liver (primarily) to produce IGF-1 (Somatomedin C)
- IGF-1 acts on target tissues via receptors with intrinsic tyrosine kinase activity (similar to insulin receptor)
- Most growth-promoting effects of GH are mediated through IGF-1
"The growth-promoting effects of growth hormone are mediated largely through production of somatomedins."
- Costanzo Physiology, 7th Ed., p. 416
"GH...induces release of IGF-1 from the liver, which is responsible for subsequent GH-like actions. The half-life of GH is short (~25 minutes)."
- Lippincott Illustrated Reviews: Pharmacology, p. 770
4. Functions of Growth Hormone
A. Linear Bone Growth (Most Striking Effect)
- Mediated via IGF-1/somatomedins
- Stimulates DNA, RNA, and protein synthesis in cartilage cells (chondrocytes)
- Widens epiphyseal plates of long bones
- Increases proliferation of chondrocytes
- Increases periosteal bone growth
- Only effective while epiphyseal plates are open (before puberty closes the growth plates)
B. Protein Synthesis and Organ Growth (Anabolic Effects)
- Increases amino acid uptake into virtually all cells
- Stimulates synthesis of DNA, RNA, and protein
- Increases lean body mass and organ size
- Causes positive nitrogen balance (diverts amino acids from oxidation to protein synthesis)
- In muscle: increased amino acid transport + increased nitrogen retention + increased fat-free tissue
"These actions are accompanied by a direct anabolic influence of GH on protein metabolism with a diversion of amino acids from oxidation to protein synthesis and a shift to a positive nitrogen balance."
- Basic Medical Biochemistry, 6th Ed., p. 1481
C. Diabetogenic / Anti-Insulin Effect on Carbohydrate Metabolism
- GH causes insulin resistance in peripheral tissues (muscle, adipose)
- Decreases glucose uptake and utilization by muscle and fat
- Raises blood glucose concentration (similar effect to lack of insulin)
- Consequently increases blood insulin levels as a compensatory response
- Called "diabetogenic" because it mimics a diabetic state
D. Fat Metabolism (Lipolysis)
- Increases lipolysis in adipose tissue
- Inhibits lipoprotein lipase (reduces fat storage)
- Stimulates hormone-sensitive lipase (promotes fat breakdown)
- Decreases lipogenesis (less fat synthesis)
- Decreases glucose transport into fat cells
- Net effect: mobilizes free fatty acids into the blood for energy use
- Leads to decreased body fat and redistribution of body composition
E. Other Metabolic and Organ Effects
| Target Tissue | GH Effect |
|---|---|
| Liver | IGF-1 production, gluconeogenesis |
| Kidney | Increased GFR, phosphate reabsorption, IGF-1 production |
| Immune system | Stimulates thymic growth and lymphocyte function |
| Heart | Increases cardiac output and myocardial contractility |
| Skin | Increases skin thickness and collagen synthesis |
| Bone density | Increases bone mineral density in adults |
5. Summary of GH Functions (Quick Reference)
| Function | Mechanism |
|---|---|
| Linear growth | IGF-1 → chondrocyte proliferation, epiphyseal plate widening |
| Protein synthesis | Direct + via IGF-1 → ↑ amino acid uptake, ↑ RNA/DNA/protein |
| Anti-insulin / diabetogenic | Direct → insulin resistance, ↑ blood glucose |
| Lipolysis | Direct → ↑ HSL, ↓ LPL, ↑ FFA release from adipose |
| Organ growth | Via IGF-1 → cell multiplication + differentiation |
| Bone density (adults) | Direct periosteal growth (after growth plates close) |
6. Pathophysiology (Clinically Important)
| Condition | Cause | Features |
|---|---|---|
| Pituitary Dwarfism | GH deficiency in children | Short stature, ↑ fat, delayed puberty |
| Laron Dwarfism | GH receptor defect | High GH levels, no IGF-1 response, treatment-resistant |
| Gigantism | GH excess BEFORE puberty (epiphyses open) | Excessive linear growth |
| Acromegaly | GH excess AFTER puberty (epiphyses closed) | Enlarged hands/feet, coarse facial features, insulin resistance |
"Before puberty, excessive levels of growth hormone cause gigantism...After puberty...excess levels cause increased periosteal bone growth, increased organ size...insulin resistance, and glucose intolerance."
- Costanzo Physiology, 7th Ed., p. 417
Textbook References:
- Costanzo Physiology, 7th Ed. - Chapter 9 (Endocrine Physiology), pp. 415-417
- Basic Medical Biochemistry: A Clinical Approach, 6th Ed. - Chapter 41, pp. 1481-1482
- Lippincott Illustrated Reviews: Pharmacology - Chapter 23, pp. 769-770
- Tietz Textbook of Laboratory Medicine, 7th Ed. - Endocrine section
This is a shared conversation. Sign in to Orris to start your own chat.