Whipples procedure steps
Reading File
Finding Sources
Searching the Web
Whipple procedure pancreaticoduodenectomy surgical steps
Reading File
Finding Sources
Reading Web Page
https://www.sciencedirect.com/science/article/pii/S258984502…
Finding Sources
Reading Web Page
https://www.ncbi.nlm.nih.gov/books/NBK560747
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a detailed, step-by-step account of the Whipple procedure (pancreaticoduodenectomy), drawn from Fischer's Mastery of Surgery 8e and Schwartz's Principles of Surgery 11e.
Whipple Procedure (Pancreaticoduodenectomy) - Operative Steps
Overview
The Whipple procedure removes the pancreatic head and uncinate process, duodenum, proximal jejunum, gallbladder, distal bile duct, and (in the classic variant) the gastric antrum. The pylorus-preserving variant (PPPD) spares the antrum and divides the duodenum 2 cm distal to the pylorus instead.
PHASE 1 - Preoperative & Entry
Staging laparoscopy (selective)
- In patients with elevated CA 19-9 or questionable lesions on imaging, diagnostic laparoscopy is performed first to exclude occult peritoneal or liver metastases before committing to laparotomy.
Incision
- Upper midline incision (standard). A bilateral subcostal (chevron) incision is used selectively in obese patients or those with prior lower abdominal surgery.
- The umbilical ligament is divided and dissected back to the umbilical fissure of the liver. This pedicled flap is preserved for later coverage of the gastroduodenal artery (GDA) stump.
Exploration
- Full abdominal exploration to confirm no metastatic disease (liver, peritoneum, lymph nodes).
- A self-retaining retractor (e.g., Thompson Surgical System) is placed.
PHASE 2 - Resection (6 Steps per Evans et al.)
Step 1 - Entry into the lesser sac and SMV identification
- The lesser sac is entered through the gastrocolic ligament.
- The hepatic flexure of the colon is taken down.
- The gastrocolic trunk is divided.
- The inferior border of the pancreatic body is identified and the visceral peritoneum incised from left to right toward the SMV.
- The infrapancreatic superior mesenteric vein (SMV) is carefully exposed at the inferior border of the pancreatic neck, near the uncinate process.
- If venous resection is anticipated or the patient is morbidly obese, a Cattell-Braasch maneuver (mobilization of the entire right colon and small bowel mesentery root) may be performed.
Step 2 - Kocher maneuver
- The peritoneum lateral to the duodenum is incised.
- The duodenum and pancreatic head are mobilized off the retroperitoneum (Kocher maneuver), exposing the inferior vena cava (IVC) and left renal vein.
- This allows palpation for vascular involvement and access to the SMA origin.
- Note: Resectability is now primarily determined by preoperative imaging, not intraoperative palpation.
Step 3 - Cholecystectomy and bile duct division
- The gallbladder is mobilized from the liver, and the cystic duct and artery are ligated and divided.
- The common hepatic duct is circumferentially dissected and divided just above the cystic duct entry point.
- The bile duct is then dissected inferiorly toward the duodenum; inferior traction on the distal bile duct exposes the anterior portal vein.
- The GDA is ligated and divided at its origin from the hepatic artery after confirming hepatic artery patency (a test clamp is applied with confirmation of a hepatic artery pulse).
Step 4 - Gastric or duodenal division
- Classic Whipple: The antrum is divided and the distal stomach resected.
- Pylorus-preserving (PPPD): The duodenum is divided 2 cm distal to the pylorus with a GI stapler.
Step 5 - Jejunal division
- The jejunum is divided approximately 10 cm distal to the ligament of Treitz using a GI stapler.
- The jejunal mesentery is divided at the serosa/mesentery junction using an energy device - great care is taken here to avoid inadvertent SMA ligation as the bowel passes posterior to the SMA.
- The duodenum and proximal jejunum are then delivered under the mesenteric vessels from left to right.
Step 6 - Pancreatic neck transection and uncinate process dissection
- A retropancreatic tunnel is created anterior to the portal vein behind the pancreatic neck using a blunt-tipped clamp.
- Hemostatic sutures are placed on both the superior and inferior sides of the planned transection line.
- The pancreatic neck is divided with electrocautery anterior to the portal vein (cautery is avoided near the pancreatic duct).
- The SMV is mobilized; small venous branches from the uncinate process draining into the portal vein/SMV are ligated individually.
- The SMV is retracted medially, exposing the SMA beneath it.
- A periadventitial dissection plane is developed along the SMA from caudal to cranial - all fibrofatty, lymphatic, and perineural tissue to the right and anterior to the SMA is taken with the specimen (critical for oncological clearance).
- Multiple inferior pancreaticoduodenal arteries (IPDA) from the SMA are individually suture-ligated.
- The uncinate process is freed from behind the SMV and SMA, completing the resection. The specimen is removed.
PHASE 3 - Reconstruction
Reconstruction restores three anastomotic connections using a single Roux limb of jejunum brought through the transverse mesocolon (retrocolic) or anterior to it (antecolic):
1. Pancreaticojejunostomy (PJ) - most proximal
The pancreatic remnant is anastomosed to the jejunum. Two main techniques:
- Duct-to-mucosa (end-to-side): The pancreatic duct is sutured directly to the jejunal mucosa with an inner layer of interrupted absorbable sutures. An outer layer approximates the pancreatic capsule to the seromuscular layer of the jejunum. This is the preferred technique for soft pancreas or small duct.
- Dunking (invagination) anastomosis: The pancreatic stump is intussuscepted (dunked) into the end of the jejunum - can be terminoterminal or terminolateral.
- A pancreaticogastrostomy (PG) is an alternative to PJ, anastomosing the pancreatic remnant to the posterior stomach wall.
2. Hepaticojejunostomy (HJ) - 10-15 cm distal to PJ
- The common hepatic duct stump is anastomosed end-to-side to the jejunum with a single layer of interrupted absorbable sutures.
3. Gastrojejunostomy or Duodenojejunostomy - most distal
- Classic Whipple: A gastrojejunostomy is created (side-to-side or end-to-side) approximately 40-60 cm distal to the HJ - usually antecolic to avoid compression.
- PPPD: A duodenojejunostomy is created, restoring pyloric continuity.
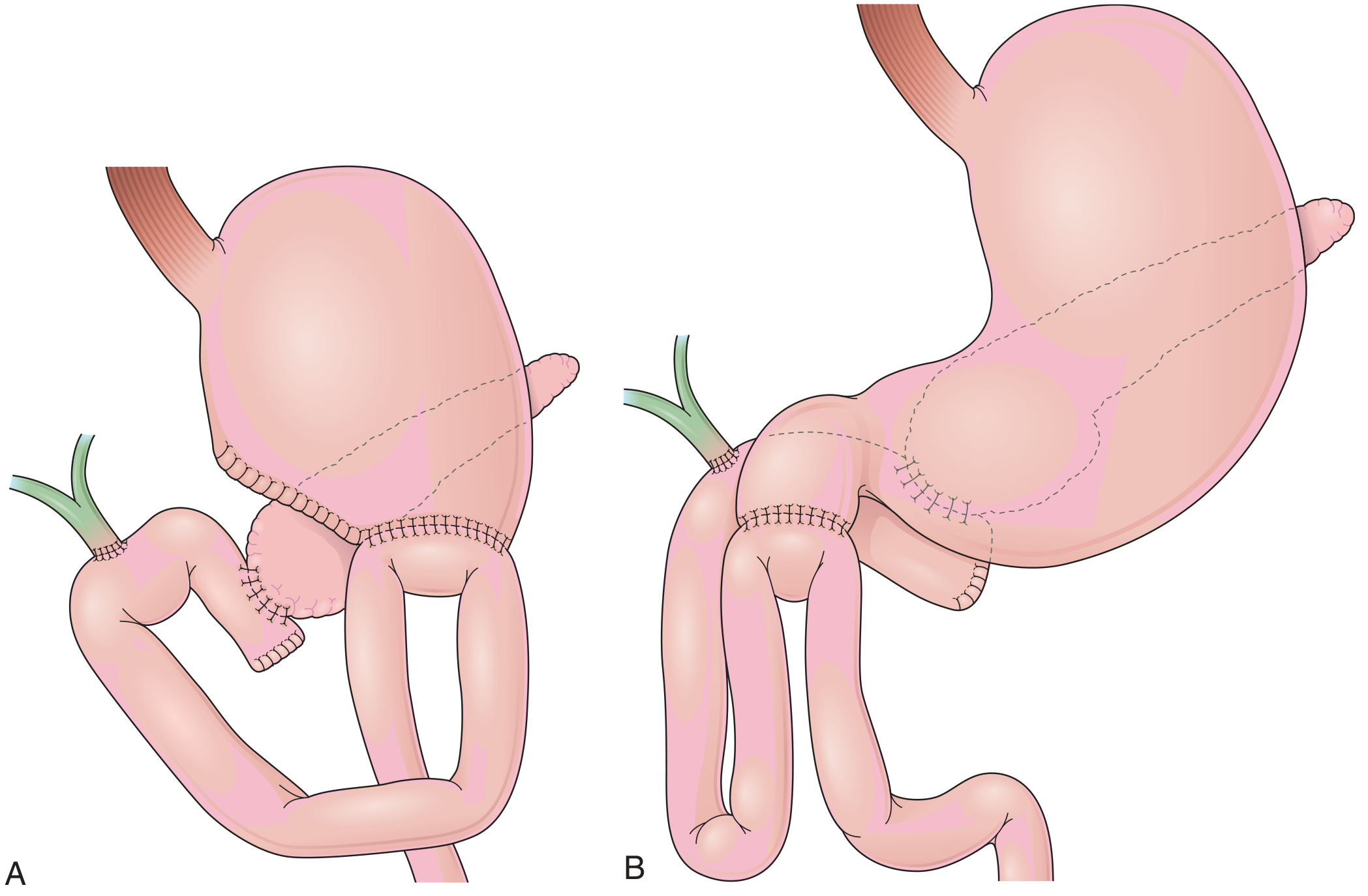
Fig 12.13 - Classic Whipple (A) vs. Pylorus-Preserving Whipple (B) - Clinical Gastrointestinal Endoscopy 3e, p.189
PHASE 4 - Closure
- Abdominal drains are placed near the pancreatic and biliary anastomoses (selective vs. routine placement remains debated; a randomized multicenter trial supported drain placement for patients who develop postoperative leaks).
- The umbilical ligament pedicle flap may be sutured over the GDA stump to protect against postoperative hemorrhage from stump blowout.
- Fascial and skin closure.
Classic vs. Pylorus-Preserving: Key Differences
| Feature | Classic Whipple | PPPD |
|---|---|---|
| Gastric division | Antrum resected | Duodenum divided 2 cm distal to pylorus |
| Gastric anastomosis | Gastrojejunostomy | Duodenojejunostomy |
| Oncologic margin | Slightly wider | Equivalent for most tumors |
| Delayed gastric emptying | Less common | More common historically |
Key Complications to Know
- Postoperative pancreatic fistula (POPF) - most common major complication; results from pancreaticojejunostomy leak. Graded A/B/C by ISGPF criteria.
- Delayed gastric emptying (DGE) - especially with PPPD.
- Post-pancreatectomy hemorrhage - may be from GDA stump or pseudoaneurysm.
- Bile leak from hepaticojejunostomy.
- Wound infection / intra-abdominal abscess.
Sources: Fischer's Mastery of Surgery 8e, Chapter 183 (Surgical Technique) | Schwartz's Principles of Surgery 11e, Chapter 33 | Clinical Gastrointestinal Endoscopy 3e, p.189
This is a shared conversation. Sign in to Orris to start your own chat.