Describe clinical features morphology diagnostic approach of lung tumours
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from authoritative textbooks. Let me compile the complete, well-structured response on lung tumours.
Lung Tumours: Clinical Features, Morphology, and Diagnostic Approach
Overview and Classification
Lung cancer is one of the leading causes of cancer death worldwide. The 2021 WHO classification recognises four major histologic subtypes with distinct biology, morphology, and clinical behaviour:
| Category | Main Types | Frequency |
|---|---|---|
| Non-small cell lung carcinoma (NSCLC) | Adenocarcinoma, Squamous cell carcinoma, Large cell carcinoma | ~84% |
| Small cell lung carcinoma (SCLC) | - | ~13% |
| Neuroendocrine (carcinoid) | Typical & Atypical | 1-2% |
| Other | Mesothelioma, sarcomatoid carcinoma | Rare |
Key risk factors: Cigarette smoking dominates across all subtypes. Others include asbestos, radon, occupational carcinogens, EGFR/ALK driver mutations (especially in non-smokers).
1. Adenocarcinoma
Clinical Features
- Most common subtype overall; more prevalent in women and non-smokers
- Typically peripheral in location
- Often presents as a solitary pulmonary nodule or ground-glass opacity on CT
- May be asymptomatic until late (peripheral lesions avoid early bronchial obstruction)
- Paraneoplastic: migratory thrombophlebitis (Trousseau syndrome), non-bacterial endocarditis, DIC, hypercoagulability
Morphology
- Gross: Peripheral grey-white mass, often with central scarring + pleural puckering (arrow sign on CT/gross specimen); anthracotic pigment incorporation
- Microscopic: Gland-forming architecture (acinar, papillary, lepidic, micropapillary patterns); mucin production present; abundant cytoplasm, pleomorphic nuclei with coarse chromatin and prominent nucleoli
- Precursor lesions: Atypical adenomatous hyperplasia (AAH) → Adenocarcinoma in situ (AIS) → Minimally invasive → Invasive adenocarcinoma
- IHC: TTF-1 positive (nuclear staining - see inset in image below), CK7+, mucin+, napsin-A+
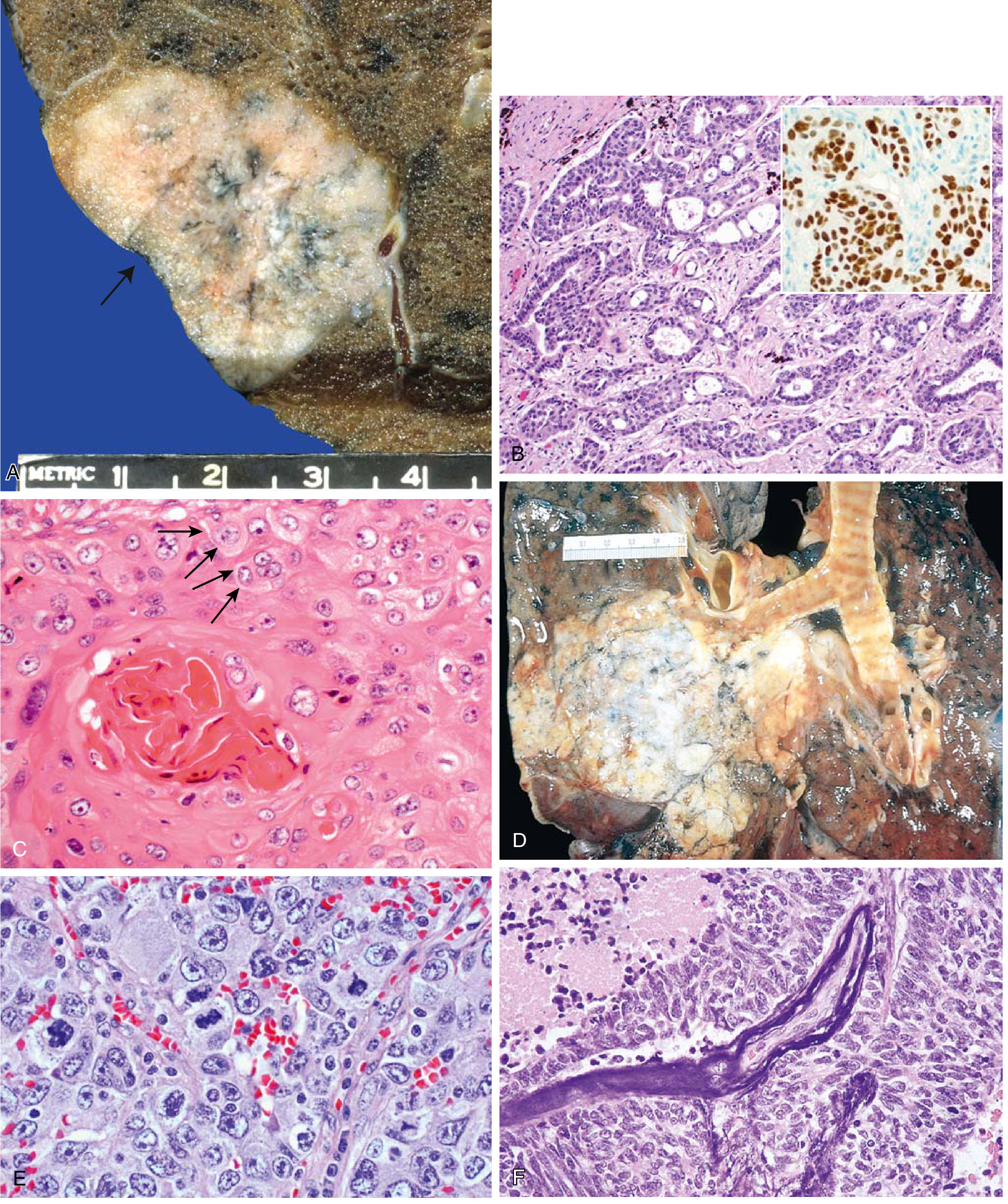
Fig. 11.44: Lung carcinoma pathology. (A) Peripheral adenocarcinoma with central scarring and pleural puckering. (B) Gland-forming adenocarcinoma with TTF-1 IHC (inset). (C) Well-differentiated squamous cell carcinoma with keratinisation, keratin pearls, and intercellular bridges. (D) Squamous cell carcinoma as a central hilar mass invading parenchyma. (E) Large cell carcinoma - sheets of large cells without differentiation. (F) Small cell carcinoma with deeply basophilic cells, necrosis, and Azzopardi effect on vessel walls. - Robbins & Kumar Basic Pathology
Key Molecular Targets
- EGFR mutations (~20% of adenocarcinomas; enriched in non-smokers, women, East Asians) - targetable with erlotinib/osimertinib
- ALK fusions (4-6%; non-smokers, often signet-ring morphology) - targetable with crizotinib/alectinib
- KRAS mutations (~30%; associated with smoking)
- BRAF, ROS1, MET - additional actionable targets
2. Squamous Cell Carcinoma
Clinical Features
- Strongly associated with heavy smoking
- Typically central/hilar in location - arises from main/lobar bronchi
- Presents with: cough, haemoptysis, post-obstructive pneumonia, atelectasis
- Cavitation is common (central necrosis)
- Paraneoplastic: Hypercalcaemia (via PTHrP secretion) - most characteristic
- Pancoast tumour (superior sulcus): shoulder/arm pain, Horner syndrome
Morphology
- Gross: Central grey-white hilar mass invading bronchial wall and adjacent parenchyma; may cavitate
- Microscopic: Squamous differentiation - keratin pearls, individual cell keratinisation, intercellular bridges (desmosomes); pleomorphic nuclei
- Precursor lesions: Squamous metaplasia → Dysplasia → Squamous cell carcinoma in situ → Invasive
- IHC: p40/p63 positive, CK5/6+, TTF-1 negative, mucin negative
3. Small Cell Lung Carcinoma (SCLC)
Clinical Features
- Almost always in heavy smokers (diagnosis should be reconsidered in non-smokers)
- Central origin, rapid growth, invariably metastatic at diagnosis
- Mediastinal extension causes: SVC syndrome, recurrent laryngeal nerve palsy, dysphagia
- Pulmonary symptoms: cough, wheeze, dyspnoea, haemoptysis
- Widespread metastases: liver, brain, bone, adrenal glands
- Paraneoplastic syndromes are common and distinctive:
- SIADH (ectopic ADH)
- Eaton-Lambert syndrome (anti-VGCC antibodies - proximal weakness, improves with repeated use)
- Ectopic ACTH/Cushing syndrome (ectopic ACTH)
- Gastrin-releasing peptide, calcitonin production
Morphology
- Gross: Large central mass, often with necrosis; white-grey, soft consistency
- Microscopic (2021 WHO definition):
- Small cells with scant cytoplasm
- Finely granular "salt and pepper" nuclear chromatin - hyperchromatic
- Absent or inconspicuous nucleoli
- Cell size typically < 3 resting lymphocytes diameter (though variable)
- Nuclear moulding prominent
- Azzopardi effect: basophilic DNA encrustation of vessel walls from necrotic tumour cells
- High mitotic rate: >60 mitoses per 2 mm²
- Extensive necrosis and apoptosis
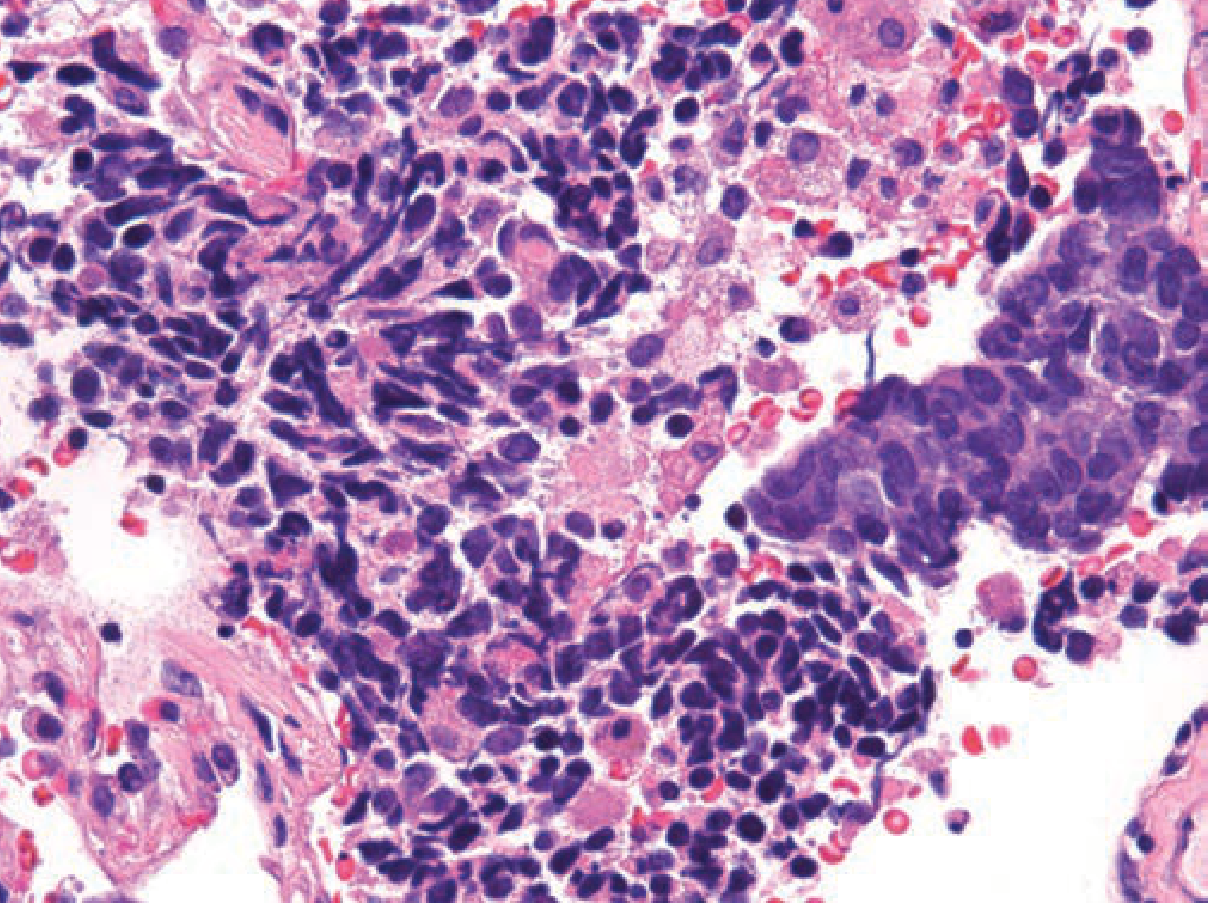
Fig. 111-18: Small cell carcinoma. Classic appearance: scant cytoplasm, hyperchromatic nuclei, nuclear moulding, crush artifact, necrosis. (H&E, 400x). - Fishman's Pulmonary Diseases
- IHC: Neuroendocrine markers - CD56, synaptophysin, chromogranin positive; dense-core granules on electron microscopy; TTF-1 often positive; EMA/CK positive; mucin absent
Staging
Traditionally: Limited (confined to ipsilateral hemithorax - radiotherapy port feasible) vs Extensive disease. IASLC now recommends TNM staging. ~60-70% present with extensive disease.
4. Large Cell Carcinoma
Clinical Features
- Diagnosis of exclusion - no glandular, squamous, or neuroendocrine differentiation by light microscopy
- Typically peripheral; presents late
- Poor prognosis
Morphology
- Microscopic: Sheets of large pleomorphic cells; abundant cytoplasm; vesicular nuclei with prominent nucleoli; no keratin pearls, gland formation, or neuroendocrine architecture by H&E
- Large cell neuroendocrine carcinoma (LCNEC): defined as high-grade NSCLC with neuroendocrine morphology (organoid nesting, trabecular, rosette-like, palisading patterns) + positive neuroendocrine IHC (CD56, chromogranin, synaptophysin); >10 mitoses/2 mm²; cells are relatively large with moderate-to-abundant cytoplasm; nucleoli prominent (key distinction from SCLC)
5. Carcinoid Tumours (Neuroendocrine)
Clinical Features
- Occur in younger adults (mean ~40 years); represent ~5% of pulmonary neoplasms
- May be part of MEN syndrome
- Typical carcinoid: low-grade; 5-15% metastasize to hilar nodes; distant metastases rare; often curable by resection
- Atypical carcinoid: higher mitotic rate, higher lymph node and distant metastasis risk; TP53 mutations in 20-40%
- Carcinoid syndrome (flushing, diarrhoea) if metastatic
Morphology
- Arise in main bronchi; two patterns:
- Polypoid spherical intraluminal mass
- Mucosal plaque penetrating bronchial wall (collar-button lesion)
- Microscopic: Nests of uniform cells; regular round nuclei; "salt-and-pepper" chromatin; absent or rare mitoses; little pleomorphism
- Spectrum: Typical carcinoid → Atypical carcinoid → LCNEC → SCLC (increasing aggressiveness)
Comparison: SCLC vs NSCLC
| Feature | Small Cell | Non-Small Cell |
|---|---|---|
| Microscopic | Scant cytoplasm; small hyperchromatic nuclei; fine chromatin; diffuse sheets | Abundant cytoplasm; pleomorphic nuclei; coarse chromatin; prominent nucleoli; glandular or squamous architecture |
| Neuroendocrine markers (CD56, chromogranin, synaptophysin) | Present | Absent |
| Mucin | Absent | Present (adenocarcinoma) |
| Peptide hormone | ACTH, ADH, GRP, calcitonin | PTHrP (squamous cell) |
| RB mutations | ~90% | ~20% |
| TP53 mutations | ~90% | ~50% |
| KRAS mutations | Rare | ~30% (adenocarcinoma) |
| EGFR mutations | Absent | ~20% (adenocarcinoma) |
| ALK fusions | Absent | 4-6% (adenocarcinoma) |
| Chemotherapy response | Often complete but invariably recurs | Incomplete |
| Checkpoint inhibitor response | Less responsive | Responsive |
(Robbins & Kumar Basic Pathology, Table 11.6)
Paraneoplastic Syndromes Summary
| Syndrome | Most common tumour type |
|---|---|
| Hypercalcaemia (PTHrP) | Squamous cell carcinoma |
| SIADH | Small cell carcinoma |
| Cushing syndrome (ectopic ACTH) | Small cell carcinoma |
| Eaton-Lambert syndrome | Small cell carcinoma |
| Hypertrophic pulmonary osteoarthropathy | Adenocarcinoma/large cell |
| Non-bacterial thrombotic endocarditis, DIC | Adenocarcinoma |
Diagnostic Approach
1. Imaging
- CT chest (with contrast): First-line; characterise mass (size, location, density, cavitation, lymphadenopathy); guide biopsy
- PET-CT (FDG): Avid uptake in most lung cancers due to high metabolic rate; essential for staging NSCLC; identifies unsuspected metastases; guides biopsy to most metabolically active area; changes management in significant proportion of patients
- SCLC: PET-CT changes staging (LD vs. ED) in ~15% of cases
- Brain MRI: Staging for SCLC and high-stage NSCLC
- Bone scan / MRI spine: Bone metastases
2. Tissue Diagnosis
- Bronchoscopy + BAL, brushings, endobronchial biopsy: Central tumours (squamous cell, SCLC)
- CT-guided percutaneous needle biopsy: Peripheral lesions; FDG-PET guidance targets most active area
- EBUS (Endobronchial ultrasound-guided TBNA): Mediastinal/hilar lymph nodes - staging
- Sputum cytology: Sensitivity limited; useful if central tumour with endobronchial involvement
- Thoracentesis: Malignant pleural effusion (cytology of fluid)
- Liquid biopsy (plasma ctDNA): EGFR mutation detection when tissue inadequate
3. Pathological/Histological Workup
- H&E morphology: Initial classification (SCLC vs NSCLC; glandular vs squamous vs undifferentiated)
- Immunohistochemistry panel:
- Adenocarcinoma: TTF-1+, napsin-A+, CK7+
- Squamous: p40/p63+, CK5/6+, TTF-1-
- SCLC/Neuroendocrine: CD56+, synaptophysin+, chromogranin+; high Ki-67
- LCNEC: neuroendocrine morphology + IHC markers
4. Molecular/Biomarker Testing (NSCLC - mandatory before treatment)
- EGFR mutation (exons 18-21, esp. exon 19 del and exon 21 L858R)
- ALK rearrangement (FISH, IHC, NGS)
- ROS1 rearrangement
- KRAS G12C mutation (targetable with sotorasib)
- BRAF V600E
- MET exon 14 skipping / amplification
- NTRK fusions
- PD-L1 expression (IHC): Predicts response to checkpoint inhibitors (pembrolizumab, atezolizumab); even PD-L1-negative tumours may respond via tumour microenvironment macrophages
- Tumour mutation burden (TMB): High TMB correlates with immunotherapy response
5. Laboratory Tests
- FBC, LFTs, renal function, LDH (staging/baseline)
- Serum calcium (PTHrP-mediated hypercalcaemia in squamous)
- Serum sodium (SIADH in SCLC)
- α1-antitrypsin (if concurrent emphysema)
Staging
- NSCLC: TNM staging (IASLC 8th edition) - Stage I-IV; drives surgical vs. chemo-radiation vs. systemic therapy decisions
- SCLC: Traditionally Limited disease (LD) vs Extensive disease (ED); IASLC now recommends TNM staging as well
Key Points to Remember (Robbins & Kumar Basic Pathology / Fishman's Pulmonary Diseases / Murray & Nadel's Respiratory Medicine):
- Adenocarcinoma is the most common lung cancer overall, especially in non-smokers and women
- Squamous cell carcinoma is central, cavitates, causes hypercalcaemia
- SCLC is central, always treated with chemotherapy (not surgery), has paraneoplastic syndromes, and invariably recurs despite initial response
- All NSCLC patients require molecular profiling before starting systemic treatment
- PET-CT is essential for staging and identifies occult metastases that change management
- SCLC has the highest mutation burden of any lung cancer but is paradoxically less responsive to checkpoint inhibitors than NSCLC
This is a shared conversation. Sign in to Orris to start your own chat.