Role of ABPI and USG in lower limb vascular diseases
Reading File
Finding Sources
Finding Sources
Searching PubMed
ankle brachial index peripheral arterial disease diagnosis
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Now I have all the content needed for a comprehensive answer. Here is the full, well-structured response:
ABPI and USG in Lower Limb Vascular Diseases
ANKLE-BRACHIAL PRESSURE INDEX (ABPI / ABI)
Definition and Principle
The ABPI (also called ABI) is the ratio of the highest systolic blood pressure at the ankle to the highest systolic blood pressure in either brachial artery. It is the most widely used non-invasive bedside test to detect and grade lower limb peripheral arterial disease (PAD).
ABPI = Ankle systolic pressure (posterior tibial or dorsalis pedis) / Higher brachial systolic pressure
Example: Ankle pressure 92 mmHg ÷ Arm pressure 164 mmHg = ABI of 0.56 (moderate obstruction)
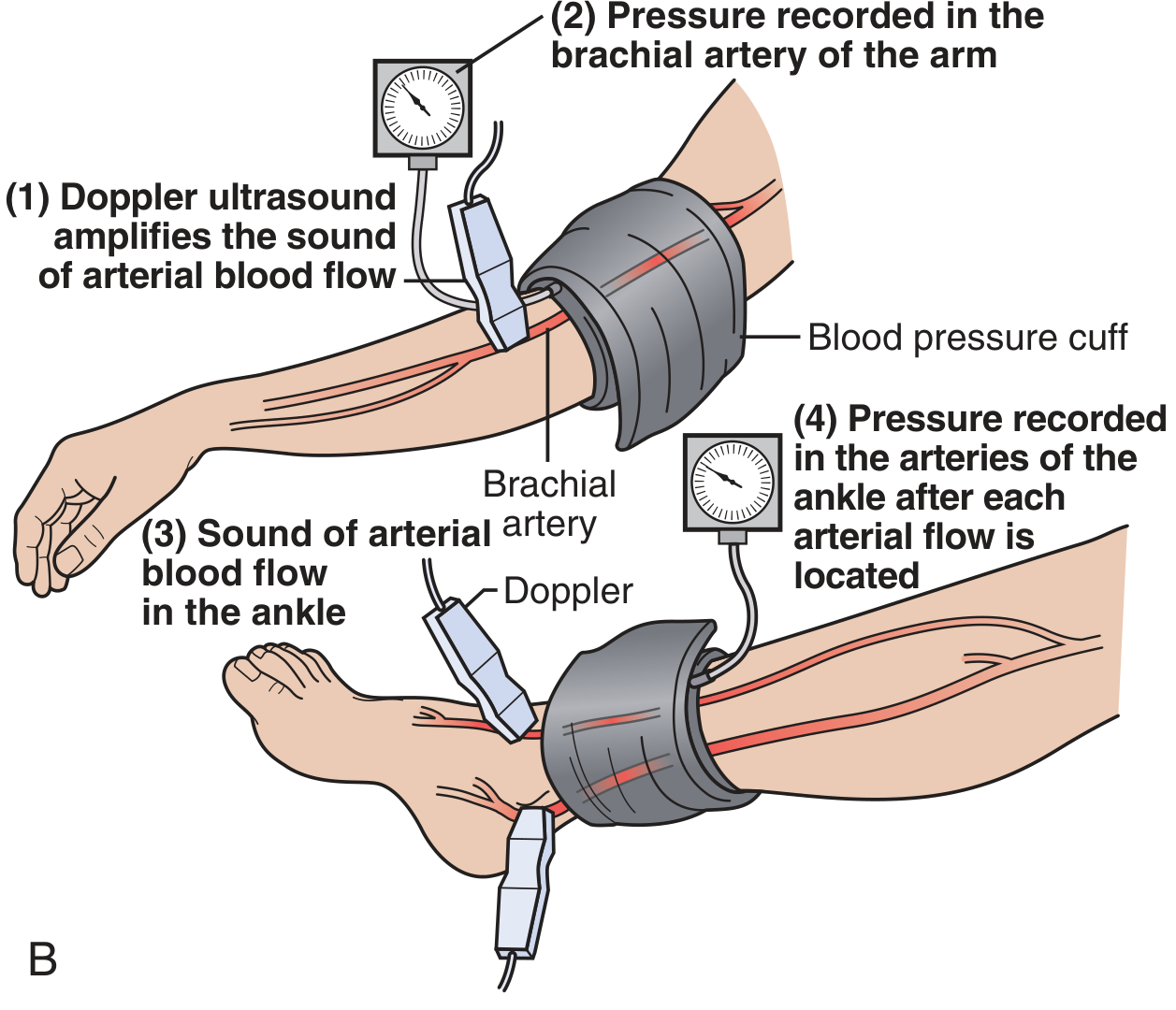
Technique / How to Measure
- The patient lies supine and rests for at least 5-10 minutes.
- A Doppler probe (5-10 MHz for limb vessels) is used with acoustic coupling gel angled at 45° along the vessel axis.
- A sphygmomanometer cuff is placed just above the malleolus. The cuff is inflated until flow disappears, then slowly deflated - the pressure at which flow returns is the ankle systolic pressure.
- This is recorded for both the posterior tibial and dorsalis pedis arteries in each leg.
- The brachial pressure is measured in both arms; the higher reading is used as the denominator.
- The higher of the ankle pressures (PT or DP) is used as the numerator.
Interpretation (PARTNERS Program Classification)
| ABPI Value | Interpretation |
|---|---|
| > 1.3 | Non-compressible/calcified vessels (falsely elevated - seen in diabetes, CKD) |
| 0.91 - 1.30 | Normal |
| 0.71 - 0.90 | Mild obstruction |
| 0.41 - 0.70 | Moderate obstruction (intermittent claudication typical) |
| 0.00 - 0.40 | Severe obstruction (rest pain, critical limb ischemia) |
| < 0.9 | Diagnostic of PAD (sensitivity and specificity >95%) |
| < 0.4 | Critical limb ischemia |
- A ratio <0.90 is abnormal and indicates need for further investigation.
- A ratio of 0.90-0.99 warrants close observation and repeated measurements.
- A completely normal ABPI (≥ 1.0) with normal examination allows safe discharge without vascular intervention in trauma patients.
Clinical Applications of ABPI
1. Diagnosis of Peripheral Arterial Disease (PAD)
- Defines the presence of PAD (ABI < 0.90) in any patient with symptoms of claudication, rest pain, or non-healing ulcers.
- Confirms PAD in patients with atypical leg pain; differentiates vascular from neurogenic claudication.
- Screens high-risk populations: age ≥65, age 50-64 with diabetes/smoking, known atherosclerosis elsewhere.
2. Grading Severity (Fontaine Classification context)
- Grade I/II (claudication): ABPI typically 0.5-0.8
- Grade III/IV (rest pain, gangrene/ulcer): ABPI typically <0.5
3. Wound Healing and Compression Therapy Guidance
- In venous leg ulcers with concurrent arterial disease, an ABPI of 0.5-0.8 allows modified compression (interface pressure ~30 mmHg is safe and effective; pressures up to 40 mmHg have been used).
- Full compression (40 mmHg four-layer bandaging) is safe only when ABPI ≥ 0.8.
- An ABPI ≥ 0.5 at the surgical level supports successful wound healing after amputation.
4. Trauma Screening (Arterial Pressure Index / API)
- In extremity trauma, comparing injured vs. uninjured limb systolic pressures (API) or ankle-to-brachial ratio screens for arterial injury with sensitivity and specificity >95%.
- API/ABI <0.90 = arterial injury until proven otherwise; proceed to further imaging (CTA/angiography).
- API/ABI 0.90-0.99 = observe for 12-24 hours with repeated measurements.
- API/ABI ≥1.0 with normal exam = safe discharge.
5. Cardiovascular Risk Stratification
- An ABI <0.9 is an independent marker of systemic atherosclerosis. Patients with PAD have a several-fold increased risk of MI, stroke, and death - over one third have significant coronary artery disease.
- ABI is used to guide intensity of medical therapy (antiplatelets, statins, ACE inhibitors).
6. Post-revascularization Monitoring
- Serial ABPI measurements track the success or failure of bypass surgery and endovascular procedures.
- Falling ABPI after revascularization indicates restenosis or graft occlusion.
Limitations of ABPI
- Non-compressible vessels (ABPI >1.3): medial calcification in diabetics, elderly, and CKD patients gives falsely high values - use toe-brachial index (TBI) instead.
- Cannot be used when both limbs are injured or in severe soft tissue disruption.
- Certain arteries (profunda femoris, profunda brachii, peroneal) do not produce measurable distal pressures.
- Shotgun wounds - normal ABPI despite multiple small arterial wounds; angiography preferred.
- Detects macrovascular disease but may miss microvascular disease (relevant in diabetic foot).
SEGMENTAL LIMB PRESSURES (Doppler)
Beyond a simple ABPI, segmental pressures measured at the upper thigh, lower thigh, upper calf, and ankle can localize the level of arterial occlusion:
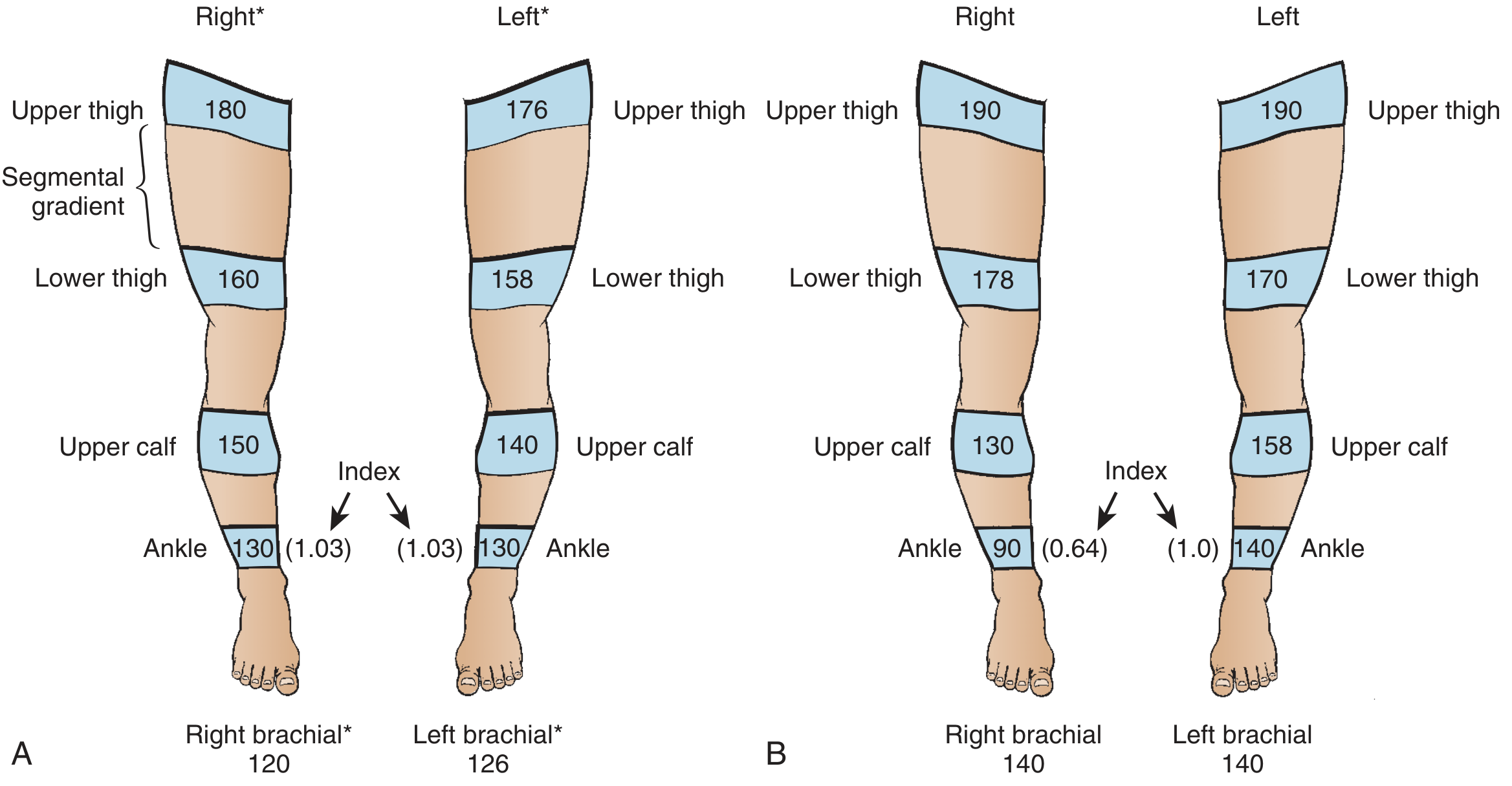
- Normal findings: ABPI ≥ 1.0; all segmental gradients <30 mmHg; upper thigh ≥ 40 mmHg above brachial.
- Gradient >30 mmHg between adjacent segments = significant occlusion at that level.
- Upper thigh pressure low: suggests aorto-iliac disease.
- Large thigh-to-calf gradient: superficial femoral artery (SFA) disease.
- Ankle-to-calf gradient: popliteal or tibial artery disease.
ULTRASOUND (USG) IN LOWER LIMB VASCULAR DISEASES
USG in lower limb vascular assessment encompasses three main modalities:
| Modality | What it provides |
|---|---|
| B-mode (2D) | Vessel anatomy, wall thickness, plaque, thrombus |
| Doppler (CW/PW) | Flow direction, velocity, waveform character |
| Duplex (B-mode + Doppler) | Combined structural + hemodynamic assessment |
| Color Doppler | Displays flow direction and velocity as color map |
A. Doppler USG Principles
- Venous flow: low-pitched hum; phasic with respiration.
- Normal arterial flow: triphasic - sharp systolic forward peak, brief early diastolic reversal, then a small forward diastolic component. Reflects high peripheral resistance.
- Damped (biphasic or monophasic) arterial waveform: indicates proximal stenosis or obstruction ("damped" by partial occlusion).
- Probes of 5-10 MHz are appropriate for limb vessels; probe angled at 45° to vessel axis for optimal frequency shifts.
B. Duplex USG in Peripheral Arterial Disease
Indications:
- Confirm location and severity of arterial stenosis or occlusion
- Pre-operative planning for revascularization
- Post-procedural surveillance of bypass grafts and stents
- Popliteal aneurysm detection
Key diagnostic findings:
- Focal increase in peak systolic velocity (PSV): indicates partial obstruction. A PSV ratio >2.0 at the stenosis vs. proximal segment = >50% stenosis.
- Loss of triphasic waveform downstream of a significant stenosis.
- Absent flow: complete occlusion.
- Echogenic material within vessel lumen: thrombus.
Limitations for arterial disease:
- Technically difficult in: deep vessels (aorta, iliac), profunda femoris, profunda brachii, subclavian and iliac vessels (acoustic windows inadequate).
- May miss lesions that don't significantly alter flow: small pseudoaneurysms, arterio-venous fistulae (AVF), intimal flaps.
- Fresh thrombus is relatively non-echogenic, making it difficult to identify on B-mode alone.
- In aortic occlusive disease (Leriche syndrome), duplex plays very little role because the aorta is often difficult to visualize - MRA or CTA preferred.
C. Duplex USG in Venous Disease (Varicose Veins / Chronic Venous Insufficiency)
This is the gold standard investigation for varicose veins. Hand-held Doppler and tourniquet tests have been abandoned in favor of duplex scanning before any intervention.
Transducer: High-frequency linear array probe, 7.5-13 MHz, appropriate for most lower limb assessments.
Color convention: Blue = antegrade flow (toward heart); Red = retrograde/reflux flow. Venous flow can be augmented by calf squeeze.
What duplex establishes in varicose veins:
- Presence of reflux in the deep and superficial venous systems.
- Exact distribution and extent of reflux - including affected junctions (SFJ, SPJ) and perforators.
- Presence of obstruction in the deep venous system.
- Suitability of incompetent superficial veins for treatment (diameter, extent, tortuosity, saphena varix).
- Presence of thrombus within superficial veins (superficial thrombophlebitis).
- Evidence of a pelvic source of reflux or obstruction.
Anatomical mapping helps guide treatment:
- Medial thigh and calf varicosities → great saphenous vein (GSV) incompetence.
- Posterolateral calf varicosities → short saphenous vein (SSV) incompetence.
- Anterolateral thigh and calf → isolated accessory GSV incompetence.
Clinical significance of reflux duration:
- Reflux >0.5 seconds on Doppler (augmentation release) = significant venous reflux.
- Best clinical results come from clinicians personally skilled in duplex who design bespoke treatment for each patient based on their unique anatomy.
D. Duplex USG in Deep Vein Thrombosis (DVT)
- Compression ultrasound: non-compressibility of the vein on probe pressure = thrombus. This is the primary diagnostic test for DVT.
- Loss of respiratory phasicity of flow on Doppler suggests proximal obstruction.
- Duplex helps differentiate acute DVT (hypoechoic, soft clot) from chronic (echogenic, calcified, recanalized) thrombus.
- Shows extension of superficial thrombophlebitis into the deep system, and detects concomitant DVT.
E. USG in Acute Limb Ischemia
- B-mode can identify loss of arterial pulsation in major vessels.
- Doppler detects absent or markedly diminished flow, and change from triphasic to monophasic waveform.
- A vascular ultrasound may reveal thrombosis of a popliteal aneurysm presenting as acute limb ischemia.
- Limitation: cannot visualize certain areas (subclavian, iliac); unreliable for fresh thrombus or intimal flaps - CTA or catheter angiography preferred for definitive planning.
Summary Comparison Table
| Feature | ABPI | Duplex USG |
|---|---|---|
| What it measures | Hemodynamic severity (pressure gradient) | Anatomical + hemodynamic |
| Arterial PAD screening | First-line, simple, bedside | Second-line, pre-operative planning |
| Venous disease | Not applicable (except compression guidance) | Gold standard |
| DVT | Not applicable | Primary diagnostic test |
| Aorto-iliac disease | Reduced ABPI + low thigh pressure | Limited (poor acoustic window) - use MRA/CTA |
| Calcified vessels (diabetics) | Falsely elevated (>1.3) | Not affected |
| Post-revascularization | Serial ABPI monitoring | Graft/stent surveillance |
| Limitations | Calcification, bilateral injury | Operator dependent, limited acoustic windows |
Key References
- Goldman-Cecil Medicine (International Edition) - Peripheral Arterial Disease chapter
- Bailey and Love's Short Practice of Surgery (28th Ed) - Varicose Veins & Arterial Disease
- Tintinalli's Emergency Medicine (Comprehensive Study) - Acute vs. Chronic Arterial Disease
- Roberts and Hedges' Clinical Procedures in Emergency Medicine - Doppler ABI Technique
- Rosen's Emergency Medicine - Arterial Pressure Index and ABI
- Grainger & Allison's Diagnostic Radiology - Chronic Aortic Occlusive Disease
Recent evidence update: A 2024 Cochrane systematic review (PMID: 39474992) assessed the toe-brachial index and toe systolic blood pressure as alternatives for PAD diagnosis - relevant when ABPI is unreliable due to vessel calcification (diabetic and CKD patients), where TBI <0.70 is now preferred for diagnosis.
This is a shared conversation. Sign in to Orris to start your own chat.