Explain syndromes of kidney injury
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information from authoritative textbooks to write a detailed, well-organized answer. Let me compile everything.
Syndromes of Kidney Injury
Kidney injury presents through a limited set of clinical syndromes, each with a distinct constellation of findings that points toward specific anatomical sites and pathological mechanisms. The major syndromes are: Acute Kidney Injury (AKI), Nephrotic Syndrome, Nephritic Syndrome, Rapidly Progressive Glomerulonephritis (RPGN), Asymptomatic Urinary Abnormalities, and Chronic Kidney Disease (CKD). Understanding these syndromes is the foundation of nephrology diagnosis.
1. Acute Kidney Injury (AKI)
AKI is a broad clinical syndrome defined by an abrupt decrease in kidney function over hours to days, characterized by a rise in serum creatinine or a fall in urine output. The three major pathophysiologic categories provide a clinical framework:
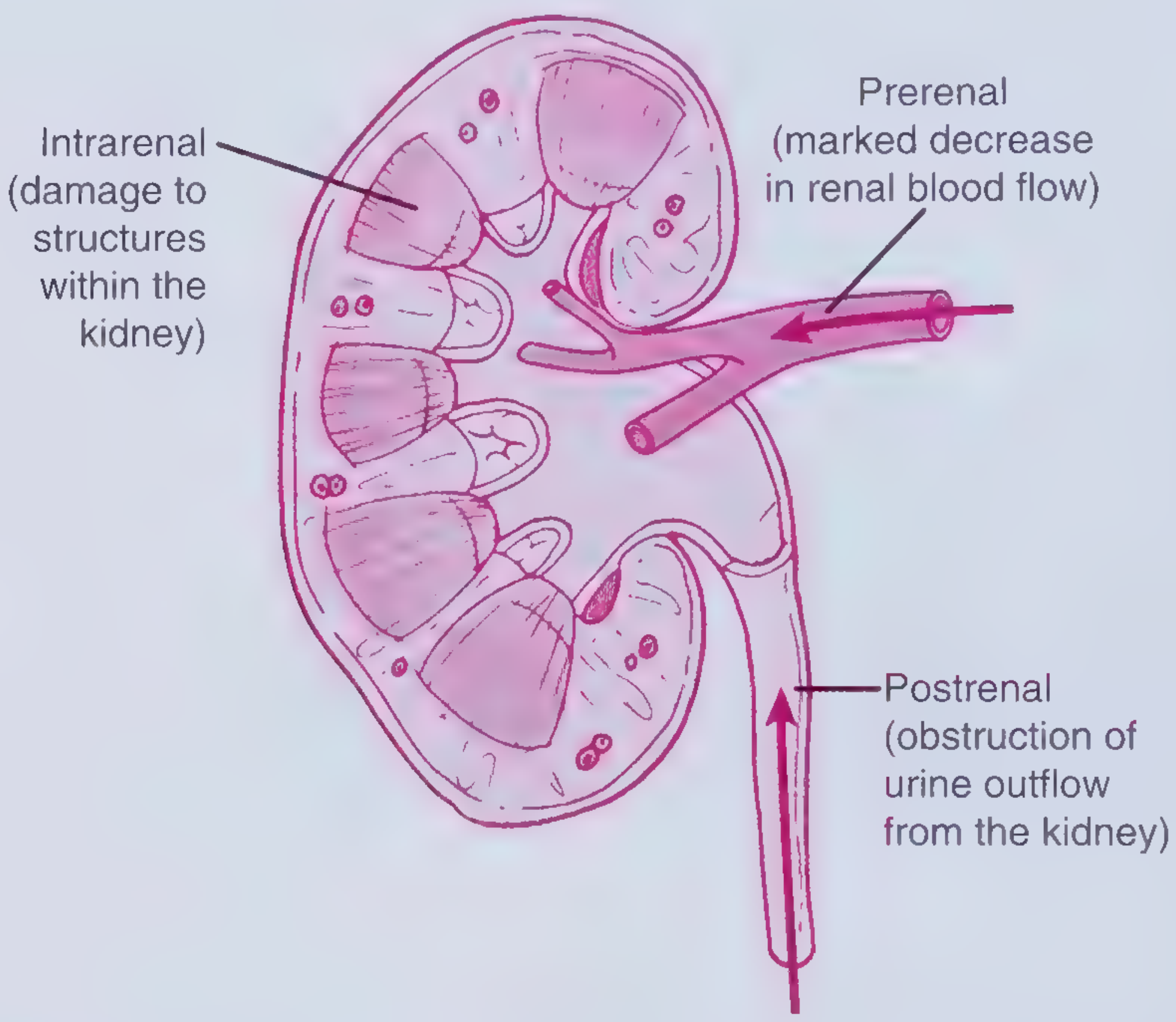
Prerenal AKI
- The most common cause, accounting for 40-55% of all AKI cases
- Results from kidney hypoperfusion due to reduced actual or effective arterial blood volume (EABV)
- Common causes: hemorrhage, GI losses (vomiting, diarrhea), overdiuresis, cardiogenic shock, septic shock, cirrhosis, hypoalbuminemia, third spacing (e.g., pancreatitis)
- Mechanism: Volume depletion activates the RAAS. Angiotensin II preferentially increases efferent arteriolar resistance to maintain GFR, but when severe, leads to afferent arteriolar constriction, reducing renal plasma flow and GFR. Sympathetic activation and ADH release augment sodium and water retention
- Key feature: Rapidly reversible if renal perfusion is restored, because parenchymal integrity is intact. Prolonged hypoperfusion leads to ischemic acute tubular necrosis (ATN), making prerenal AKI and ischemic ATN a pathophysiological spectrum
- There are volume-responsive and volume-nonresponsive forms; the latter occurs in CHF, liver failure, and sepsis where restoring volume does not improve kidney perfusion
Intrinsic (Intrarenal) AKI
Damage to structures within the kidney itself. Subdivided by anatomical compartment:
- Tubular - ATN (ischemia, nephrotoxins: aminoglycosides, contrast, myoglobin)
- Glomerular - glomerulonephritis
- Interstitial - acute allergic interstitial nephritis (drugs, diuretics)
- Vascular - HUS, TTP, renal artery/vein thrombosis
Postrenal AKI
- Obstruction of urine outflow from the kidney
- Causes: BPH, stones, tumors, strictures, bilateral ureteral obstruction
- Promptly reversible upon relief of obstruction
Source: Brenner and Rector's The Kidney, AKI Pathophysiology chapter; Tietz Textbook of Laboratory Medicine, 7th ed.
2. Nephrotic Syndrome
Definition: Heavy proteinuria (≥3.5 g/day in adults), hypoalbuminemia (albumin <3 g/dL), generalized edema, hyperlipidemia, and lipiduria. Minimal or absent hematuria.
Pathophysiology: Glomerular injury disrupts the filtration barrier (podocyte foot processes and slit diaphragm), allowing massive protein loss into urine. The hallmark histological finding is fusion of epithelial foot processes on electron microscopy, seen in all cases regardless of cause. Loss of albumin causes oncotic pressure to fall, promoting fluid transudation and edema; the liver compensates by overproducing lipoproteins, causing hyperlipidemia.
Clinical features:
- Insidious onset, massive edema (periorbital, ankle, anasarca)
- Normal blood pressure (early), normal/low JVP
- Proteinuria ++++, hematuria absent or mild
- Serum albumin low
- Hypercoagulable state (loss of antithrombin III, protein C/S)
Major causes:
| Primary | Secondary |
|---|---|
| Minimal Change Disease (MCD) - 70-90% of childhood NS | Diabetic nephropathy |
| Focal Segmental Glomerulosclerosis (FSGS) | SLE (membranous lupus) |
| Membranous nephropathy | Amyloidosis |
| MPGN | Hepatitis B/C |
Complications:
- AKI (via volume depletion, renal vein thrombosis, sepsis, NSAIDs, ACE inhibitors, interstitial nephritis from diuretics)
- Thromboembolism (renal vein thrombosis, DVT, PE)
- Infection (loss of immunoglobulins)
- Progressive kidney failure - risk is directly proportional to degree of proteinuria; sustained proteinuria >5 g/day carries the highest risk
Treatment: Cause-specific immunosuppression (steroids for MCD), loop diuretics, ACE inhibitors/ARBs, SGLT2 inhibitors (to reduce proteinuria), statins, anticoagulation.
Source: Comprehensive Clinical Nephrology, 7th ed.; Harrison's Principles of Internal Medicine, 22nd ed.; Robbins, Cotran & Kumar Pathologic Basis of Disease
3. Nephritic Syndrome
Definition: Glomerular inflammation causing hematuria with RBC casts, non-nephrotic proteinuria, oliguria, hypertension, and reduced GFR. Edema is present but less severe than in nephrotic syndrome.
Pathophysiology: Immune-mediated injury (immune complex deposition, anti-GBM antibodies, ANCA-mediated) activates complement and Fc receptors, causing leukocyte infiltration into glomeruli, endocapillary hypercellularity, and barrier disruption. Subendothelial immune deposits cause more inflammation (due to easier access of complement from blood), unlike subepithelial deposits which cause proteinuria with less inflammation.
Comparison with nephrotic syndrome:
| Feature | Nephrotic | Nephritic |
|---|---|---|
| Onset | Insidious | Abrupt |
| Edema | ++++ | ++ |
| Blood pressure | Normal | Raised |
| JVP | Normal/low | Raised |
| Proteinuria | ++++ | ++ |
| Hematuria | Absent/mild | +++ |
| RBC casts | Absent | Present |
| Serum albumin | Low | Normal/slightly reduced |
Classic presentation: Poststreptococcal GN in children - rapid onset of oliguria, weight gain, generalized edema, brown (cola-colored) urine with RBC casts, hypertension, and pulmonary edema without primary cardiac disease.
Common causes (with key serologic tests):
- Poststreptococcal GN: elevated ASO titer
- IgA nephropathy: elevated serum IgA, concurrent with respiratory/GI infections
- Lupus nephritis: ANA, anti-dsDNA, low C3/C4
- Endocarditis: positive blood cultures, low C3
Source: Comprehensive Clinical Nephrology, 7th ed.; Robbins, Cotran & Kumar Pathologic Basis of Disease
4. Rapidly Progressive Glomerulonephritis (RPGN)
RPGN represents the most severe end of the nephritic spectrum. Glomerular injury is so acute and severe that kidney function deteriorates markedly over days to weeks, potentially producing a uremic emergency.
Histologic hallmark: Crescentic GN - a proliferative cellular response (parietal epithelial cells, fibrin, monocytes) occupying Bowman's space outside the glomerular tuft. Crescents are so named for their shape on cross-section. Adjacent glomerular segments typically show fibrinoid necrosis or segmental necrotizing GN (especially in vasculitis syndromes).
Classification (3 immunologic types):
| Type | Mechanism | Example | Key Test |
|---|---|---|---|
| I (Linear IgG) | Anti-GBM antibodies | Goodpasture syndrome | Anti-GBM antibody (NC1 domain of α3 chain of type IV collagen) |
| II (Granular) | Immune complex | Postinfectious GN, lupus, IgA nephropathy, MPGN | Complement levels, ANA, anti-dsDNA, ASO |
| III (Pauci-immune) | ANCA-mediated | Granulomatosis with polyangiitis, microscopic polyangiitis | ANCA (PR3-ANCA or MPO-ANCA) |
Key caveat: Not all patients with nephritic urinary sediment and AKI have RPGN - AKI in milder GN can also be caused by accelerated hypertension, renal vein thrombosis, or superimposed ATN. Histologic confirmation is essential.
Source: Comprehensive Clinical Nephrology, 7th ed.; Brenner and Rector's The Kidney; Goldman-Cecil Medicine
5. Asymptomatic Urinary Abnormalities
Some glomerular diseases cause isolated proteinuria or isolated hematuria with no other signs or symptoms. These patients are often identified incidentally on routine urinalysis.
- Isolated hematuria: Microscopic blood in urine without proteinuria or renal impairment. Common causes include IgA nephropathy (recurrent macroscopic hematuria with concurrent infections) and thin basement membrane nephropathy (TBMN) - the latter has uniformly thinned GBM on biopsy, normal kidney function, and no/minimal proteinuria
- Isolated proteinuria: Sub-nephrotic range protein without hematuria or functional impairment; requires workup to exclude orthostatic proteinuria, early glomerular disease, or tubulointerstitial disease
- More severe disease develops if these abnormalities progress, and they serve as early markers of evolving glomerular pathology
Source: Brenner and Rector's The Kidney; Tietz Textbook of Laboratory Medicine, 7th ed.
6. Chronic Kidney Disease (CKD) / Chronic Glomerulonephritis
Most forms of chronic GN lead to slowly progressive kidney failure. Between 25-50% of patients with glomerular disease show progressive renal impairment over years. Patients present late with:
- Established hypertension
- Proteinuria
- Reduced GFR
- Small, smooth, symmetric kidneys on imaging (bilateral renal atrophy)
At advanced stages, biopsy shows non-specific ESKD changes: focal or global glomerulosclerosis, dense tubulointerstitial fibrosis, and tubular atrophy. The original glomerular disease pattern may no longer be identifiable by light microscopy; immunofluorescence (e.g., mesangial IgA in IgA nephropathy) may help.
Proteinuria as a major prognostic factor: Progression is uncommon with sustained proteinuria <2 g/day; the risk rises sharply with excretion >5 g/day. Proteinuria itself may be directly nephrotoxic to the tubulointerstitium.
Uremic syndrome develops at end-stage CKD, involving multi-organ dysfunction: pericarditis, encephalopathy, peripheral neuropathy, bleeding (platelet dysfunction), anemia (reduced EPO production), mineral-bone disorder, and metabolic acidosis.
Summary Table
| Syndrome | Key Feature | Urine | GFR | Blood Pressure | Onset |
|---|---|---|---|---|---|
| Prerenal AKI | Hypovolemia | Low Na, high SG | ↓ acutely | Low/normal | Hours |
| Intrinsic AKI (ATN) | Tubular casts | Muddy brown casts | ↓↓ acutely | Variable | Hours-days |
| Nephrotic | Massive proteinuria | Proteinuria ++++, lipiduria | Normal (early) | Normal | Insidious |
| Nephritic | Hematuria + RBC casts | Hematuria, proteinuria ++ | ↓ | Raised | Abrupt |
| RPGN | Crescentic GN | As in nephritic | ↓↓↓ rapidly | Raised | Days-weeks |
| CKD | Small shrunken kidneys | Proteinuria ± hematuria | ↓ chronically | Raised | Months-years |
The classification of kidney injury into these syndromes is imperfect - patients with membranoproliferative GN, for instance, may present with nephrotic syndrome, nephritic syndrome, or a combination of both. Clinical description at first presentation helps narrow the differential diagnosis, but histologic confirmation (kidney biopsy) remains the definitive tool in most cases.
- Comprehensive Clinical Nephrology, 7th Edition
- Brenner and Rector's The Kidney, 2-Volume Set
- Harrison's Principles of Internal Medicine, 22nd ed.
- Robbins, Cotran & Kumar Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.