Tell me g6pd deficiency 5 mark qution in medicine MBBS
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive 5-mark MBBS answer. Let me compile it.
G6PD Deficiency - 5 Mark Question (MBBS Medicine)
Definition
Glucose-6-Phosphate Dehydrogenase (G6PD) deficiency is the most common inherited enzyme deficiency in humans, affecting over 400 million people worldwide. It is an X-linked recessive disorder where deficiency of the G6PD enzyme renders red blood cells (RBCs) unable to withstand oxidative stress, leading to hemolytic anemia.
(Harrison's Principles, 22E; Lippincott Biochemistry, 8E)
Pathophysiology
G6PD is the rate-limiting enzyme of the Pentose Phosphate Pathway (PPP). In RBCs, the PPP is the only source of NADPH.
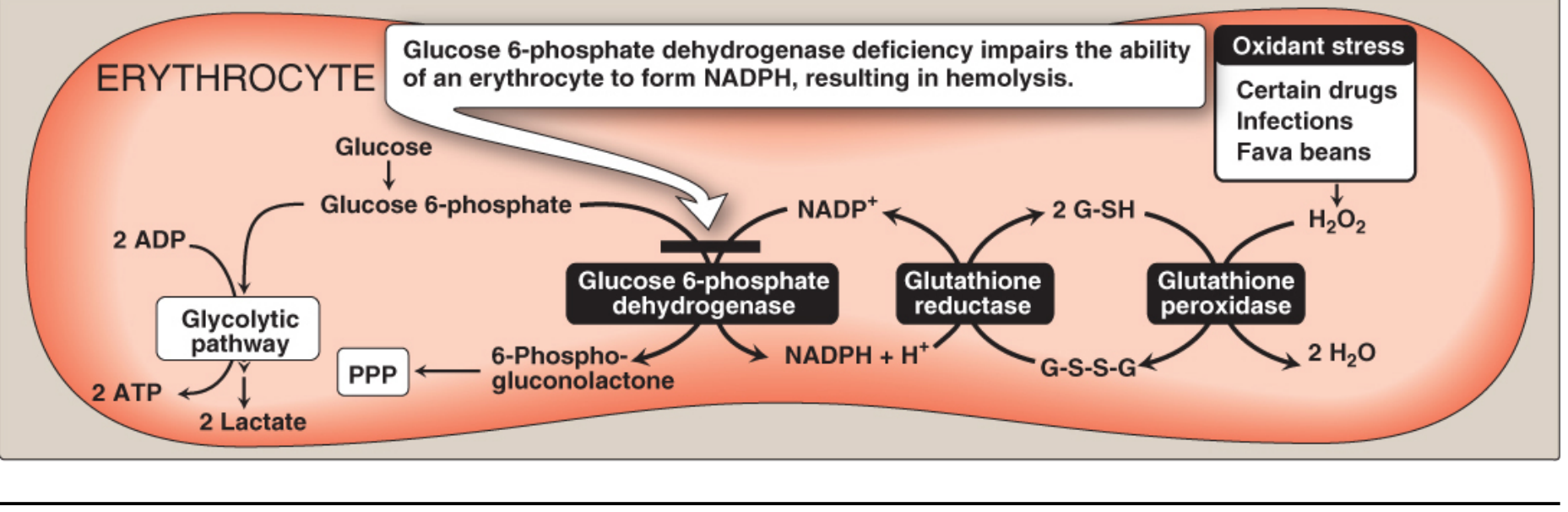
The chain of events:
- G6PD converts Glucose-6-phosphate → 6-Phosphogluconolactone + NADPH
- NADPH keeps glutathione in its reduced active form (G-SH)
- Reduced glutathione neutralizes H₂O₂ via glutathione peroxidase
- When G6PD is deficient → less NADPH → glutathione becomes oxidized (G-S-S-G) → H₂O₂ accumulates → oxidation of hemoglobin → Heinz body formation → membrane damage → hemolysis
RBCs are especially vulnerable because they have no mitochondria or nucleus - they cannot regenerate the enzyme or use alternative NADPH-generating pathways.
(Lippincott Biochemistry, 8E; Goldman-Cecil Medicine)
Genetics
- X-linked recessive - gene locus at Xq28
- Predominantly affects males (hemizygous); females are mostly carriers
- Over 400 variants described; most are missense point mutations
- Common variants:
- G6PD A- (Africa) - Class III, enzyme activity 10-23%
- G6PD Mediterranean (Middle East, South Asia) - Class II, activity <5%, more severe
- G6PD Canton (Asia) - Class II, similar to Mediterranean
(Goldman-Cecil Medicine, Harrison's 22E)
WHO Classification (5 Classes)
| Class | Clinical Severity | Residual Enzyme Activity |
|---|---|---|
| I | Congenital nonspherocytic hemolytic anemia (CNSHA) | <10% |
| II | Severe - acute hemolytic anemia (e.g., G6PD Mediterranean) | <10% |
| III | Moderate - hemolysis only after oxidant stress (e.g., G6PD A-) | 10-60% |
| IV | No clinical symptoms (e.g., G6PD B normal) | >60% |
| V | Overproduction of G6PD (asymptomatic) | >100% |
Classes II and III together represent >90% of G6PD variants.
Precipitating Factors (Triggers)
- Drugs (the most important "4 A's" - Antibiotics, Antimalarials, Analgesics, Antipyretics):
- Antimalarials: Primaquine, Pamaquine, Chloroquine
- Sulfonamides / Sulfones: Dapsone, Sulfamethoxazole-TMP (Co-trimoxazole), Sulfanilamide
- Other antibiotics: Nitrofurantoin, Chloramphenicol, Nalidixic acid
- Analgesics: Aspirin (high dose), Phenacetin
- Miscellaneous: Rasburicase, Methylene blue
- Fava beans (Favism) - especially G6PD Mediterranean variant
- Infections - most common trigger; inflammatory response generates free radicals in macrophages that diffuse into RBCs
- Neonatal period - neonatal jaundice
Clinical Features
1. Acute Hemolytic Anemia (AHA)
- Onset 24-72 hours after oxidant exposure
- Symptoms: fever, malaise, nausea, abdominal pain, back pain
- Dark urine (hemoglobinuria), jaundice
- Pallor, tachycardia
- Hepatosplenomegaly may be present
- Severe cases: acute renal failure, congestive heart failure
2. Neonatal Jaundice (NNJ)
- Appears 1-4 days after birth
- May be severe, requiring phototherapy or exchange transfusion
- Risk of kernicterus if untreated
3. Congenital Nonspherocytic Hemolytic Anemia (CNSHA)
- Rare, Class I variants only
- Chronic hemolysis even without oxidant trigger
- Pallor, splenomegaly, gallstones (pigment)
Laboratory Findings
- CBC: Normochromic, normocytic anemia; reticulocytosis
- Peripheral blood smear: Bite cells (blister cells), poikilocytes, Heinz bodies (on supravital staining with crystal violet) - represent precipitated, denatured hemoglobin
- Elevated bilirubin (indirect), raised LDH, reduced haptoglobin
- Hemoglobinuria (dark urine)
- G6PD assay: Quantitative spectrophotometric assay (definitive test) - measure enzyme activity. Note: May be falsely normal during acute hemolysis due to preferential lysis of older enzyme-depleted cells; repeat after 3 months.
- Fluorescent spot test: Screening test (NADPH fluoresces under UV light)
Management
-
Preventive (most important):
- Avoid known triggering drugs and foods (fava beans)
- Screen before prescribing oxidant drugs (esp. primaquine, dapsone)
-
Acute hemolytic episode:
- Remove the offending agent / treat underlying infection
- Supportive care: IV fluids, maintain urine output to prevent renal failure
- Blood transfusion if anemia is severe (Hb <7 g/dL or symptomatic)
- Hemodialysis if acute renal failure develops
- Phototherapy or exchange transfusion for neonatal jaundice
-
CNSHA (Class I):
- Folic acid supplements
- Regular hematologic surveillance
- Avoid hemolytic drugs
- Splenectomy in severe cases
Why G6PD Deficiency Persists in Populations (Evolutionary Advantage)
G6PD-deficient RBCs infected by Plasmodium falciparum undergo increased oxidative stress → premature lysis → protective against severe malaria. This explains the high prevalence in malaria-endemic regions (Africa, Mediterranean, South/Southeast Asia).
Sources: Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine, 22E; Lippincott Illustrated Reviews: Biochemistry, 8E
This is a shared conversation. Sign in to Orris to start your own chat.