Detail treatment for liver abscess
Reading File
Finding Sources
Searching PubMed
"liver abscess" AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
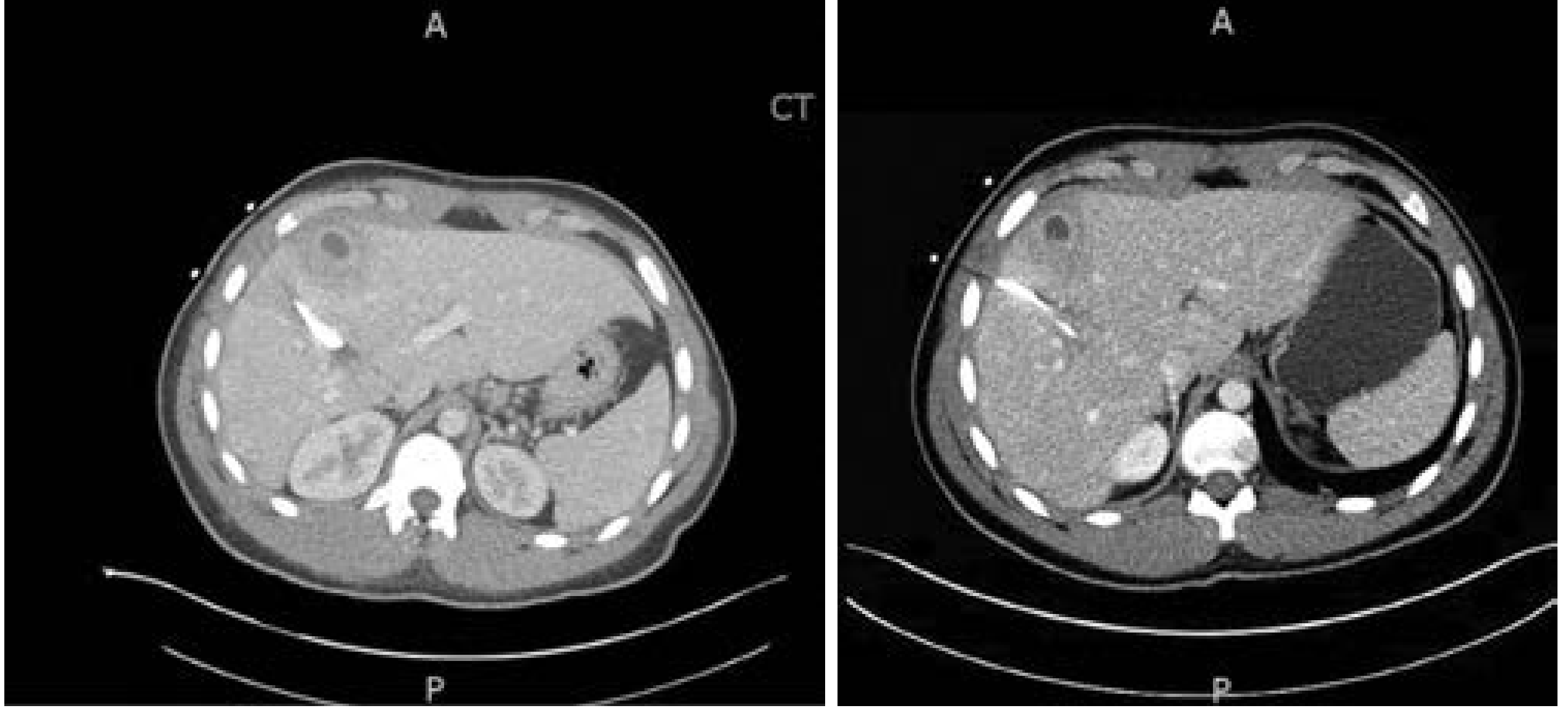
Loading Image
I now have all the information needed for a comprehensive answer. Here is the detailed treatment guide for liver abscess.
Treatment of Liver Abscess
Liver abscess is classified into three main types based on etiology: pyogenic (bacterial), amebic, and fungal. Treatment differs substantially by type. The cornerstone for all types is antimicrobial therapy, with drainage reserved based on size, response, and type.
1. Pyogenic Liver Abscess (PLA)
Step 1 - Cultures Before Antibiotics
Blood cultures are positive in >50% of PLAs and are essential to guide therapy. Abscess fluid cultures should also be obtained at the time of drainage or aspiration. Never start antibiotics before obtaining cultures when feasible. - Current Surgical Therapy 14e, p. 440
Step 2 - Empiric Antibiotic Therapy
Start broad-spectrum antibiotics immediately, covering streptococci, gram-negative bacilli (E. coli, Klebsiella, Pseudomonas), and anaerobes (Bacteroides fragilis).
| Clinical Scenario | Empiric Regimen |
|---|---|
| Standard PLA | Piperacillin/tazobactam (monotherapy) OR Ceftriaxone + metronidazole |
| Prior biliary instrumentation / liver transplant | Carbapenem (meropenem/imipenem) - for ESBL coverage |
| Anaerobic coverage emphasis | Metronidazole or clindamycin (excellent cavity penetration) |
| Gram-negative emphasis | Third-generation cephalosporin or aminoglycoside |
- Sleisenger & Fordtran's GI and Liver Disease: initial coverage with third-generation cephalosporin or fluoroquinolone plus metronidazole; carbapenems and beta-lactam/beta-lactamase inhibitor combinations are valid alternatives.
- Bailey & Love's Short Practice of Surgery: combination of two or more antibiotics recommended; metronidazole/clindamycin for anaerobic coverage, third-generation cephalosporins/aminoglycosides for gram-negative coverage.
Duration: IV antibiotics until clinical response is achieved, then switch to oral antibiotics for up to 6 weeks total, guided by follow-up imaging at 4-6 weeks showing abscess resolution. - Sleisenger & Fordtran's
Step 3 - Drainage
Drainage is standard of care for PLAs. The approach depends on abscess size:
| Abscess Size | Recommended Management |
|---|---|
| < 3 cm | Antibiotics alone (aspiration if technically feasible to guide culture) |
| 3-5 cm | Percutaneous needle aspiration (PNA) - repeated aspirations may be needed |
| > 5 cm | Percutaneous catheter drainage (PCD) - first-line |
| > 10 cm | PCD still preferred; multiple catheters may be needed |
| Multiple abscesses | Drain only the largest; smaller ones often resolve with antibiotics |
Percutaneous catheter drainage (PCD) vs. needle aspiration: A 2023 systematic review and meta-analysis (Lin et al., BMJ Open 2023, PMID 37518084) confirmed PCD has superior outcomes compared to needle aspiration for larger abscesses. A 2025 comparative meta-analysis (Li & Pan, Medicine 2025, PMID 40958348) corroborated this finding.
Catheter management:
- Leave catheter in until output is low and clear for several days
- Watch for bile in the drain - indicates biliary tree communication
- If biliary communication is found, investigate with MRCP or ERCP; may require sphincterotomy or percutaneous biliary drain
Biliary decompression: If the abscess is associated with biliary tract obstruction, biliary decompression via ERCP or the transhepatic route is essential. - Sleisenger & Fordtran's
Step 4 - Surgical Drainage (reserved cases)
Surgery is required in approximately 10-20% of PLAs. Indications include:
- Failure of percutaneous drainage (after appropriate trial)
- Large multiloculated abscesses not amenable to PCD
- Ruptured abscess with peritonitis
- Concurrent intra-abdominal pathology (e.g., diverticulitis requiring surgery)
- Unresolved jaundice, renal impairment, incomplete percutaneous drainage
- Abscess communication with the biliary tree not manageable endoscopically
Minimally invasive (laparoscopic) approach is preferred when feasible. There is no evidence that hepatic resection is superior to surgical drainage with irrigation, and manipulation of a septic liver carries risk of acute septic shock. - Current Surgical Therapy 14e, p. 441
Outcomes & Prognosis
Mortality now ranges 4-10% with modern management. Worse prognosis with: delay in diagnosis, multiple abscesses, polymicrobial bacteremia, fungal cause, shock, jaundice, hypoalbuminemia, pleural effusion, biliary malignancy, multiorgan dysfunction, diabetes, or cirrhosis.
Complications include: empyema, pleural/pericardial effusion, portal/splenic vein thrombosis, rupture into pericardium, thoraco-abdominal fistula, and sepsis. Notably, metastatic septic endophthalmitis occurs in up to 10% of diabetic patients with K. pneumoniae liver abscess. - Sleisenger & Fordtran's
2. Amebic Liver Abscess (ALA)
Caused by Entamoeba histolytica. Always consider in patients with travel to endemic regions (Africa, Southeast Asia, Mexico, Central/South America). Classic abscess contents are described as "anchovy paste." Eosinophilia is not typically seen.
Antibiotic Treatment
Metronidazole is the drug of choice:
- 500-750 mg orally, three times daily for 7-10 days
- Clinical improvement (reduction in pain and fever) expected within 72 hours
-
90% of patients respond to this regimen
- Longer-acting nitroimidazoles (tinidazole, ornidazole) work as single-dose therapy in developing countries
Mandatory luminal agent to eradicate intestinal cysts and prevent recurrence (as ~72% of ALA patients have bowel E. histolytica co-infection even without GI symptoms):
- Paromomycin 10 mg/kg orally, three times daily for 7 days, OR
- Diiodohydroxyquin 650 mg orally, three times daily for 20 days
Treatment duration for ALA is standardized (unlike PLAs which require imaging resolution). Repeat imaging is recommended but abscess resolution may take months and is NOT required for antibiotic cessation. - Current Surgical Therapy 14e, Harrison's 22E
Drainage for ALA
Aspiration/drainage is NOT routinely recommended for ALA - prospective studies have failed to show benefit to early drainage. Indications to aspirate:
- Need to rule out pyogenic abscess (especially with multiple lesions)
- No clinical response within 3-5 days of metronidazole therapy
- Threat of imminent rupture
- Left-lobe abscesses threatening pericardial rupture
Even large abscesses (up to 10 cm) do not require drainage if the patient is responding clinically. If response fails, broaden to cover bacteria (possible secondary infection) and pursue PCD. Surgery is reserved for bowel perforation or pericardial rupture. - Harrison's Principles of Internal Medicine 22E
3. Fungal Hepatic Abscess
Almost exclusively in immunocompromised patients: liver/hematopoietic stem cell transplant recipients, HIV patients, and those with hepatobiliary malignancy. Most commonly caused by Candida spp.
Treatment
- Empiric antifungal therapy: amphotericin B OR an echinocandin (caspofungin or micafungin)
- Tailor to culture data when available
- Percutaneous drainage follows the same principles as PLA
- Duration guided by resolution on imaging
- Antifungal prophylaxis in transplant patients has improved mortality
- Overall mortality remains high (~20% even with treatment; ~50% mortality from disseminated infection in historical series)
Prompt recognition is critical - maintain a high index of suspicion in at-risk patients. - Current Surgical Therapy 14e
Summary Decision Framework
Liver Abscess Suspected
│
├─ Obtain: Blood cultures, abscess cultures (if draining)
│
├─ Travel history / serology → Amebic?
│ YES → Metronidazole + luminal agent
│ Drain only if: no response at 3-5 days, rupture risk, left lobe, rule out PLA
│
├─ Immunocompromised? → Consider Fungal
│ Empiric: Amphotericin B or echinocandin + PCD
│
└─ Pyogenic (most common)
├─ Start empiric broad-spectrum antibiotics
├─ Size < 3 cm → Antibiotics alone
├─ 3-5 cm → PNA (repeated as needed)
├─ > 5 cm → PCD (leave catheter until drainage clears)
├─ Biliary obstruction → Biliary decompression (ERCP/PTBD)
└─ PCD failure / ruptured → Surgical drainage
Sources: Current Surgical Therapy 14e (pp. 440-442); Sleisenger & Fordtran's GI and Liver Disease; Bailey & Love's Short Practice of Surgery 28e; Harrison's Principles of Internal Medicine 22E (2025)
This is a shared conversation. Sign in to Orris to start your own chat.