Mild hydronephrosis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hydronephrosis"[MeSH Terms] AND "management"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have comprehensive information to provide a thorough answer on mild hydronephrosis.
Mild Hydronephrosis
Definition & Grading
Hydronephrosis is dilation of the renal pelvis and calyces, with or without accompanying parenchymal atrophy, caused by obstruction or reversal of urine outflow. It is graded qualitatively as mild, moderate, or severe:
| Grade | Ultrasound Findings |
|---|---|
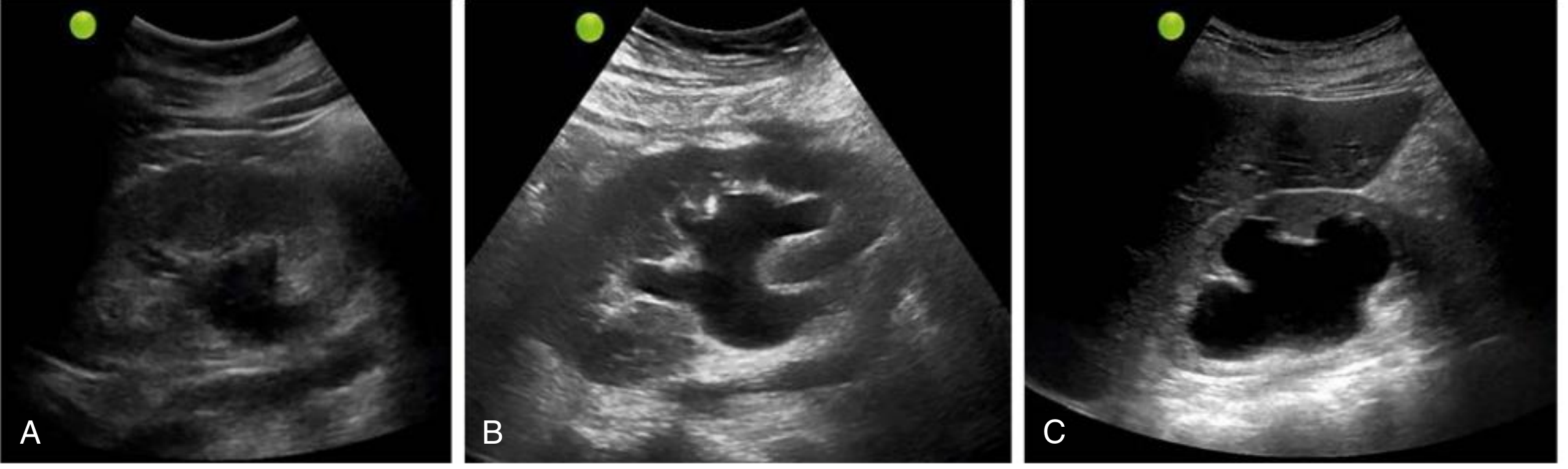
| Mild (Grade I) | Dilation of renal pelvis ± calyces; slight separation of central renal sinus fat; calyces not distorted; cortical thickness normal |
| Moderate (Grade II) | Greater pelvicalyceal distension; calyceal contours rounded; cortical thickness unaltered |
| Severe (Grade III–IV) | Marked calyceal ballooning; cortical thinning present; corticomedullary differentiation lost in extreme cases |
Fig. 5.6 — Mild (A), moderate (B), and severe (C) hydronephrosis on renal ultrasound:
Causes
Obstruction can occur at any level from urethra to renal pelvis. Causes are classified as:
Congenital
- Urethral atresia or valves
- Ureteropelvic junction (UPJ) obstruction (most common site in fetal hydronephrosis)
- Aberrant renal artery compressing the ureter
- Vesicoureteral reflux (VUR)
Acquired
- Foreign bodies/calculi — nephrolithiasis (most common in adults)
- Proliferative — benign prostatic hyperplasia, prostate/bladder/cervical carcinoma, retroperitoneal lymphoma
- Inflammatory — prostatitis, urethritis, retroperitoneal fibrosis
- Neurogenic — paralytic bladder (spinal cord injury)
- Physiological — pregnancy (mild hydronephrosis is normal, especially right-sided)
Bilateral hydronephrosis occurs only when obstruction is below the ureteral orifices (e.g., BPH, posterior urethral valves). Unilateral disease implies obstruction at or above the ureter.
Pathophysiology
Even with complete obstruction, glomerular filtration continues briefly. The filtrate backflows into the renal interstitium and returns via lymphatics/veins. The rising intrapelvic pressure is transmitted through the collecting ducts, compressing renal vasculature → arterial insufficiency + venous stasis. The papillae are most vulnerable (highest pressure), so the earliest functional defect is impaired tubular concentrating ability, with glomerular filtration declining later. Prolonged obstruction triggers interstitial inflammation → interstitial fibrosis.
Clinical Significance of Mild Hydronephrosis
- Long-term morbidity is low when mild (pelvicaliectasis without parenchymal thinning) — Brenner & Rector's Kidney
- Mild hydronephrosis in pregnancy is physiological (progesterone-mediated ureteral relaxation + uterine compression, predominantly right side)
- In fetal/neonatal context: mild antenatal hydronephrosis carries a prevalence of vesicoureteral reflux of ~15% on postnatal ultrasound — Campbell-Walsh Urology
- The degree of hydronephrosis does not always correlate with the degree of obstruction
Diagnosis
Ultrasound is the primary modality (>95% accuracy for detecting hydronephrosis). Key points:
- Hydronephrosis appears as anechoic branching/interconnected areas in the collecting system
- Always scan the bladder to assess retention and to guide level of obstruction
- False negatives occur with acute/partial obstruction, volume depletion, or retroperitoneal fibrosis
- Use color Doppler to distinguish from renal vasculature (flow) or parapelvic cysts (round, non-branching, no connection to ureter)
- Pseudohydronephrosis (overdistended bladder) can mimic mild hydronephrosis — have the patient void first
If ultrasound cannot determine the cause: non-contrast CT is the next step (excellent for calculi and obstruction level). MAG3 furosemide renography evaluates differential renal function and drainage kinetics.
Management Principles
Management is directed at the underlying cause and severity:
| Scenario | Approach |
|---|---|
| Mild, incidental, no functional impairment | Watchful waiting + repeat imaging |
| Calculus-related | Analgesia, hydration; urologic intervention if no spontaneous passage |
| BPH causing outlet obstruction | Bladder catheter (diagnostic + therapeutic), α-blockers, surgical referral |
| Fetal/neonatal hydronephrosis | Postnatal US in first week; if confirmed → urine culture, BMP (if bilateral), VCUG; if VCUG normal → furosemide renography |
| Urosepsis/azotemia + hydronephrosis | IV antibiotics + urgent drainage (nephrostomy or ureteral stenting) |
| Transplant kidney + rising creatinine | Low threshold for stenting; if rejection suspected simultaneously → biopsy first |
Key Pitfalls
- Mild hydronephrosis on US does not exclude significant obstruction — functional imaging (renography) may be needed
- Acute/complete obstruction may show only mild dilation because filtration ceases early before significant distension develops
- Always consider pyonephrosis if hydronephrosis is accompanied by fever, flank pain, or internal echoes on US → urgent drainage required
Sources: Comprehensive Clinical Nephrology 7e | Robbins & Kumar Basic Pathology | Brenner & Rector's The Kidney | Campbell-Walsh Urology | Textbook of Family Medicine 9e
This is a shared conversation. Sign in to Orris to start your own chat.