Nevus flameus
Reading File
Finding Sources
Finding Sources
Searching PubMed
"nevus flammeus" OR "port wine stain"
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have comprehensive information. Here is the full structured answer:
Nevus Flammeus (Port-Wine Stain / Capillary Malformation)
Terminology
Nevus flammeus (Latin: "flame nevus") is the classical name for what is now formally classified as a capillary malformation (CM) - a slow-flow vascular malformation of the skin. Common synonyms include port-wine stain (PWS) or port-wine birthmark (the currently preferred term by the ISSVA). Note that "nevus flammeus neonatorum" (also called nevus simplex, salmon patch, stork bite, or angel's kiss) is a separate, benign transient entity that must not be confused with true CM.
Epidemiology
- Prevalence: ~0.3% of the population
- No sex preponderance
- Most cases are sporadic (somatic mutation), but inherited (autosomal dominant, multiple) forms exist as part of the CM-AVM syndrome
(Fitzpatrick's Dermatology, p. 2668)
Clinical Features
Nevus Flammeus Neonatorum (Figure A below - the transient neonatal variant):

Figure: (A) Facial nevus flammeus neonatorum. (B) Unna nevus on the nape of the neck - both are transient variants. - Fitzpatrick's Dermatology
True Capillary Malformation (Port-Wine Stain):
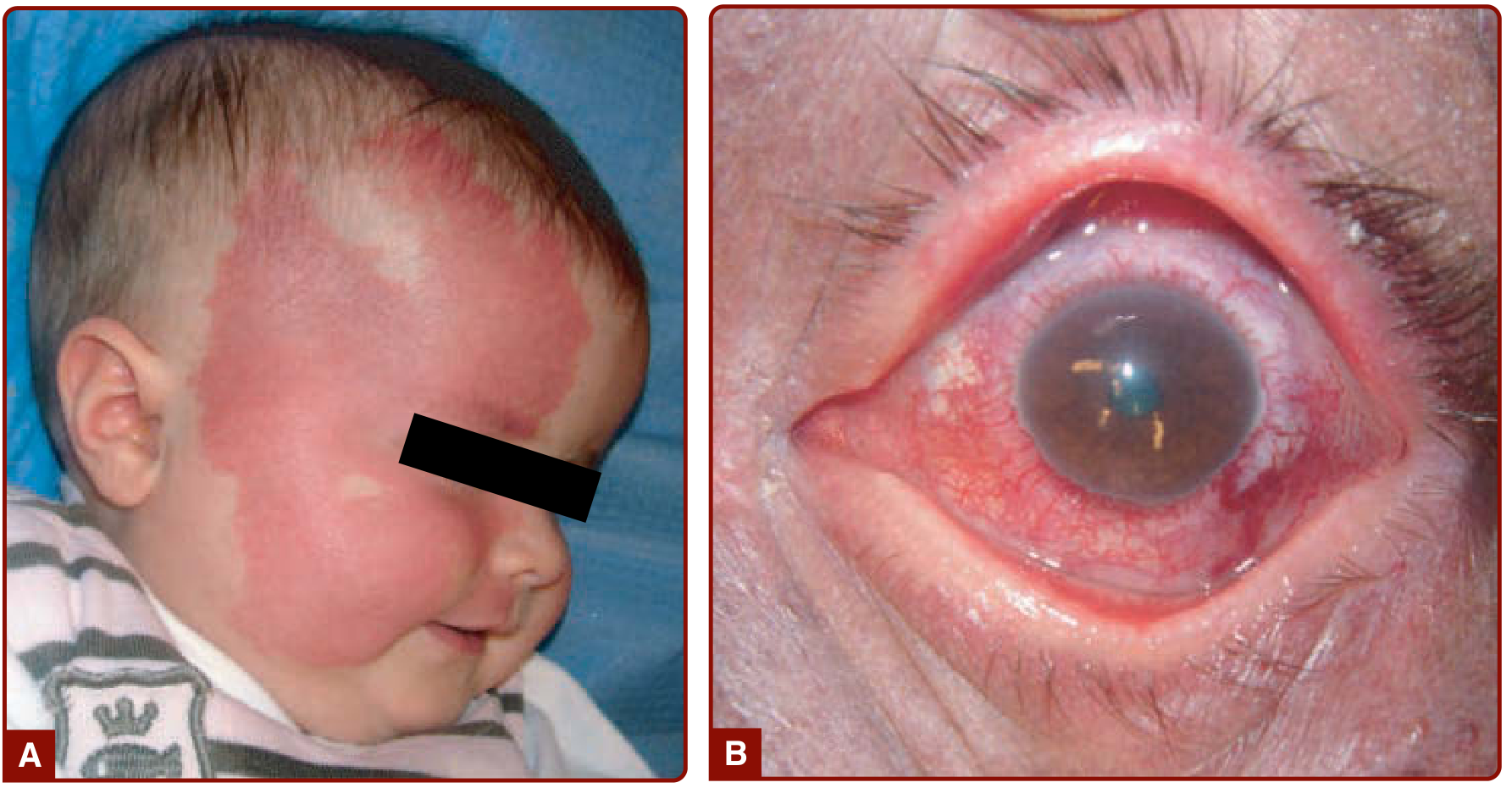
Figure: (A) Extensive right facial CM involving V1/V2 trigeminal branches in Sturge-Weber syndrome. (B) Choroidal CM with glaucoma. - Fitzpatrick's Dermatology
| Feature | Description |
|---|---|
| Appearance | Red-to-deep purple, flat, homogenous, geographic or dermatomal |
| Onset | Congenital, present at birth |
| Location | 50% on face (trigeminal distribution: V1, V2, V3); also extremities, trunk |
| Laterality | Often unilateral |
| Temperature | Normal (cold; never warm - distinguishes from AVM) |
| Blanching | Does NOT blanch completely |
| Pain/bleeding | Flat and painless; no spontaneous bleeding |
| Course | Persists lifelong and progressively darkens to purple; soft tissue hypertrophy develops over time |
(Fitzpatrick's Dermatology, p. 2669; Kanski's Clinical Ophthalmology, p. 63)
The palate/oral mucosa can also be involved, as seen here:

Figure: Mucosal port-wine stain of the palate - Andrews' Diseases of the Skin
Pathogenesis & Genetics
- Sporadic CM: caused by somatic activating mutations in GNAQ (a G-protein alpha subunit mediating signals between G-protein-coupled receptors and downstream effectors). The same mutations drive Sturge-Weber syndrome (SWS).
- Clonal expansion of abnormal neural-crest-derived cells is the proposed mechanism for facial CM.
- Phakomatosis pigmentovascularis (PPV): mutations in GNAQ or GNA11 lead to combined CM + pigmented nevus.
- Inherited CM-AVM1: inactivating mutations in RASA1 (GTPase-activating protein, negatively regulates Ras).
- Inherited CM-AVM2: inactivating mutations in EPHB4 (regulates arteriovenous identity, interacts with RASA1 via RAS-MAPK signaling).
- M-CM (Macrocephaly-CM): activating mutations in AKT3, PIK3CA, PIK3R2.
(Fitzpatrick's Dermatology, p. 2671)
Histology
- Dilated capillaries of the papillary and upper reticular dermis
- Areas of increased number of otherwise normal-appearing capillaries
- Endothelial cells are flat
- Factor VIII, fibronectin, and basement membrane proteins are normal
- S100 staining shows abnormal innervation (key finding)
- Immunohistochemistry: D2-40 negative (distinguishes from lymphatic malformation)
(Fitzpatrick's Dermatology, p. 2671; Kanski's Clinical Ophthalmology)
Complications
- Soft tissue hypertrophy - especially V2/V3 dermatomes; affects lips, gums, maxilla/mandible - leading to skeletal asymmetry, occlusal tilt, open-bite deformity
- Pyogenic granulomas - lobular vascular overgrowths that can bleed; arise within the PWS especially during adolescence
- Purple nodules and verrucous/cobblestone thickening of the skin over time
- Meyerson phenomenon - atopic dermatitis, psoriasis, or acne is worse within the CM area
- Ocular - glaucoma, episcleral hemangioma, choroidal hemangioma (in SWS)
- Leg-length discrepancy when extremities involved
(Fitzpatrick's Dermatology, p. 2671)
Associated Syndromes
| Syndrome | Key Features |
|---|---|
| Sturge-Weber Syndrome (SWS) | Facial CM (V1 ± V2/V3) + ipsilateral leptomeningeal angioma (seizures, hemiparesis, hemianopia) + ipsilateral glaucoma |
| Klippel-Trenaunay Syndrome | CM + varicosities + limb hypertrophy |
| Proteus Syndrome | CM + hemihypertrophy + macrodactyly + epidermal nevus + cerebriform plantar overgrowth |
| Phakomatosis Pigmentovascularis | CM + pigmented nevus (nevus spilus, Ota) ± systemic involvement |
| CM-AVM Syndrome | Multiple atypical CMs + AVMs (RASA1/EPHB4 mutations) |
| Macrocephaly-CM (M-CM) | CM + macrocephaly (PIK3CA, AKT3) |
| TAR Syndrome | Thrombocytopenia + absent radius + occasionally PWS |
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Nevus flammeus neonatorum (salmon patch) | Median location (glabella, nape, eyelids), fades by 1-4 years |
| Infantile hemangioma | Appears weeks after birth, raised, grows rapidly then involutes |
| Telangiectasia | Fine red vessels, not a solid patch |
| CMTC (Cutis Marmorata Telangiectatica Congenita) | Marbled blue-red pattern, often with skin atrophy |
| CM-AVM | Multiple, smaller, atypical CMs; inherited |
Diagnosis
- Clinical diagnosis in most cases
- Doppler ultrasound is indicated only if the lesion is painful, warm, or spontaneously bleeds (to rule out fast-flow AVM)
- MRI/MRA when SWS or intracranial involvement is suspected
- Ophthalmologic evaluation starting in infancy for lesions involving V1 territory (glaucoma screening)
(Fitzpatrick's Dermatology, p. 2671)
Treatment
First-Line: Pulsed-Dye Laser (PDL)
- Wavelength: 585 nm or 595 nm; short pulse duration (400-1500 ms)
- Gold standard - targets oxyhemoglobin selectively (selective photothermolysis)
- 6-12 sessions typically required; general anesthesia may be needed in children
- Dynamic cooling device used to protect epidermis and allow higher fluence
- More effective on face/cervical/trunk lesions than extremities
- Does not improve associated soft tissue hypertrophy
- Recurrence can occur after stopping treatment
A recent systematic review and network meta-analysis (Nguyen et al., 2025) confirmed PDL at 595 nm remains the best-evidence treatment for port-wine birthmarks.
Other Modalities
- Topical rapamycin (sirolimus) - alone or as adjuvant to laser, shows promise
- Topical imiquimod - adjuvant role
- Contour resection / soft tissue debulking - for hypertrophy complications (lip, gum overgrowth)
- Camouflage makeup - highly effective noninvasive option for cosmetic management
- Orthopedic - shoe lifts for leg-length discrepancy >1.5 cm; epiphysiodesis at ages 11-13
For SWS specifically
- Prompt ophthalmologic follow-up from birth (glaucoma management)
- Prophylactic antiepileptic therapy - advocated but lacking robust RCT evidence
- Neuroimaging for leptomeningeal involvement
(Fitzpatrick's Dermatology, p. 2673-2674; Kanski's Clinical Ophthalmology, p. 63-64)
Key Points Summary
- Nevus flammeus = capillary malformation (CM) = port-wine stain - a congenital, slow-flow vascular malformation
- Caused by somatic GNAQ mutation; presents at birth, never involutes
- Darkens with age; soft tissue hypertrophy develops over decades
- 50% facial (trigeminal distribution); always assess for Sturge-Weber syndrome when V1 is involved
- Histology: dilated capillaries in upper dermis, S100-negative innervation, D2-40 negative
- Gold-standard treatment: pulsed-dye laser (595 nm) - multiple sessions required
- Distinguished from "nevus flammeus neonatorum" (salmon patch) which is transient and benign
Sources: Fitzpatrick's Dermatology (Vol. 1-2), Kanski's Clinical Ophthalmology (10th ed.), Andrews' Diseases of the Skin; supplemented by Nguyen et al. 2025 network meta-analysis and Hashemi et al. 2025 systematic review on laser treatment.
This is a shared conversation. Sign in to Orris to start your own chat.