explain pharangitis
Reading File
Finding Sources
Searching PubMed
pharyngitis diagnosis treatment
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from authoritative sources. Let me compile the full explanation.
Pharyngitis
Pharyngitis is inflammation of the pharynx (the back of the throat), most commonly presenting as a sore throat. It is one of the most frequent reasons for medical visits - accounting for over 7 million pediatric primary care visits annually in the US alone.
Clinical Appearance
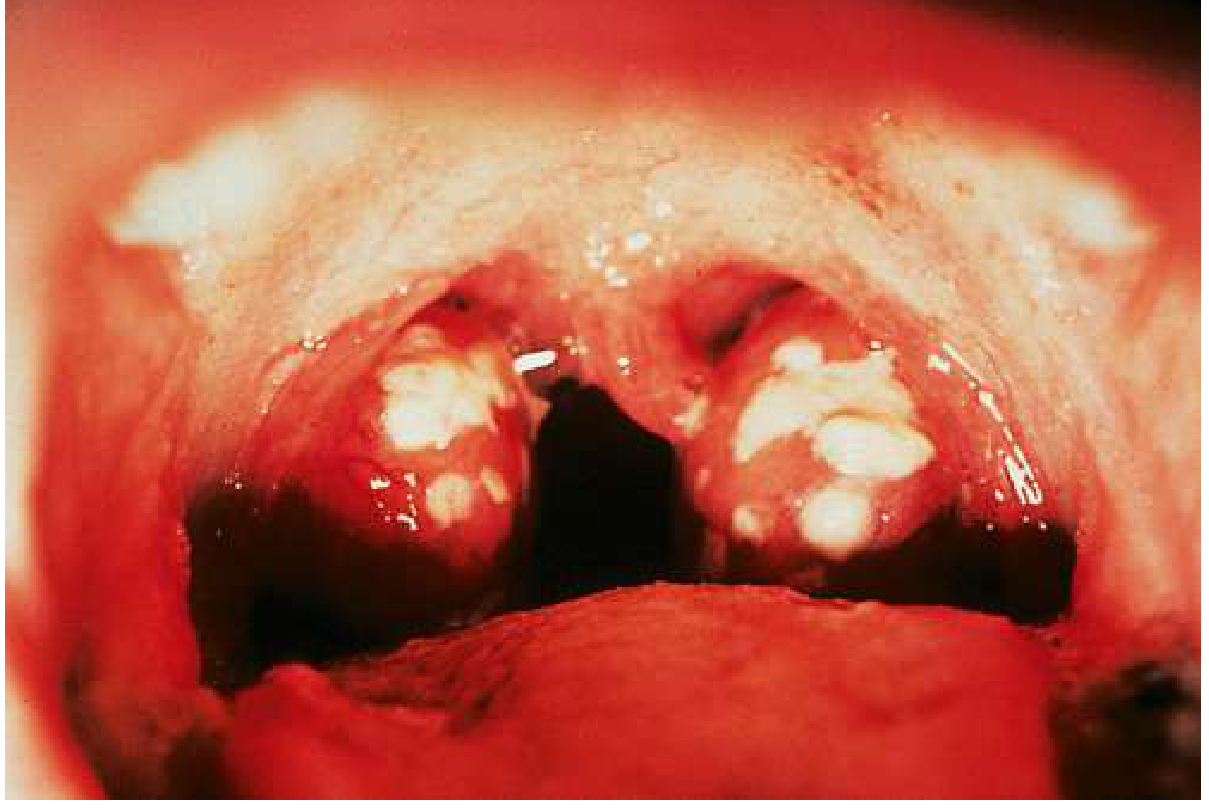
Typical appearance of bacterial (streptococcal) pharyngitis: erythematous, swollen tonsils with confluent white exudates.
Etiology (Causes)
Viral (50-80% of cases)
Viral causes dominate, especially in children. Common culprits include:
| Virus | Notes |
|---|---|
| Adenovirus | Very common |
| Epstein-Barr virus (EBV) | Causes infectious mononucleosis |
| Rhinovirus | Most frequent URI agent |
| Influenza A & B | Seasonal |
| Enterovirus (Coxsackievirus) | Hand-foot-mouth disease |
| Coronavirus, RSV, Parainfluenza | Various respiratory illnesses |
| Herpes simplex virus 1 & 2 | Can cause ulcerative pharyngitis |
| HIV | Acute retroviral syndrome |
| Cytomegalovirus | Mimics EBV mono |
Bacterial (20-40% in children, 5-15% in adults)
- Group A beta-hemolytic Streptococcus (GABHS) / Streptococcus pyogenes - the most important and most common bacterial cause
- Neisseria gonorrhoeae (in sexually active individuals)
- Corynebacterium diphtheriae (rare, but serious - diphtheria)
- Mycoplasma pneumoniae, Chlamydophila pneumoniae
- Fusobacterium necrophorum (can cause Lemierre's syndrome)
Symptoms
- Sore throat (dominant complaint)
- Odynophagia (pain on swallowing)
- Fever
- Headache
- Nausea, vomiting, abdominal pain (more common in children)
- Cough, hoarseness, coryza (suggest viral etiology)
- Myalgias, arthralgias, lethargy
- Chilliness (frank rigors are unusual in strep)
Physical Examination Findings
- Tonsillopharyngeal erythema and/or exudates
- Soft palate petechiae
- Uvular edema
- Hypertrophied tonsils
- Anterior cervical lymphadenopathy (submandibular)
- Rash (in scarlet fever)
- Conjunctivitis (suggests viral/adenovirus)
- Discrete oral ulcers/vesicles (suggest viral)
Key point: Tonsillar exudate does NOT reliably distinguish bacterial from viral etiology. Cough, rhinorrhea, oral ulcers, and conjunctivitis point strongly toward a viral cause.
Streptococcal Pharyngitis - the Clinically Most Important Type
S. pyogenes pharyngitis peaks in children aged 5-15 years, typically in winter and early spring. Classic presentation: abrupt onset of fever, sore throat, and submandibular adenopathy WITHOUT cough.
The infection triggers antibodies against M protein, streptolysin O, DNase, hyaluronidase, and pyrogenic exotoxins.
Even without treatment, symptoms typically resolve in 3-6 days - but untreated strep carries risks of serious complications.
The Centor/McIsaac Score (Modified Centor Score)
Used to predict likelihood of GABHS and guide testing/treatment:
| Criterion | Points |
|---|---|
| Tonsillar exudates | +1 |
| Tender anterior cervical lymphadenopathy | +1 |
| Absence of cough | +1 |
| Fever (>38°C) | +1 |
| Age 3-14 years | +1 |
| Age 15-44 years | 0 |
| Age ≥45 years | -1 |
- Score 0-1: GABHS unlikely - no testing or antibiotics needed
- Score 2-3: Test with rapid antigen or culture
- Score 4-5: High likelihood; consider empiric treatment
Diagnosis
Gold Standard
Throat culture - sensitivity 90-95%, but requires 18-48 hours for results.
Rapid Tests
- Rapid antigen detection test (RADT): sensitivity 80-90%, results in minutes
- Rapid nucleic acid test: sensitivity 97.5%, specificity 95% - preferred over antigen tests
- If RADT is negative in children/adolescents, a follow-up culture is recommended
- In adults, backup culture is usually not needed given the low incidence of GABHS and low rheumatic fever risk
Infectious Mononucleosis (EBV)
- Monospot (heterophile antibody) test - relatively insensitive in young children (only 25% positive in 10-24 months age)
- EBV IgM/IgG is more sensitive and specific but slower
- Atypical lymphocytes on CBC
- A telltale sign: amoxicillin or ampicillin given for presumed bacterial pharyngitis triggers a characteristic pruritic maculopapular rash
Complications of Untreated Streptococcal Pharyngitis
These are the main reason to diagnose and treat GABHS:
- Suppurative complications: peritonsillar abscess, retropharyngeal abscess, mastoiditis, otitis media, sinusitis
- Scarlet fever: strep infection + fever + characteristic sandpaper rash from pyrogenic exotoxins
- Acute rheumatic fever (ARF): autoimmune sequel affecting heart, joints, CNS; prevented by antibiotics
- Post-streptococcal glomerulonephritis (PSGN): immune complex nephritis; antibiotics do NOT prevent this
- Bacteremia
- Streptococcal toxic shock syndrome (uncommon)
Treatment
Viral Pharyngitis
- Supportive care only: analgesics (acetaminophen, NSAIDs), hydration, throat lozenges, warm saltwater gargles
- 85% resolve spontaneously within 1 week
- No antibiotics indicated
- For EBV/mono with severe tonsillar enlargement: a short course of corticosteroids may be considered to reduce swelling (though evidence is limited)
- EBV patients with splenomegaly: avoid contact sports until cleared by a physician
Bacterial (GABHS) Pharyngitis
Antibiotic of choice:
- Penicillin V (oral) or Amoxicillin - 10 days - first line
- Benzathine penicillin G - single IM injection - for compliance concerns
- Penicillin allergy: Azithromycin or clindamycin
Key points:
- Antibiotics shorten illness duration by ~1 day and prevent rheumatic fever
- Antibiotics do NOT prevent PSGN regardless of timing
- Delaying treatment by a few days is acceptable - still achieves the goal of preventing rheumatic fever while reducing unnecessary antibiotic use
- Patient satisfaction is most influenced by physician concern and reassurance - not antibiotic prescription
Special Considerations
Immunocompromised Patients
Consider opportunistic organisms: Candida albicans (thrush/pharyngitis), Mycobacterium avium.
Adolescents with Pharyngitis + High-Risk Behaviors
Acute HIV (acute retroviral syndrome) can mimic EBV pharyngitis in 50-70% of patients. Distinguishing features: no prominent exudates or tonsillar hypertrophy, mucocutaneous ulceration, rash.
Children Under 3 Years
Routine streptococcal testing is not recommended - low rates of strep and very low complication risk in this age group.
Summary Table
| Feature | Viral | Streptococcal (GABHS) |
|---|---|---|
| Cough | Common | Absent |
| Rhinorrhea | Present | Absent |
| Exudate | Possible | Common |
| Fever | Variable | Abrupt, high |
| Adenopathy | Posterior > anterior | Anterior cervical |
| Treatment | Supportive | Penicillin/Amoxicillin |
| Complications | Usually none | ARF, abscess, scarlet fever |
Sources:
- Goldman-Cecil Medicine, International Edition (Block 44)
- Tintinalli's Emergency Medicine: A Comprehensive Study (Block 10)
- Goldman-Cecil Medicine - S. pyogenes section
This is a shared conversation. Sign in to Orris to start your own chat.