Fall in elderly
"falls"[MeSH Terms] AND "aged"[MeSH Terms] AND "prevention"[MeSH Terms]
"accidental falls"[MeSH Terms] AND "aged"[MeSH Terms]
Falls in the Elderly
Epidemiology
- ~30% of community-dwelling people over 65 years fall at least once per year
- Rises to 40% in those over 80 years
- Exceeds 50% in nursing home residents
- Annual incidence in long-term care: ~1,600 falls per 1,000 beds
- 55% of those who fall once will fall again
- 10-15% of falls result in fractures or serious injuries
- Falls cause approximately 9,500 deaths annually in the United States
- Only 50% of elderly who fall are able to get up unaided - the "long lie" is associated with lasting functional decline
Pathophysiology - Why the Elderly Fall
Age-Related Physiologic Changes
- Postural reflex impairment - A study found moderate/severe postural reflex impairment in two-thirds of neurologically intact elderly patients
- Reduced reaction time - Failure to make rapid postural adjustments during usual activities (walking, changing position, descending stairs)
- Impaired visual function - Decreased visual acuity and contrast sensitivity
- Vestibular dysfunction - Age-related decline in vestibular function and proprioception
- Muscle weakness - Especially lower extremity weakness (sarcopenia)
- Decreased hearing - Impairs spatial orientation
- Cervical degenerative disease - Impairs proprioception
Causes of Falls - Classification
1. Associated with Syncope / Loss of Consciousness
- Dysrhythmias
- Seizures
- Acute coronary syndrome
- Hypoglycemia
- Pulmonary embolism
2. Near-Syncope / Positional / Vasodilatory
- Orthostatic hypotension (most common cause) - especially from antihypertensives (beta-blockers, calcium channel blockers, ACE inhibitors)
- Dehydration / diuretics
- GI bleed or abdominal aortic aneurysm
- Sepsis / anemia
- Postprandial hypotension (30-60 minutes after eating)
3. Nonsyncopal "Mechanical" Causes
- Deconditioning
- Decreased visual acuity
- Unsafe home environment (poor lighting, loose rugs, wet floors)
- Alcohol use
- Sedating medications - benzodiazepines, narcotics, antihistamines, sleep aids, tricyclic antidepressants (especially amitriptyline - both anticholinergic and alpha-blocking effects)
- Neurologic disease: stroke, Parkinson disease, normal-pressure hydrocephalus, progressive supranuclear palsy, dementia (Alzheimer's)
- Urinary urgency (rushing to bathroom)
- Peripheral edema (impairs foot clearance)
High-Risk Medications (Beers Criteria)
| Drug Class | Mechanism |
|---|---|
| Benzodiazepines | Sedation, impaired balance |
| Tricyclics (amitriptyline) | Anticholinergic + alpha-blockade (orthostasis) |
| Antihypertensives (ACE-i, CCB, diuretics) | Orthostatic hypotension |
| Antipsychotics | Sedation, extrapyramidal effects |
| Anticholinergics | Confusion, sedation |
Risk Factors
- Advanced age
- Past history of falls (strongest predictor)
- Cognitive impairment / dementia
- Female gender
- Lower extremity weakness
- Gait or balance problems
- Foot disorders
- Poor vision
- Psychotropic medication use
- Arthritis
- Vitamin D deficiency
- Parkinson disease
- Osteoporosis (amplifies fracture risk)
Consequences / Complications
Fractures
- Hip fracture - the most feared complication
- 14% die within 6 months; ~25% within 1 year
- Most do not regain prior functional level
- 5x more likely to be institutionalized at 1 year
- Associated with depression, social isolation, chronic pain
- Shorter time to surgery reduces mortality and complications
- Pelvic fracture - >80% caused by falls; in-hospital mortality ~8%, up to 5x higher than younger patients; 27% die within 1 year
- Rib fractures - in-hospital mortality doubles in patients >65 years; >3 ribs = worse outcomes, higher rates of pneumonia and ICU stay
- Cervical spine fracture - 5-10% risk of permanent neurological deficit; 1-year mortality 20-30%
- Distal radius fracture ("Colles' fracture" - outstretched hand)
Other Complications
- Subdural hematoma - especially in anticoagulated patients
- Soft tissue injuries, lacerations
- "Long lie" - inability to get up leads to dehydration, hypothermia, rhabdomyolysis, pressure injuries, aspiration pneumonia
- Fear of falling (FOF) - leads to activity restriction, deconditioning, social withdrawal, further increasing fall risk (vicious cycle)
- Loss of independence / institutionalization
Assessment
Initial Screening (AGS/BGS Guidelines)
- Have you fallen in the past year?
- How often, and what were the circumstances?
- Do you have difficulty with walking or balance?
- Anyone who fell and sought medical attention
- Recurrent falls (2+ in past year)
- Single fall + gait/balance difficulty on assessment
Multifactorial Risk Assessment Includes:
- Detailed fall circumstances, frequency, symptoms, injuries
- Full medication review (all Rx and OTC)
- Relevant medical history (osteoporosis, urinary incontinence, cardiovascular disease)
- Gait and balance (Timed Up and Go test, Berg Balance Scale)
- Neurologic: cognitive function, peripheral nerves, proprioception, cerebellar and extrapyramidal function
- Muscle strength (lower extremities)
- Cardiovascular: heart rate, rhythm, orthostatic BP (lying, sitting, standing)
- Visual acuity
- Feet and footwear examination
- ADL performance and use of mobility aids
- Fear of falling scale
- Activity curtailment assessment
- Home safety evaluation (lighting, flooring, bathroom rails, stairs)
Emergency Management (ED Approach)
- Do not be falsely reassured by "normal" vital signs - beta-blockers mask tachycardia; use SBP <110 mmHg (not <90) as hypotension cutoff in elderly blunt trauma
- Up to 39% with SBP >90 and HR <120 may have occult hypoperfusion (check lactate/base deficit)
- Because hypertension affects ~90% of elderly, a "normal" BP may actually be relatively hypotensive for that patient
- Always investigate why the patient fell - could reveal cardiac arrhythmia, stroke, PE, GI bleed
Prevention - Multifactorial Intervention
1. Exercise Programs
- Strength and balance training (most evidence-based)
- Tai chi - proven effective in reducing falls
- Gait training with mobility aids
- Physical therapy referral
2. Medication Review
- Medication review every 3 months for every elder
- Minimize total number of medications
- Withdraw psychotropic drugs where possible
- Start new medications at low doses and titrate slowly ("start low, go slow")
- Avoid amitriptyline and other high-risk drugs in the elderly (Beers Criteria)
3. Environmental Modification
- Adequate lighting without glare
- Dry, non-slippery floors free of obstacles
- High, firm chairs and raised toilet seats
- Handrails in bathrooms and stairways
- Remove loose rugs and trip hazards
- Bed and call-bell within reach
4. Medical/Sensory Optimization
- Correct visual impairment (cataract surgery, new glasses)
- Treat orthostatic hypotension
- Manage cardiovascular disease; cardiac pacing for high-risk individuals with bradyarrhythmias
- Treat vitamin D deficiency (supplementation if levels are low - evidence for fall reduction strongest in deficient patients)
- Manage urinary incontinence / urgency
5. Osteoporosis Prevention (reduces fracture severity even if fall occurs)
- Calcium + Vitamin D supplementation in postmenopausal women
- Bisphosphonates, calcitonin, or estrogen therapy
- Fracture Liaison Service referral after fragility fracture
6. Education
- Patient and caregiver education about fall risk
- Teach how to get up safely from the floor
7. Restraints - Evidence Against
- No study has ever shown restraints reduce fall risk
- Restraints cause significant morbidity: strangulation, vascular injury, neurologic damage, anxiety, agitation
- Alternatives: wedge cushions for chair positioning, organized walking programs, supervised ambulation
Recent Evidence (PubMed 2023-2024)
- A 2024 JAMA systematic review for the USPSTF (PMID 38833257) evaluated interventions to prevent falls in older adults - exercise, vitamin D, and multifactorial interventions all showed benefit in community-dwelling elders
- A 2024 network meta-analysis in Systematic Reviews (PMID 39593159) of fall prevention interventions for community-dwelling older adults confirmed that exercise-based interventions and multifactorial programs reduce fall incidence
- A 2024 systematic review in Age and Ageing (PMID 39023234) analyzed hospital fall clinical practice guidelines globally, confirming multifactorial risk assessment and targeted interventions as standard of care
- A 2023 meta-analysis in JAMDA (PMID 37433427) reported fall incidence and risk factors specifically in nursing home populations
Key Clinical Pearls
| Point | Detail |
|---|---|
| Most common cause of fall-related death | Hip fracture |
| Most common pathophysiology | Orthostatic hypotension |
| Single most dangerous drug class | Benzodiazepines + tricyclics (TCA) |
| Most proven single intervention | Exercise (strength + balance / Tai chi) |
| Who needs full fall risk assessment | Recurrent falls OR any fall + gait difficulty |
| Restraints | No evidence of benefit; cause harm |
| "Long lie" | 50% cannot get up; associated with functional decline |
| Vitamin D | Only reduces falls if patient is deficient |
Pharynx anatomy with simple diagram
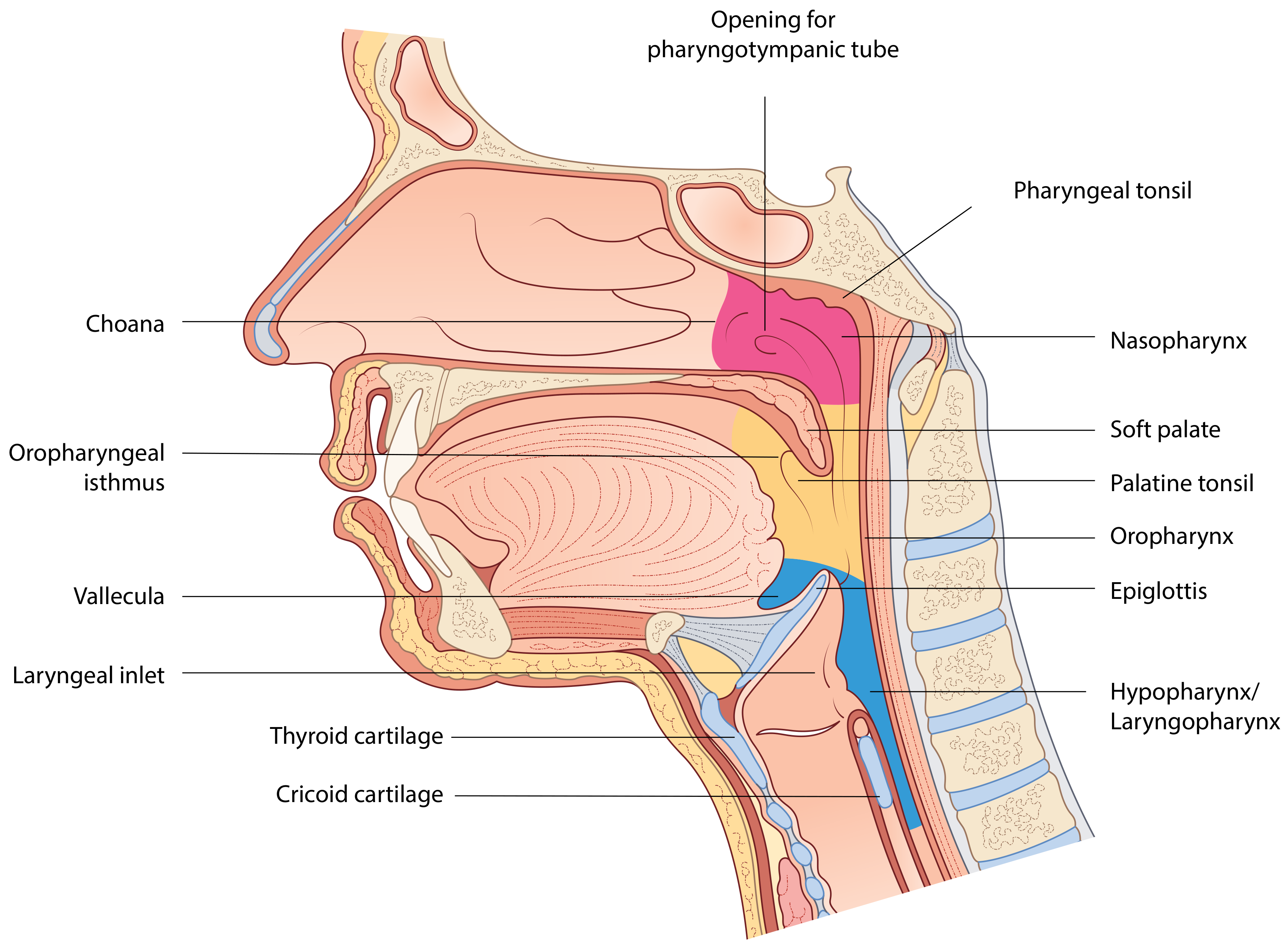
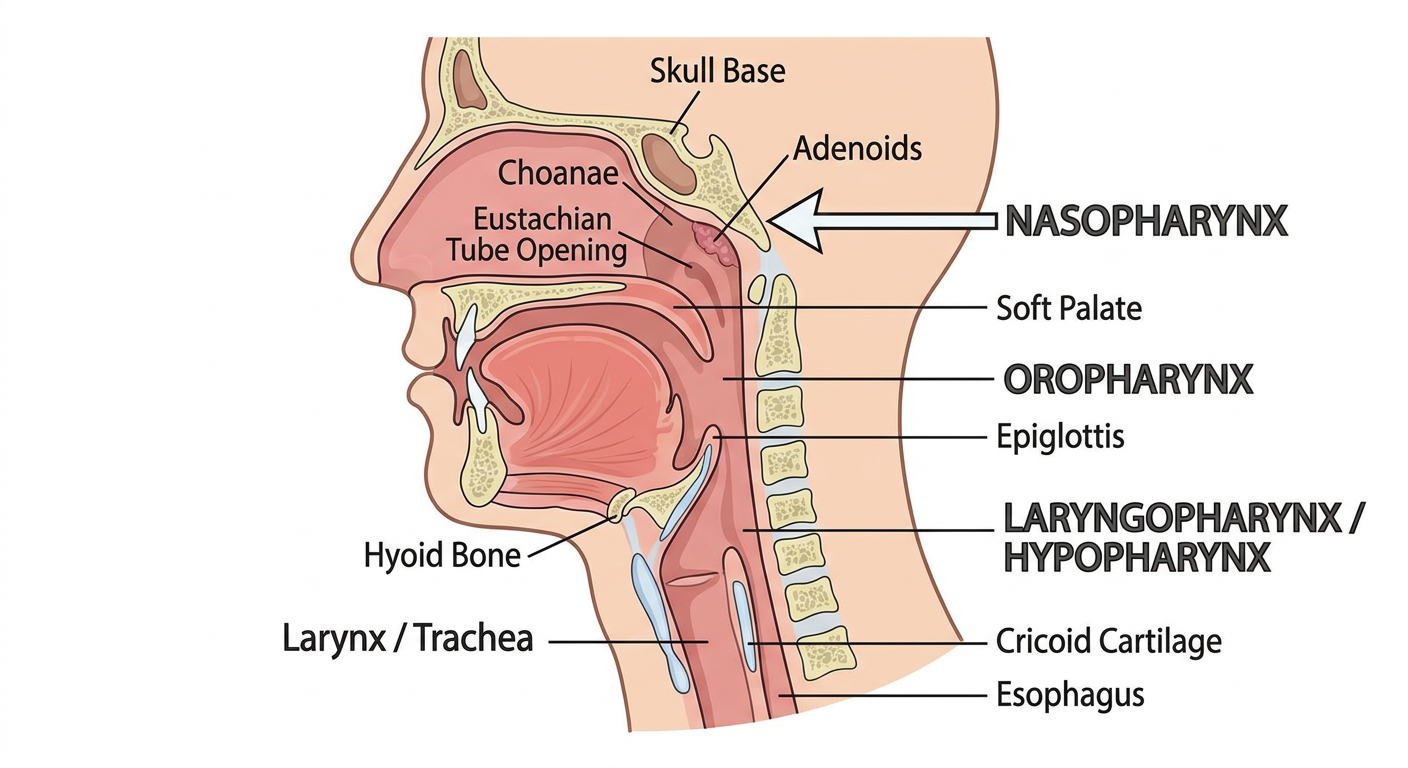
Simple labeled anatomical diagram of the pharynx showing a sagittal (side) cross-section of the head and neck. Label the three parts: Nasopharynx (top, behind nasal cavity), Oropharynx (middle, behind oral cavity), and Laryngopharynx/Hypopharynx (bottom, behind larynx). Show key landmarks: skull base (top), choanae, soft palate (boundary between nasopharynx and oropharynx), epiglottis, hyoid bone (boundary between oropharynx and laryngopharynx), cricoid cartilage (bottom, where pharynx joins esophagus), and the esophagus below. Also mark the Eustachian tube opening in the nasopharynx and the adenoids. Show the larynx/trachea anteriorly. Use clean educational style with clear labels, simple colors, on white background.
Anatomy of the Pharynx
Overview
Simple Diagram (Sagittal Section)
Subdivisions
SKULL BASE
|
[NASOPHARYNX] ← above soft palate, behind choanae
|
Soft palate (boundary)
|
[OROPHARYNX] ← behind oral cavity, soft palate to epiglottis
|
Hyoid bone / pharyngoepiglottic folds (boundary)
|
[LARYNGOPHARYNX / HYPOPHARYNX] ← behind larynx
|
Lower border of cricoid cartilage
|
[ESOPHAGUS]
1. Nasopharynx
- Roof/posterior wall: Sloping sphenoid + occipital (basisphenoid); contains the pharyngeal tonsil (adenoids) - lymphoid tissue maximal in childhood
- Lateral walls: Contain the pharyngotympanic (Eustachian) tube orifice (~1-1.5 cm from posterior end of inferior turbinate), the fossa of Rosenmuller (most common site of nasopharyngeal carcinoma), and tubal tonsils (Gerlach's tonsils)
- Floor: Soft palate
- Anterior: Choanae (posterior nasal apertures), separated by the vomer
2. Oropharynx
- Soft palate and uvula
- Base of tongue (posterior 1/3)
- Palatine tonsils (in tonsillar fossae between anterior and posterior pillars)
- Posterior and lateral oropharyngeal walls
- Valleculae (recesses between base of tongue and epiglottis)
- Pharyngoepiglottic and glossoepiglottic folds
- Encapsulated (unlike other Waldeyer's ring components) - provides a clean dissection plane for tonsillectomy
- Supplied by tonsillar branch of facial artery (enters inferior pole)
- Also supplied by ascending palatine, lingual, ascending pharyngeal, and descending palatine arteries
- Venous drainage via external palatine vein (most common bleeding source in tonsillectomy)
- Lymphatics drain to jugulodigastric node
- True asymmetry of tonsils = concern for malignancy or parapharyngeal mass
3. Laryngopharynx (Hypopharynx)
- Pyriform sinuses (fossae) - most important clinically; extend from pharyngoepiglottic folds to upper cervical esophagus; bounded laterally by thyroid cartilage, medially by aryepiglottic folds
- Posterior hypopharyngeal wall
- Postcricoid region - extends from arytenoid cartilages inferiorly to cricoid, forms anterior wall of hypopharynx
Waldeyer's Ring (Lymphoid Ring of Pharynx)
| Component | Location |
|---|---|
| Pharyngeal tonsil (adenoids) | Roof of nasopharynx (midline) |
| Tubal tonsils (Gerlach's) | Near Eustachian tube orifice |
| Palatine tonsils | Between tonsillar pillars in oropharynx |
| Lingual tonsils | Posterior 1/3 of tongue |
| Lateral pharyngeal bands | Behind posterior tonsillar pillars |
Muscles of the Pharynx
Constrictor Muscles (Outer Circular Layer)
| Muscle | Origin (Anterior Attachment) | Innervation | Action |
|---|---|---|---|
| Superior constrictor | Pterygomandibular raphe, mandible, pterygoid hamulus, base of tongue | Vagus (CN X) | Constricts upper pharynx; forms Passavant's ridge |
| Middle constrictor | Greater horn of hyoid, stylohyoid ligament | Vagus (CN X) | Constricts middle pharynx |
| Inferior constrictor | Oblique line of thyroid cartilage, cricoid cartilage | Vagus (CN X) | Constricts lower pharynx; lower fibers form cricopharyngeus (UES) |
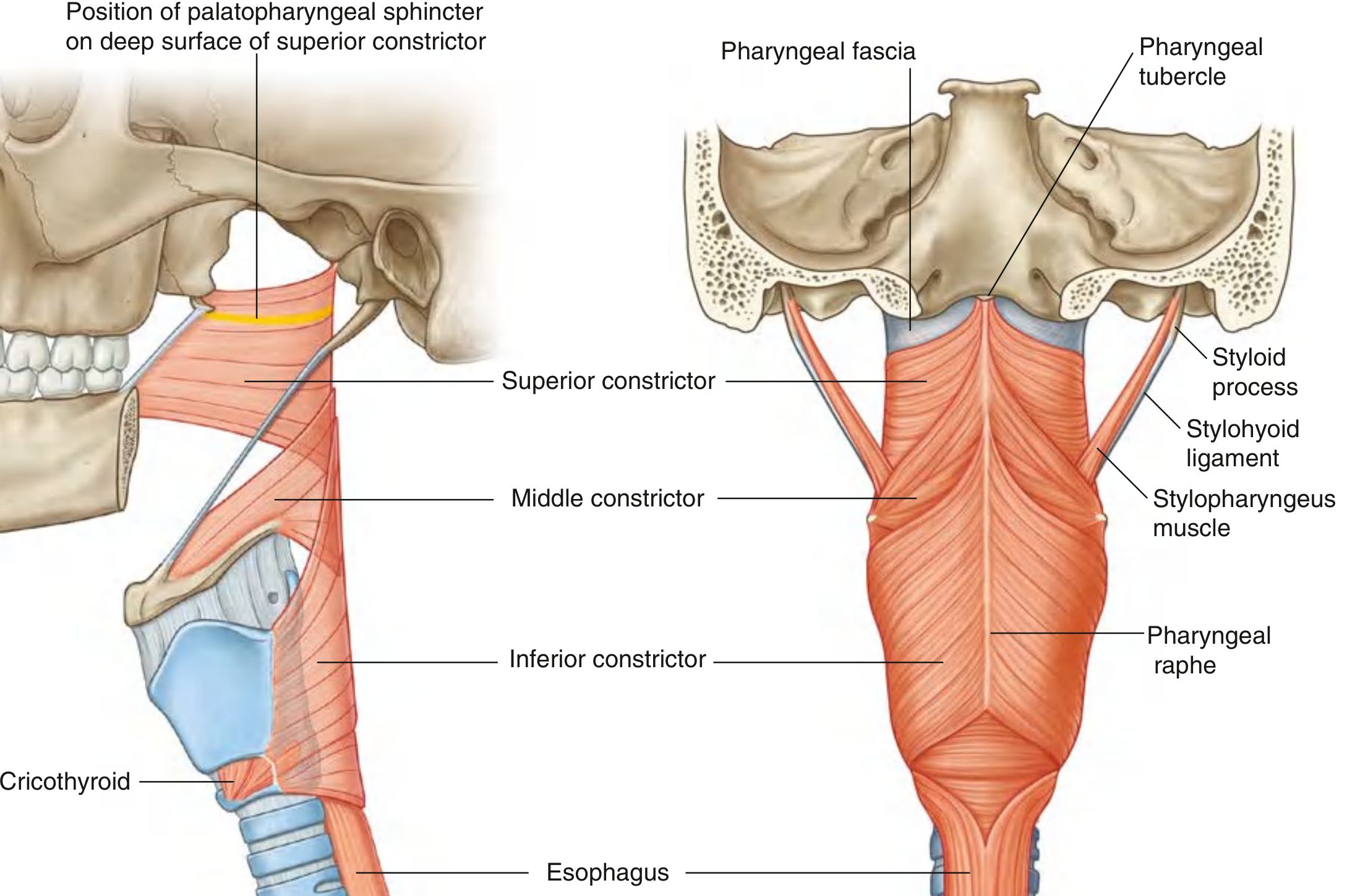
Killian's dehiscence: Gap between cricopharyngeus and inferior constrictor - site of Zenker's diverticulum formation
Longitudinal (Elevator) Muscles (Inner Layer)
| Muscle | Origin | Action |
|---|---|---|
| Stylopharyngeus | Styloid process | Elevates pharynx and larynx; innervated by CN IX (only pharyngeal muscle not by CN X) |
| Palatopharyngeus | Soft palate | Closes oropharyngeal aperture; lowers soft palate |
| Salpingopharyngeus | Eustachian tube cartilage | Elevates pharynx; helps open Eustachian tube |
Soft Palate Muscles (5)
| Muscle | Function | Nerve |
|---|---|---|
| Levator veli palatini | Elevates soft palate (closes nasopharynx during swallowing) | CN X via pharyngeal plexus |
| Tensor veli palatini | Tenses palate; opens Eustachian tube | CN V3 (only soft palate muscle not CN X) |
| Palatoglossus | Narrows oropharyngeal isthmus; approximates palate to tongue | CN X |
| Palatopharyngeus | Raises larynx/pharynx | CN X |
| Musculus uvulae | Shortens uvula | CN X |
Innervation Summary
Motor
- All pharyngeal muscles: Vagus nerve (CN X) via the pharyngeal plexus
- Exception - Stylopharyngeus: Glossopharyngeal nerve (CN IX)
- Exception - Tensor veli palatini: CN V3
Sensory
| Region | Nerve |
|---|---|
| Nasopharynx | Pharyngeal branch of maxillary nerve (CN V2) |
| Oropharynx | Glossopharyngeal nerve (CN IX) - also provides afferent limb of gag reflex |
| Laryngopharynx | Vagus nerve (CN X) via internal laryngeal branch of superior laryngeal nerve |
Referred otalgia: CN IX supplies both the tonsil/oropharynx and the ear (via tympanic nerve) - so tonsillar pathology (abscess, cancer) can present as ear pain.
Blood Supply
- Ascending pharyngeal artery
- Facial artery (ascending palatine + tonsillar branches)
- Maxillary and lingual artery branches
- Inferior thyroid artery (from thyrocervical trunk of subclavian)
Lymphatic Drainage
Epithelium
| Region | Epithelial Type |
|---|---|
| Nasopharynx (anterior) | Ciliated pseudostratified (respiratory) |
| Nasopharynx (posterior) | Non-keratinized stratified squamous |
| Oropharynx | Non-keratinized stratified squamous |
| Laryngopharynx | Non-keratinized stratified squamous |
Key Clinical Points
| Anatomy | Clinical Relevance |
|---|---|
| Fossa of Rosenmuller | Most common origin of nasopharyngeal carcinoma |
| Adenoids | Obstruct Eustachian tube → otitis media with effusion in children |
| Killian's dehiscence (between cricopharyngeus + inferior constrictor) | Site of Zenker's diverticulum |
| Killian-Jamieson space (below cricopharyngeus) | Passage for inferior thyroid artery |
| Eustachian tube orifice | Tensor veli palatini contraction opens it during swallowing |
| External palatine vein | Most common bleeding vessel in tonsillectomy |
| Jugulodigastric node | "Tonsillar node" - first draining node for tonsil infections/cancer |
| CN IX (gag reflex afferent) | Tests oropharyngeal sensory function |
Explain with best diagram inguinal hernia in flowchart
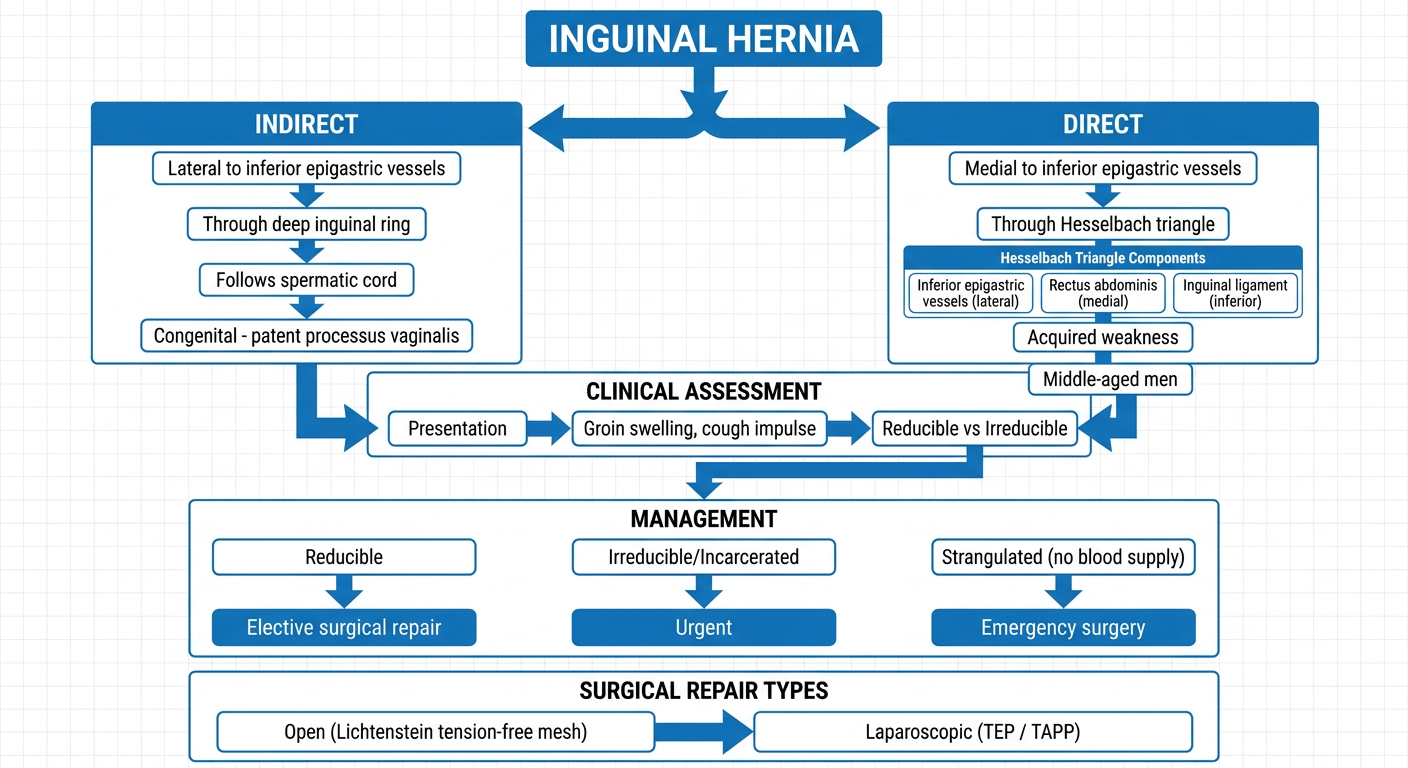
Detailed medical flowchart diagram explaining inguinal hernia. Start at top with "INGUINAL HERNIA" as the title. First branch: two types - "INDIRECT" (lateral to inferior epigastric vessels, through deep inguinal ring, follows spermatic cord, congenital - patent processus vaginalis) and "DIRECT" (medial to inferior epigastric vessels, through Hesselbach triangle, acquired weakness, middle-aged men). Show Hesselbach triangle components below direct type: inferior epigastric vessels (lateral), rectus abdominis (medial), inguinal ligament (inferior). Then show a clinical assessment flow: Presentation → Groin swelling, cough impulse, reducible vs irreducible. Then Management branch: Reducible → Elective surgical repair; Irreducible/Incarcerated → Urgent; Strangulated (no blood supply) → Emergency surgery. Show repair types at bottom: Open (Lichtenstein tension-free mesh) and Laparoscopic (TEP / TAPP). Use clean professional medical flowchart style, blue and white color scheme, clear boxes with arrows, educational infographic look.
Inguinal Hernia - Complete Guide with Diagrams and Flowchart
Main Flowchart
Anatomy Diagram (Bailey & Love)

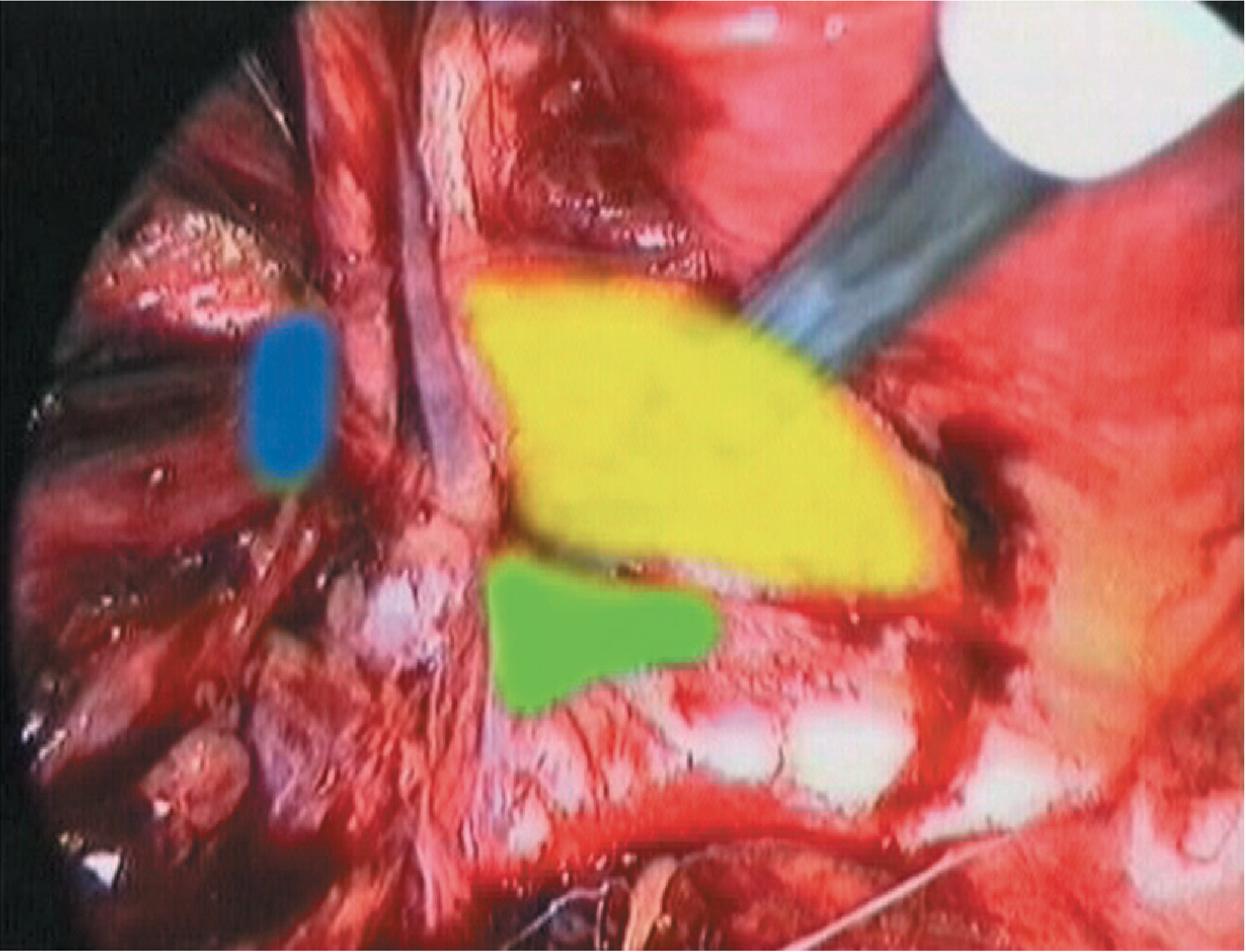
Laparoscopic View: Hernia Defects
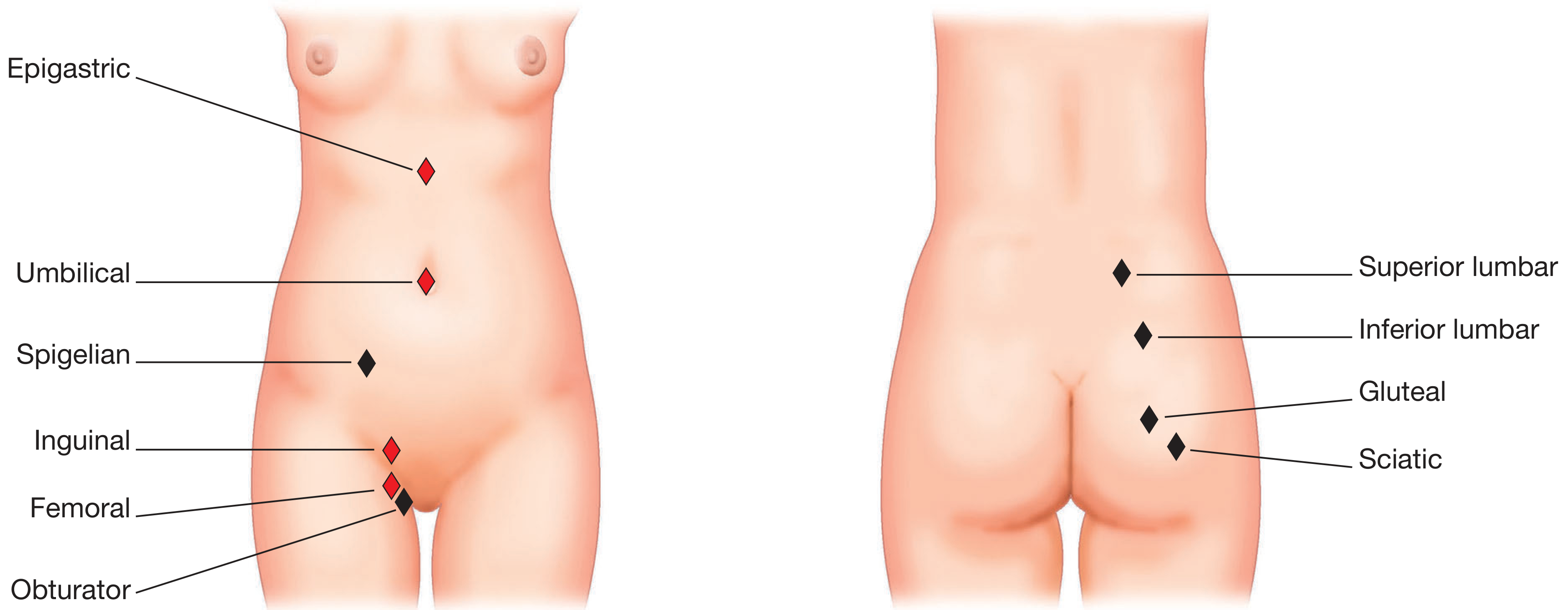
Sites of Abdominal Wall Hernias
Full Structured Explanation
1. What Is It?
2. Inguinal Canal Anatomy (The Key to Understanding)
ANTERIOR SUPERIOR PUBIC
ILIAC SPINE ←4-5cm→ TUBERCLE
↓
DEEP INGUINAL RING SUPERFICIAL (EXTERNAL) RING
(in transversalis (in external oblique
fascia) aponeurosis)
↓————INGUINAL CANAL (4 cm long)————→
| Wall | Structure |
|---|---|
| Anterior | External oblique aponeurosis |
| Posterior | Transversalis fascia |
| Roof | Conjoint tendon (internal oblique + transversus arching over) |
| Floor | Inguinal (Poupart's) ligament (rolled lower edge of external oblique) |
- Males: Testicular artery/veins, vas deferens, lymphatics, cremasteric muscle, ilioinguinal nerve, genital branch of genitofemoral nerve
- Females: Round ligament
3. Types of Inguinal Hernia
INGUINAL HERNIA
│
┌───────────────┴───────────────┐
│ │
INDIRECT (Lateral) DIRECT (Medial)
│ │
┌───────────────┐ ┌─────────────────┐
│ Through DEEP │ │ Through │
│ INGUINAL RING │ │ HESSELBACH'S │
│ (transversalis│ │ TRIANGLE │
│ fascia defect)│ │ (posterior wall │
└───────────────┘ │ weakness only) │
│ └─────────────────┘
Lateral to inferior │
epigastric vessels Medial to inferior
│ epigastric vessels
Follows spermatic cord │
→ may enter scrotum Broad base, rarely
│ enters scrotum
CONGENITAL (patent │
processus vaginalis) ALWAYS ACQUIRED
OR Acquired │
│ Elderly men, muscle
ALL childhood weakness/raised
hernias = indirect intra-abdominal
pressure
4. Hesselbach's Triangle (Direct Hernia Boundary)
Inferior Epigastric Vessels
(LATERAL side)
/
/
Rectus ────────────────
Abdominis HESSELBACH'S
(MEDIAL side) TRIANGLE
────────────────
\
\
Inguinal Ligament
(INFERIOR side)
5. Indirect vs Direct - Key Differences
| Feature | Indirect (Lateral) | Direct (Medial) |
|---|---|---|
| Position | Lateral to inferior epigastric vessels | Medial to inferior epigastric vessels |
| Mechanism | Through deep ring → along canal | Directly through Hesselbach's triangle |
| Type | Congenital (patent processus vaginalis) or acquired | Always acquired |
| Age | Any age (neonates, children, adults) | Middle-aged / elderly men |
| Sac | True peritoneal sac inside spermatic cord | Covered by attenuated transversalis fascia |
| Reaches scrotum? | Yes (follows processus vaginalis) | Rarely (broad-based, pushes forward) |
| Strangulation risk | Higher (narrow neck) | Lower (broad base) |
| Cough impulse control | Controlled by finger over deep ring | NOT controlled by deep ring pressure |
6. Clinical Flowchart: Presentation to Diagnosis
PATIENT PRESENTS WITH GROIN SWELLING
│
┌───────────────┴───────────────┐
│ │
STANDING / COUGHING SUPINE
(swelling appears) (swelling may reduce)
│
CLINICAL EXAMINATION
│
┌─────────────────────┴────────────────────────┐
│ │
REDUCIBLE IRREDUCIBLE
(returns to (cannot reduce
abdomen) manually)
│ │
Cough impulse ┌───────────┴───────────┐
present? │ │
│ INCARCERATED STRANGULATED
│ (bowel stuck, (blood supply
│ no blood supply cut off → ischemia)
│ concern yet) │
│ │ │
│ Urgent reduction EMERGENCY
│ under sedation SURGERY
│ → if fails → surgery
│
├── Press deep inguinal ring → hernia controlled?
│ YES → likely INDIRECT
│ NO (bulges medially) → likely DIRECT
│
Distinguish from:
- Femoral hernia (below inguinal ligament, medial to femoral vein)
- Lymph node
- Hydrocele (transilluminates, can get above it)
- Saphena varix (empties on lying, blue tinge)
- Lipoma of cord
- Undescended testis
7. Special Types
| Type | Description |
|---|---|
| Sliding hernia | Wall of a viscus (sigmoid colon on left, caecum on right, or bladder) forms part of the hernia sac wall - do NOT excise the sac |
| Richter's hernia | Only part of bowel circumference is trapped - can strangulate without obstruction |
| Maydl's hernia | "W" hernia - two loops in sac, middle loop in abdomen strangulates |
| Pantaloon hernia | Both direct AND indirect components straddle inferior epigastric vessels |
| Infantile hernia | Indirect; processus vaginalis not obliterated |
| Scrotal hernia | Massive indirect hernia descending into scrotum |
8. Complications - Priority Flowchart
INGUINAL HERNIA
│
┌─────────────┴──────────────┐
│ │
REDUCIBLE IRREDUCIBLE
(no urgency) (stuck, won't reduce)
│ │
Elective repair INCARCERATED
(no strangulation yet)
│
Attempt manual
reduction (taxis)
- light sedation
- Trendelenburg position
- gentle upward pressure
│
┌────────────┴────────────┐
│ │
REDUCED FAILS / SIGNS OF
│ STRANGULATION
Admit, repair │
next 24 hrs EMERGENCY SURGERY
│
- Bowel resection if
ischemic/necrotic
- Orchidectomy if
testis infarcted
- Tense, irreducible swelling
- Severe constant pain + tenderness
- Overlying skin erythema/edema
- Systemic toxicity: fever, tachycardia, vomiting
- Bowel obstruction signs
9. Investigations
| Investigation | When Used |
|---|---|
| Clinical examination | Diagnosis in most cases |
| Ultrasound | Doubtful diagnosis, occult hernia, scrotal swelling |
| CT scan | Complex cases, large hernias, suspected strangulation, differential diagnosis |
| MRI | Occult/sports hernia (athletic pubalgia) |
| Herniography | Rarely used today |
10. Treatment Flowchart
CONFIRMED INGUINAL HERNIA
│
┌───────────────┴───────────────┐
│ │
ASYMPTOMATIC SYMPTOMATIC
(watchful waiting │
acceptable in SURGICAL REPAIR
low-risk elderly) │
┌───────────────┴───────────────┐
│ │
OPEN REPAIR LAPAROSCOPIC REPAIR
│ │
┌───────────┴───────────┐ ┌──────────┴──────────┐
│ │ │ │
MESH REPAIR SUTURE REPAIR TEP TAPP
(Lichtenstein (Bassini/Shouldice (Totally (Trans-
tension-free - tissue repair) Extraperitoneal Abdominal
mesh - GOLD - no mesh Preperitoneal) Preperitoneal)
STANDARD) - used where │
│ mesh unavailable) Intraperitoneal approach
Mesh over posterior via 3 ports
wall, fixed to │
inguinal ligament & Extraperitoneal
conjoint tendon balloon dissection
- recurrence < 1% - no mesh enters
peritoneum
- faster recovery
- preferred for
bilateral hernias
- preferred for
recurrent hernias
| Repair | Description | Best For |
|---|---|---|
| Lichtenstein (open mesh) | Tension-free polypropylene mesh over posterior wall | Standard unilateral repair, gold standard |
| Shouldice (open suture) | 4-layer transversalis fascia repair, no mesh | Best suture repair; <2% recurrence at expert centres |
| Bassini (open suture) | Conjoint tendon sutured to inguinal ligament | Resource-limited settings |
| TEP (laparoscopic) | Extraperitoneal approach, mesh over defect | Bilateral hernias, recurrent hernias, faster recovery |
| TAPP (laparoscopic) | Transabdominal, mesh fixed intraperitoneally | Same as TEP; better visualization |
11. Post-operative Complications
SURGICAL COMPLICATIONS
│
┌────┴─────┐
EARLY LATE
│ │
- Haematoma - Recurrence (~1% with mesh)
- Wound infection- Chronic groin pain
- Urinary - Mesh infection/migration
retention - Testicular atrophy
- Ilioinguinal - Hydrocele
nerve injury - Vas deferens injury
(→ numbness - Hernia in opposite
inner thigh) groin (common - always
examine other side!)
12. Special Considerations
Quick Memory Aid
INDIRECT DIRECT
"Goes In Deep" "Directly through"
Through Deep ring Through Hesselbach's triangle
Lateral to IEV Medial to IEV
Congenital or acquired Always acquired
Any age Middle-aged/elderly men
Into scrotum Rarely into scrotum
Higher strangulation Lower strangulation risk