HFrEF and HFpEF difference
Reading File
Finding Sources
Finding Sources
Searching PubMed
"heart failure" AND "HFrEF" AND "HFpEF" AND differences
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive comparison of HFrEF vs HFpEF based on Goldman-Cecil Medicine, Braunwald's Heart Disease, and Harrison's Principles of Internal Medicine (22nd ed, 2025):
HFrEF vs HFpEF: Key Differences
1. Definition & EF Cutoffs
| Feature | HFrEF | HFpEF | HFmrEF (borderline) |
|---|---|---|---|
| LVEF | <40% | ≥50% | 41-49% |
| Former name | Systolic HF | Diastolic HF | Borderline / Mid-range EF |
2. Pathophysiology
HFrEF - Goldman-Cecil Medicine, p. 466:
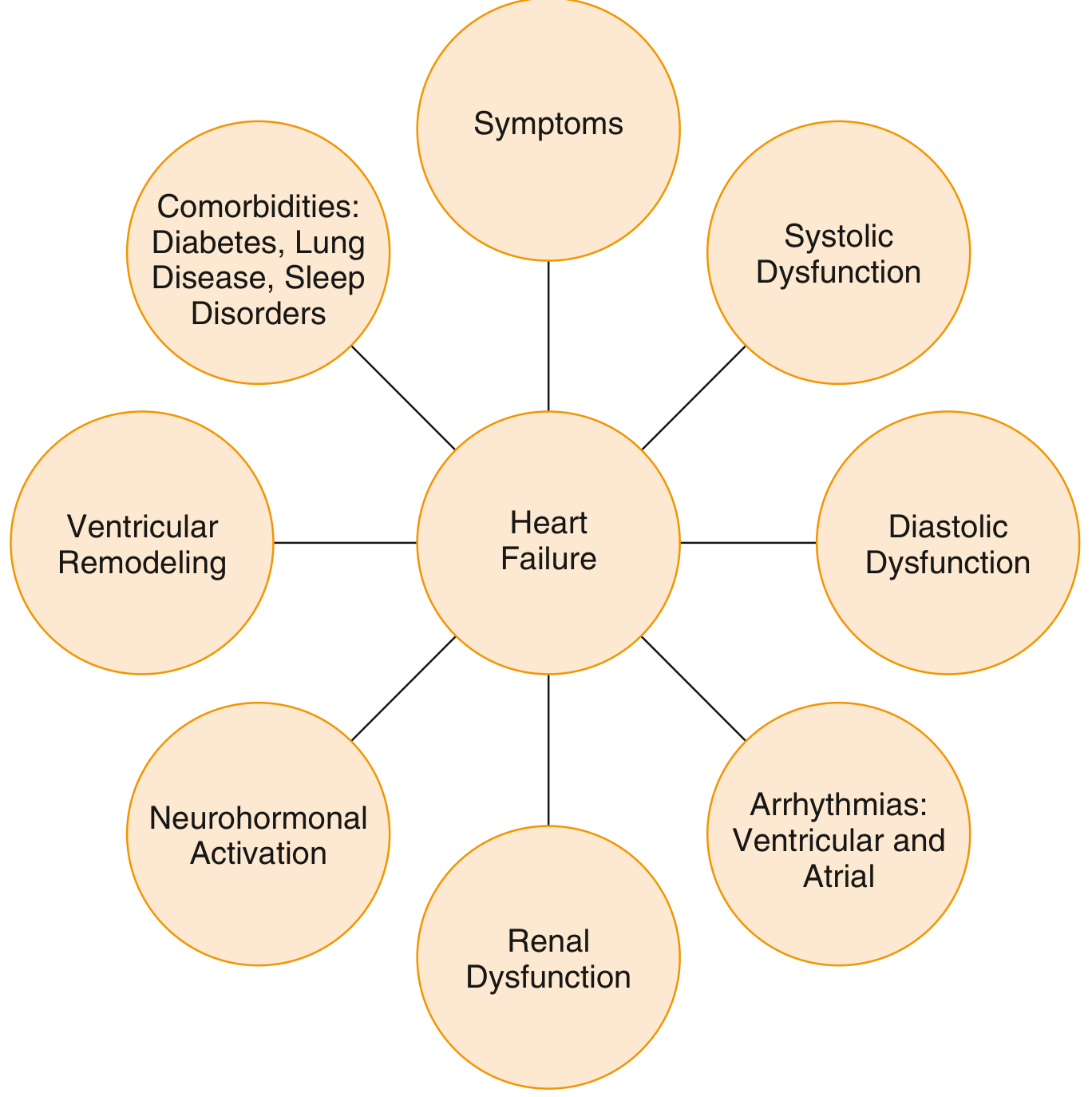
- The core problem is impaired contractility: maladaptive neurohormonal activation (SNS + RAAS) drives prototypical ventricular remodeling - chamber dilation, wall thinning, increased sphericity
- Abnormal calcium cycling: reduced SR calcium content via altered ryanodine receptors + loss of SERCA2a function impairs both contraction and relaxation
- Elevated catecholamines downregulate beta-adrenergic receptors and are directly cardiotoxic
- Replacement fibrosis, TNF-alpha, IL-1beta, IL-6 drive myocyte necrosis and further systolic impairment
- RAAS activation causes vasoconstriction and sodium retention, worsening remodeling over time
HFpEF - Goldman-Cecil Medicine, p. 467:
- The core problem is impaired relaxation (diastole): increased ventricular stiffness from LV hypertrophy + interstitial fibrosis + abnormal calcium cycling
- Most patients have prior/current hypertension - resulting LVH and fibrosis cause rigid chamber walls that cannot fill normally
- Ischemic heart disease contributes via subendocardial fibrosis
- Aging is a major predisposing factor: myocyte apoptosis, shifts to more rigid collagen types, loss of vascular compliance
- Myocardial relaxation is energy-dependent; any process compromising energy metabolism (ischemia) worsens diastolic filling
3. Epidemiology & Demographics
| Feature | HFrEF | HFpEF |
|---|---|---|
| Sex | More common in men | More common in women |
| Age | Younger patients | Older patients |
| Prevalence trend | Declining relative proportion | Increasing - now ~50% of all HF |
| Primary driver | CAD, prior MI | Hypertension, aging, obesity, diabetes |
From Braunwald's Heart Disease, community-based US studies show ~50% of hospitalized HF patients have LVEF >50%, and the proportion with preserved EF increased from 33% (2005) to 39% (2010), with projections to 65% by 2020, making HFpEF the predominant form in aging societies.
4. Common Causes/Etiologies
| HFrEF | HFpEF |
|---|---|
| Coronary artery disease / prior MI (most common in industrialized countries) | Systemic hypertension with LVH |
| Dilated cardiomyopathy (idiopathic, genetic) | Hypertrophic cardiomyopathy |
| Toxic (alcohol, chemotherapy - e.g., trastuzumab) | Infiltrative disease (amyloidosis, sarcoidosis) |
| Myocarditis | Ischemic heart disease (subendocardial fibrosis) |
| Tachycardia-induced cardiomyopathy (potentially reversible) | Restrictive cardiomyopathy |
| Chagas disease (Central/South America) | Aging-related fibrosis |
5. Clinical Features
Both share the same symptoms (dyspnea, orthopnea, PND, fatigue, edema), but differ in some key signs:
- HFrEF: S3 gallop, laterally displaced PMI (dilated ventricle), more prominent jugular venous distension
- HFpEF: S4 gallop (stiff ventricle), normal or small LV cavity on echo, more sensitive to volume loading/depletion - modest volume overload greatly worsens symptoms; diuresis can cause hypotension
HFpEF patients often present with multiple comorbidities: obesity, diabetes, atrial fibrillation, obstructive sleep apnea, CKD.
6. Biomarkers
Both elevate BNP/NT-proBNP, but levels tend to be lower in HFpEF (especially in obese patients, where BNP is suppressed by adipose tissue). Natriuretic peptides counterbalance vasoconstriction/sodium retention in both - Goldman-Cecil Medicine, p. 466.
7. Treatment - The Critical Difference
This is where HFrEF and HFpEF differ most dramatically:
HFrEF: Multiple disease-modifying therapies proven to reduce mortality (Goldman-Cecil Medicine, Braunwald's):
- RAAS blockade: ACE inhibitors or ARBs; or preferably ARNI (sacubitril/valsartan)
- Beta-blockers: carvedilol, metoprolol succinate, bisoprolol
- Mineralocorticoid receptor antagonists (MRA): spironolactone, eplerenone
- SGLT2 inhibitors: dapagliflozin, empagliflozin (also reduce hospitalization + mortality)
- Diuretics: for fluid control (symptom relief but no mortality benefit)
- Digoxin: reduces hospitalizations in sinus rhythm
- Device therapy: ICD (sudden death prevention), CRT (for LBBB/wide QRS)
- Long-chain omega-3 PUFAs: modestly improved outcomes (GISSI-HF trial)
HFpEF: No therapy has conclusively shown mortality benefit (Harrison's 22E, p. 2031):
- Attempts to export HFrEF drugs (ACE inhibitors, ARBs, beta-blockers, digoxin) to HFpEF have generally failed to reduce mortality
- SGLT2 inhibitors (dapagliflozin, empagliflozin 10 mg/day) are the current primary pharmacologic therapy - reduce HF hospitalizations and improve quality of life; also effective in HFmrEF
- MRA (spironolactone): TOPCAT trial showed no improvement in primary composite endpoint but did reduce HF hospitalizations; benefit was principally in those with LVEF closer to 50%
- ARBs (candesartan, irbesartan): CHARM-Preserved showed reduced HF hospitalizations but no mortality benefit; I-PRESERVE showed no benefit
- ARNI (sacubitril/valsartan): possible benefit especially at lower EF ranges (PARAGON-HF)
- GLP-1 agonists: emerging evidence in obese HFpEF patients (e.g., semaglutide - STEP-HFpEF)
- Diuretics: for symptom control
- Treat underlying causes: hypertension, atrial fibrillation (rate/rhythm control), obesity, sleep apnea, diabetes, myocardial ischemia
- Ivabradine and isosorbide mononitrate have no benefit in HFpEF; isosorbide mononitrate actually worsens activity levels
8. Quick Summary Table
| Feature | HFrEF | HFpEF |
|---|---|---|
| EF | <40% | ≥50% |
| Primary dysfunction | Systolic (impaired contraction) | Diastolic (impaired relaxation/filling) |
| Ventricle morphology | Dilated, thin-walled | Concentric hypertrophy, small cavity |
| Dominant sex | Male | Female |
| Main etiology | CAD, dilated CMP | Hypertension, aging, obesity |
| Neurohormonal activation | Prominent RAAS + SNS | Less prominent, more metabolic/inflammatory |
| Mortality-reducing drugs | Multiple (ACEi/ARB/ARNI, BB, MRA, SGLT2i) | None proven; SGLT2i reduce hospitalizations |
| BNP | High (often very high) | Elevated but typically lower |
| Prognosis | Poor; 50% 5-year mortality | Similar or slightly worse long-term due to comorbidities |
Sources: Goldman-Cecil Medicine International Edition (pp. 465-470); Braunwald's Heart Disease, 2-Vol Set (Ch. 51); Harrison's Principles of Internal Medicine 22E (2025), Ch. 28.
This is a shared conversation. Sign in to Orris to start your own chat.