Skin tumour
Reading File
Asking for Preferences
All from patho robins
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content. Let me compile the full structured answer from Robbins.
Skin Tumours - Robbins & Cotran Pathologic Basis of Disease
(Chapter 25 - The Skin)
OVERVIEW - Classification
| Category | Tumours |
|---|---|
| Disorders of Pigmentation & Melanocytes | Freckle, Lentigo, Melanocytic Nevus, Dysplastic Nevi, Melanoma |
| Benign Epithelial Tumours | Seborrheic Keratosis, Acanthosis Nigricans, Fibroepithelial Polyp, Epithelial/Follicular Inclusion Cyst |
| Adnexal (Appendage) Tumours | Cylindroma, Syringoma, others |
| Premalignant & Malignant Epidermal Tumours | Actinic Keratosis, Squamous Cell Carcinoma, Basal Cell Carcinoma, Merkel Cell Carcinoma |
| Tumours of the Dermis | Benign Fibrous Histiocytoma (Dermatofibroma), Dermatofibrosarcoma Protuberans |
| Tumours of Cellular Migrants to the Skin | Mycosis Fungoides (CTCL), Mastocytosis |
I. DISORDERS OF PIGMENTATION & MELANOCYTES
1. Freckle (Ephelis)
- Most common pigmented lesion of childhood in lightly pigmented individuals
- Small (1 mm to several mm), tan-red or light brown macules appearing after sun exposure
- Morphology: Hyperpigmentation results from increased melanin in basal keratinocytes - melanocytes are normal in density (may be slightly enlarged)
- Fade in winter, darken in summer - due to changes in degree of pigmentation, NOT number of melanocytes
- Note: Café au lait spots of neurofibromatosis type 1 resemble freckles histologically but are larger, arise independently of sun, and contain macromelanosomes
2. Lentigo
- Common benign localised hyperplasia of melanocytes
- Equal in both sexes, all skin types; most common in infants and children
- Small (5-10 mm), oval, tan-brown macules or patches; can involve mucous membranes
- Morphology: Linear (nonnested) melanocytic hyperplasia restricted to the cell layer immediately above the basement membrane - produces a hyperpigmented basal cell layer
- Unlike freckles, lentigines do NOT darken on sun exposure
3. Melanocytic Nevus (Pigmented Nevus / Mole)
Pathogenesis:
- Benign neoplasms associated with acquired activating mutations in RAS or BRAF (the kinase immediately downstream of RAS)
- Oncogene-induced senescence: the initial activating mutation causes a burst of proliferation followed by permanent cell cycle arrest - this is why nevi grow to a certain size and stop
Types (Table 25.2 summary):
| Type | Location of Nevus Cells | Features |
|---|---|---|
| Junctional nevus | Dermoepidermal junction | Flat, brown; nests of melanocytes at DEJ |
| Compound nevus | DEJ + dermis | Slightly raised; nests at both locations |
| Intradermal nevus | Dermis only | Raised, dome-shaped; most common type in adults; nests entirely in dermis |
| Blue nevus | Deep dermis | Slate-blue colour due to Tyndall effect; spindle-shaped melanocytes deep in dermis |
| Spitz nevus | Compound (usually) | Large epithelioid/spindle cells; mostly in children; often confused with melanoma |
| Congenital nevus | Compound/intradermal | Present at birth; large congenital nevi have increased risk of melanoma |
| Dysplastic nevus | Compound | Irregular borders, variegated colour; see below |
Morphology of common acquired nevus:
- Small (<6 mm), rounded, well-demarcated lesion with uniform pigmentation
- Early: nests of round-to-oval nevus cells at DEJ (junctional component)
- Progression: cells drop off into dermis; junctional activity disappears with age
- Mature intradermal nevi: upper dermal cells may be large and pigmented; deeper cells smaller, spindle-shaped, may form neural-like structures ("neurotization")
- Maturation (cells smaller with depth) distinguishes benign nevi from melanoma
4. Dysplastic Nevi
Key features:
- Larger than common acquired nevi (>5 mm, often >10 mm)
- Irregular, pebbly surface; variable pigmentation; irregular, indistinct borders
- May occur sporadically or in familial clusters (Familial Dysplastic Nevus Syndrome / B-K mole syndrome)
- Patients with familial dysplastic nevi + family history of melanoma have a nearly 100% lifetime risk of developing melanoma
Morphology:
- Architectural disorder: nests of melanocytes that bridge adjacent rete ridges (confluent growth)
- Cytologic atypia: enlarged melanocytes with abundant cytoplasm and large nuclei with prominent nucleoli
- Stromal reaction: lamellar fibroplasia around elongated rete ridges and lymphocytic infiltrate
- Lentiginous proliferation: single melanocytes proliferating along the basal layer beyond the lateral margins of the compound component ("shouldering")
5. Melanoma
One of the most aggressive human malignancies - incidence rising steadily.
Pathogenesis:
| Mutation | Frequency | Significance |
|---|---|---|
| BRAF (V600E) | ~60% of melanomas | Activates MAPK; targetable with vemurafenib |
| NRAS | ~20% | Activates both MAPK and PI3K/AKT |
| NF1 loss | ~15% | Upstream RAS activator; often in older patients |
| KIT | <5% | Acral/mucosal melanomas; targetable |
| CDKN2A (p16/p14ARF) | Common | Tumour suppressor; lost in many melanomas |
| TERT promoter | >70% | Maintains telomere length |
- UV radiation is the main environmental cause; C→T transitions at dipyrimidine sites are the UV mutational signature
- UV suppresses cutaneous immunity (transient defect in innate immunity), reducing elimination of sun-damaged cells
ABCDE warning signs:
- Asymmetry
- Border irregularity
- Color variation (shades of brown, black, red, white, blue)
- Diameter >6 mm
- Evolution (change over time)
Growth phases:
- Radial growth phase (RGP): Horizontal spread within epidermis and superficial dermis; low metastatic potential; melanoma cells lack ability to form tumour masses in dermis
- Vertical growth phase (VGP): Invasion into deeper dermis as an expanding mass; acquisition of metastatic potential; cells have different antigenic profile from RGP cells
Morphological types:
| Type | Features |
|---|---|
| Superficial spreading melanoma | Most common (~70%); prolonged RGP; anywhere on body |
| Lentigo maligna melanoma | On sun-damaged skin of elderly; longest RGP (years-decades) |
| Nodular melanoma | Predominantly VGP from outset; darkly pigmented nodule; most aggressive |
| Acral lentiginous melanoma | Palms, soles, subungual; most common type in dark-skinned individuals; BRAF mutations less common; KIT mutations more common |
Morphology:
- Radial growth: atypical melanocytes (large cells, prominent red nucleoli, irregular nuclear contours) spreading upward (pagetoid spread) and laterally
- Vertical growth: nodular aggregates of cells with mitotic figures invading dermis
- Regression areas: fibrosis, melanophages, lymphocytes
Prognosis - Breslow thickness (most important prognostic factor):
| Breslow Thickness | 5-year Survival |
|---|---|
| <0.76 mm | ~98% |
| 0.76-1.5 mm | ~85% |
| 1.5-4 mm | ~57% |
| >4 mm | ~50% |
Other prognostic factors: mitotic rate, ulceration, sentinel lymph node status, presence of tumour-infiltrating lymphocytes.
II. BENIGN EPITHELIAL TUMOURS
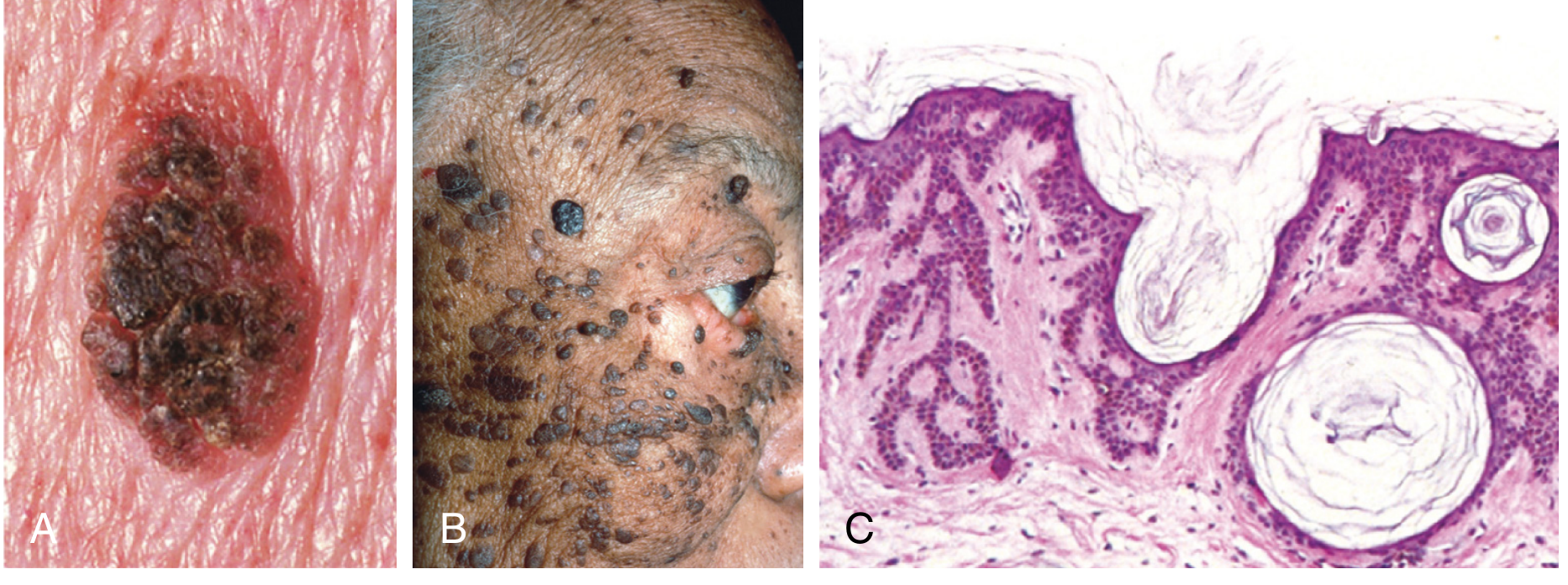
6. Seborrheic Keratosis
- Extremely common, usually in older individuals; rarely seen before age 30
- Appear suddenly in large numbers (Leser-Trélat sign) may indicate internal malignancy (usually GI adenocarcinoma)
Morphology:
- Round, flat-to-raised coin-like lesions with a "stuck-on" greasy appearance; tan to dark brown; sharply demarcated
- Microscopically: proliferation of basaloid (basosquamous) cells with variable melanin; formation of keratin-filled cysts (horn cysts) and pseudo-horn cysts (invaginations of surface keratin)
- Dermatosis papulosa nigra: a variant seen in ~1/3 of African American adults (clinically and histologically identical to seborrheic keratosis)
- Pathogenesis: activating mutations in FGFR3 (identical receptor mutated in achondroplasia) and/or PIK3CA in most sporadic lesions; FGFR3 also mutated in acanthosis nigricans
7. Acanthosis Nigricans
- Thickened, hyperpigmented, velvety skin in flexural areas (axillae, neck folds, groin, anogenital)
- Two types:
- Benign (~80%): childhood/puberty onset; associated with obesity, diabetes (hyperinsulinemia → IGF1R activation), endocrine tumours, or autosomal dominant inheritance (FGFR3 germline mutation)
- Malignant (~20%): middle-aged/older; paraneoplastic - most commonly with GI adenocarcinoma (possibly via TGF-α → EGFR activation)
- Morphology: Undulating epidermal peaks and valleys (papillomatosis), hyperkeratosis, slight basal layer hyperpigmentation - NO melanocytic hyperplasia
8. Fibroepithelial Polyp (Acrochordon / Skin Tag / Squamous Papilloma)
- One of the most common cutaneous lesions; middle-aged and older individuals
- Soft, flesh-coloured polypoid growths on neck, axillae, eyelids, groin
- Covered by normal-appearing epidermis; fibrovascular core
9. Epithelial/Follicular Inclusion Cyst
- Intradermal or subcutaneous cyst lined by stratified squamous epithelium containing laminated keratin
- Rupture causes intense foreign-body inflammatory reaction
III. ADNEXAL (APPENDAGE) TUMOURS
Arise from hair follicles, sweat glands, or sebaceous glands. Generally benign but malignant variants exist.
- Cylindroma: lobules of basaloid cells in a "jigsaw puzzle" pattern; thought to arise from eccrine or apocrine glands
- Syringoma: small ducts lined by flattened epithelium in a dense fibrous stroma; eccrine differentiation; common on lower eyelids
- Most adnexal tumours are benign and locally excised
IV. PREMALIGNANT & MALIGNANT EPIDERMAL TUMOURS
10. Actinic Keratosis (Solar Keratosis)
- The most common precancerous skin lesion; risk of progression to SCC is low for any individual lesion but significant in aggregate
- Caused by UV-induced DNA damage; strongly associated with cumulative sun exposure in lightly pigmented individuals
- Morphology:
- Sandpaper-like rough, scaly erythematous lesions on sun-exposed areas
- Atypical (dysplastic) keratinocytes in the lower epidermis with cytoplasmic pink (dyskeratotic) cells, alternating ortho- and parakeratosis
- Elastosis (solar elastosis) in the dermis
- Atypia confined to the lower portion of the epidermis (unlike full-thickness change of CIS/Bowen disease)
- Bowenoid actinic keratosis: full-thickness epidermal atypia = carcinoma in situ (Bowen disease)
11. Squamous Cell Carcinoma (SCC) of Skin
Second most common tumour on sun-exposed sites (after BCC).
Risk factors:
- UV radiation (most important) - TP53 mutations at pyrimidine dimers are early events
- Immunosuppression (chemotherapy, organ transplantation) - reduces surveillance; HPV subtypes 5 & 8 suspected
- Industrial carcinogens (tars, oils)
- Chronic ulcers, burn scars, draining osteomyelitis
- Arsenical ingestion
- Ionizing radiation
- Xeroderma pigmentosum (defective nucleotide excision repair → rapid mutation accumulation)
- Oral: tobacco, betel nut chewing
Genetics: TP53 (early), RAS activation, Notch signalling loss
Morphology:
- In situ (Bowen disease): sharp, red, scaling plaques; full-thickness epidermal atypia - atypical cells with enlarged hyperchromatic nuclei at ALL levels of epidermis
- Invasive: nodular lesions, variable keratin production (hyperkeratotic scale), may ulcerate
- Variable differentiation: well-differentiated forms make keratin pearls (squamous eddies); poorly differentiated forms show anaplastic cells with rare keratinization
- Desmosomes (intercellular bridges) may be identified
Prognosis: <5% metastasize to regional nodes (far lower than oral/pulmonary SCC), but causes ~8000 deaths/year in the US (similar to metastatic melanoma) due to sheer frequency
12. Basal Cell Carcinoma (BCC)
Most common human malignancy. Locally aggressive but almost never metastasizes.
Pathogenesis:
- UV radiation + Hedgehog (HH) signalling pathway is central
- Loss of PTCH1 (Patched) function → constitutive activation of Smoothened (SMO) → Gli transcription factor activation
- PTCH1 mutations in ~90% of sporadic BCCs (often UV signature mutations)
- Gorlin syndrome (Basal Cell Nevus Syndrome): germline PTCH1 mutation → hundreds of BCCs, jaw cysts, skeletal anomalies, medulloblastoma
- Hedgehog inhibitor vismodegib (SMO inhibitor) is effective in advanced BCC
Morphology:
- Arise on hair-bearing skin; most on face (nose most common site)
- Pearly or translucent papules with telangiectatic vessels; may show central ulceration ("rodent ulcer")
- Microscopically: nests of basaloid cells with large oval nuclei and scant cytoplasm arising from the epidermis
- Characteristic peripheral palisading of nuclei in tumour nests + retraction artefact (clefting) between tumour nests and stroma
- Stromal mucin between tumour nests
- Subtypes: nodular (most common), superficial, morpheaform/sclerosing (most aggressive - infiltrative cords in a dense fibrous stroma; high recurrence)
13. Merkel Cell Carcinoma
- Rare but highly aggressive neuroendocrine carcinoma of the skin
- Arises from Merkel cells (mechanoreceptors in basal epidermis) or their precursors
- Associated with Merkel cell polyomavirus (MCV) integration in ~80% of cases; UV-related TP53 mutations in most MCV-negative cases
- Seen predominantly in elderly, immunocompromised patients
- Morphology: Small blue cells with scant cytoplasm, vesicular nuclei, numerous mitoses; perinuclear dot-like cytokeratin 20 (CK20) positivity on immunostaining (paranuclear dot pattern - pathognomonic)
- High rates of lymph node metastasis; poor prognosis
V. TUMOURS OF THE DERMIS
14. Benign Fibrous Histiocytoma (Dermatofibroma)
- Common benign dermal tumour; most common on legs of women
- Triggered by minor trauma or insect bite in some cases
- Morphology: Firm, tan-brown papule/nodule; overlying epidermis often hyperpigmented
- Histology: whorled proliferation of spindle-shaped fibroblasts/histiocytes with collagen trapping at the periphery
- Overlying epidermis shows basilar hyperpigmentation and pseudoepitheliomatous hyperplasia
- "Dirty finger" pattern - irregular collagen trapping
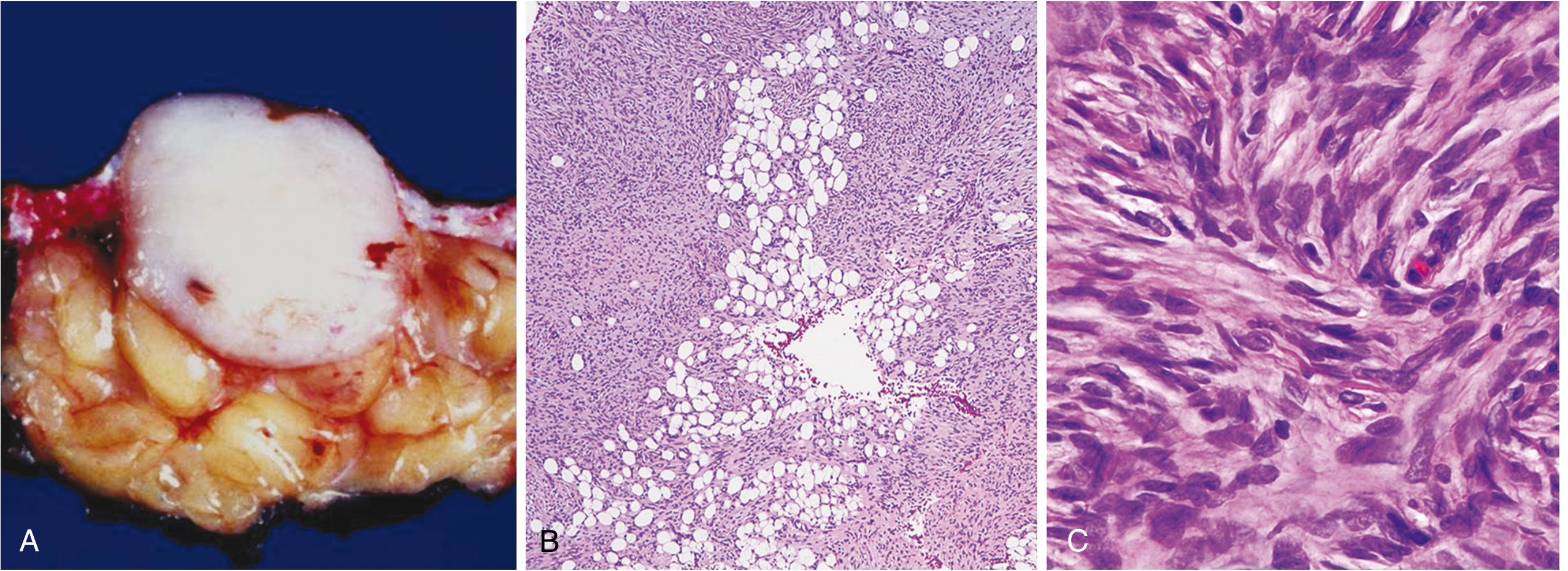
15. Dermatofibrosarcoma Protuberans (DFSP)
- Low-grade malignant fibrous tumour of the dermis; locally aggressive, rarely metastasizes
- Pathogenesis: characteristic translocation t(17;22) creating COL1A1-PDGFB fusion gene → constitutive PDGFR-β signalling; imatinib (PDGFR inhibitor) is effective in unresectable cases
- Morphology:
- Indurated, flesh-coloured plaque that may develop protuberant nodules
- On sectioning: firm, fibrotic nodule
- Histology: storiform (cartwheel/swirling) pattern of spindled cells
- Infiltrates subcutis in a "Swiss cheese" pattern (tumour cords surrounding fat lobules) - accounts for high local recurrence after simple excision
VI. TUMOURS OF CELLULAR MIGRANTS TO THE SKIN
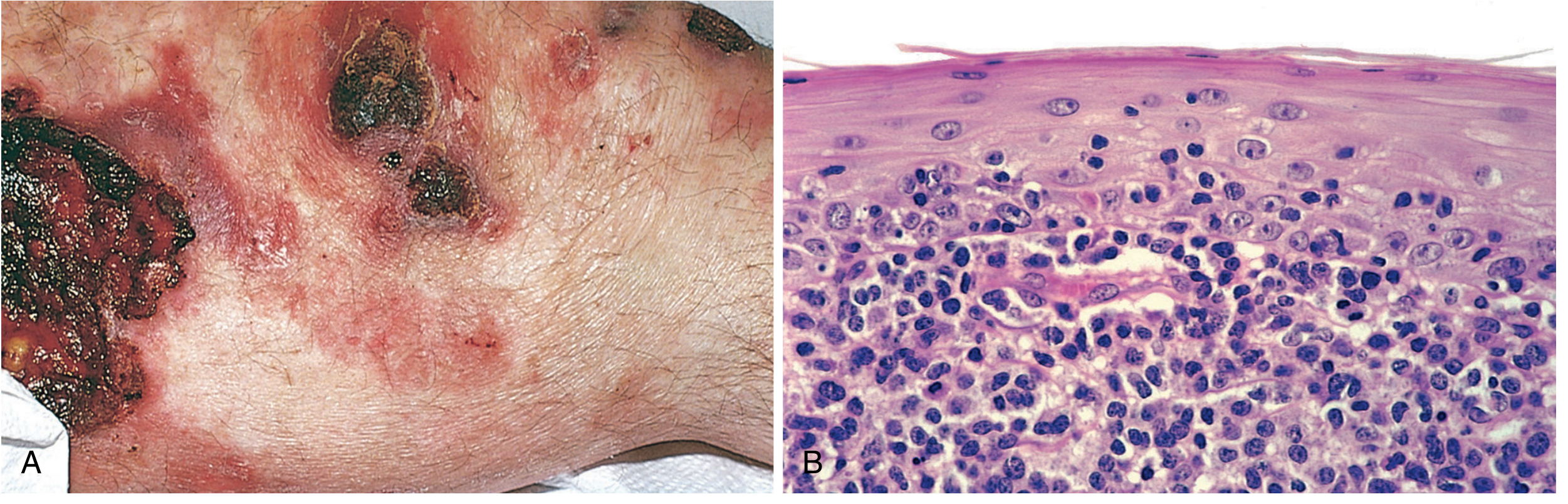
16. Mycosis Fungoides (Cutaneous T-Cell Lymphoma / CTCL)
- Lymphoma of skin-homing CD4+ helper T cells; part of a spectrum of CTCLs
- Most commonly affects persons >40 years old; involves truncal areas
Clinical stages:
- Eczema-like patches - scaly, red-brown patches (early; may persist for years)
- Plaques - raised, scaling, indurated erythematous plaques resembling psoriasis
- Tumour nodules - fungating, may ulcerate; correlates with systemic spread
Morphology:
- Infiltrate of atypical lymphocytes accumulating beneath and invading the epidermis
- Pautrier microabscesses: small intraepidermal aggregates of atypical lymphocytes (pathognomonic)
- Atypical cells have highly convoluted ("cerebriform") nuclei
Immunophenotype: CD4+, CLA+ (cutaneous lymphocyte antigen - responsible for skin homing); aberrant loss of pan-T-cell antigens (CD7 most commonly lost); clonal TCR gene rearrangements
Sézary syndrome: leukemic phase of CTCL - circulating neoplastic T cells (Sézary cells with cerebriform nuclei) + erythroderma
Treatment: topical steroids/UV for early lesions; systemic chemotherapy for advanced disease
17. Mastocytosis
- A spectrum of disorders characterised by accumulation of mast cells in the skin and other organs
- Most common form: urticaria pigmentosa - multiple small, reddish-brown macules and papules that urticate when rubbed (Darier sign - localized urticaria/whealing on stroking a lesion)
- Pathogenesis: Majority caused by activating mutations in c-KIT (CD117), the receptor for stem cell factor (SCF), which is the major growth factor for mast cells; most common mutation is D816V point mutation in KIT
- Morphology: Dense dermal infiltrates of mast cells with round/oval nuclei and abundant pale cytoplasm; metachromatic granules on Giemsa stain; CD117+ on immunohistochemistry
- Systemic mastocytosis can involve bone marrow, liver, spleen; may cause mediator release symptoms (flushing, hypotension, GI symptoms)
Key Comparison Table: BCC vs SCC vs Melanoma
| Feature | BCC | SCC | Melanoma |
|---|---|---|---|
| Origin | Basal cells of epidermis | Squamous keratinocytes | Melanocytes |
| Most common site | Face (nose) | Sun-exposed (face, hands) | Any site (back in men, legs in women) |
| Key driver | PTCH1/HH pathway | TP53, RAS | BRAF V600E (~60%) |
| Metastasis | Almost never | <5% (skin SCC) | Common; early |
| Prognosis | Excellent | Good if caught early | Depends on Breslow depth |
| Key histology | Peripheral palisading + retraction | Keratin pearls, intercellular bridges | Pagetoid spread, VGP |
| Special association | Gorlin syndrome (germline PTCH1) | Xeroderma pigmentosum, immunosuppression | Dysplastic nevi, CDKN2A germline |
Source: Robbins, Cotran & Kumar Pathologic Basis of Disease, Chapter 25 - The Skin
Just explain benign tumour and malignant tumour
Reading File
Reading File
I have enough content. Here is a focused explanation of just the benign and malignant epithelial skin tumours from Robbins.
Benign Epithelial Tumours of the Skin
(Robbins Chapter 25)
These are common tumours derived from the keratinising stratified squamous epithelium of the epidermis, hair follicles, and cutaneous glands. They often closely recapitulate the structures from which they arise. Though usually harmless, some are signs of underlying systemic or visceral malignancy.
1. Seborrheic Keratosis
Who gets it: Middle-aged and older individuals; on the trunk most commonly, also head, neck, extremities.
Pathogenesis:
- Activating mutations in FGFR3 (a receptor tyrosine kinase) drive tumour growth in most sporadic cases
- Leser-Trélat sign: sudden appearance of large numbers of seborrheic keratoses as a paraneoplastic sign, likely due to TGF-α from tumour cells (most commonly GI carcinoma)
Morphology:
- Round to oval, flat, waxy, tan-to-dark-brown plaque with a velvety/granular surface; mm to several cm
- "Stuck-on" greasy appearance; sharp demarcation from adjacent epidermis
- In dark-skinned individuals: appears as multiple small dark lesions on the face - called dermatosis papulosa nigra (present in ~35% of African American adults)
- Hand lens shows small pore-like ostia filled with keratin - helps distinguish from melanoma
Histology:
- Exophytic, sharply demarcated from normal epidermis
- Sheets of small basaloid cells (resembling normal basal cells) with variable melanin
- Horn cysts: small keratin-filled cysts - characteristic
- Invagination cysts: invaginations of keratin into the main tumour mass
- If irritated: whirling squamous differentiation ("eddy currents")
2. Acanthosis Nigricans
What it looks like: Thickened, hyperpigmented, velvety skin in flexural areas - axillae, neck folds, groin, anogenital region
Two types:
| Type | Features |
|---|---|
| Benign (~80%) | Gradual onset, childhood/puberty; associated with obesity, type 2 diabetes (hyperinsulinemia → IGF1R activation), endocrine tumours, or autosomal dominant FGFR3 germline mutation |
| Malignant (~20%) | Middle-aged/older; paraneoplastic - most commonly GI adenocarcinoma; possibly via TGF-α → EGFR activation |
Pathogenesis unifying theme: Disturbance leading to increased growth factor receptor signalling in the skin (FGFR3, IGF1R, or EGFR depending on cause)
Histology:
- Undulating epidermal peaks and valleys (papillomatosis)
- Hyperkeratosis
- Slight basal layer hyperpigmentation - but NO melanocytic hyperplasia (unlike lentigines)
3. Fibroepithelial Polyp (Acrochordon / Skin Tag / Squamous Papilloma)
- One of the most common cutaneous lesions
- Soft, flesh-coloured, pedunculated (polypoid) growths on neck, axillae, eyelids, groin
- Microscopically: normal-appearing epidermis overlying a loose fibrovascular core - no atypia
4. Epithelial / Follicular Inclusion Cyst
- Intradermal or subcutaneous cyst lined by stratified squamous epithelium filled with laminated keratin
- Rupture of the cyst wall → intense foreign-body giant cell inflammatory reaction
Premalignant & Malignant Epidermal Tumours
5. Actinic Keratosis (Solar Keratosis) - Premalignant
Not yet invasive, but considered a direct precursor to SCC.
- Caused by cumulative UV-induced DNA damage in lightly pigmented individuals
- Feels like sandpaper; rough, scaly, erythematous lesion on sun-exposed skin
Histology:
- Atypical (dysplastic) keratinocytes confined to the lower layers of the epidermis (unlike SCC in situ where atypia is full-thickness)
- Dyskeratotic (pink) cells, alternating ortho- and parakeratosis
- Solar elastosis in dermis (degenerated elastic fibres due to UV)
- When atypia becomes full-thickness → Bowen disease (SCC in situ)
6. Squamous Cell Carcinoma (SCC)
Second most common tumour on sun-exposed skin (after BCC). Higher incidence in males except on legs.
Risk factors:
- UV radiation (most important) - TP53 mutations at pyrimidine dimers are early events
- Immunosuppression (organ transplant, chemotherapy)
- Industrial carcinogens (tars, oils)
- Chronic ulcers, burn scars, draining osteomyelitis
- Arsenical ingestion, ionizing radiation
- Xeroderma pigmentosum (defective nucleotide excision repair → rapid mutation accumulation)
- HPV subtypes 5 & 8 in epidermodyplasia verruciformis
Genetics: TP53 (early, UV signature), RAS activation, Notch signalling loss
Morphology:
- In situ (Bowen disease): sharply defined red scaling plaque; full-thickness epidermal atypia - enlarged hyperchromatic nuclei at ALL layers of epidermis
- Invasive SCC: nodular, hyperkeratotic scale (variable keratin production), may ulcerate
- Well-differentiated: keratin pearls (squamous eddies); intercellular bridges (desmosomes) visible
- Poorly differentiated: anaplastic cells, rare keratinization
Behaviour:
- <5% metastasize to regional nodes
- Despite low metastatic rate, causes ~8,000 deaths/year in the US (comparable to metastatic melanoma) due to sheer frequency
7. Basal Cell Carcinoma (BCC)
Most common human malignancy. Locally invasive but almost never metastasizes.
Pathogenesis - Hedgehog (HH) pathway:
- PTCH1 (Patched-1) normally inhibits Smoothened (SMO)
- Loss-of-function mutations in PTCH1 (~90% of BCCs) → constitutive SMO activation → Gli transcription → tumour growth
- UV signature mutations in PTCH1
- Gorlin syndrome (Basal Cell Nevus Syndrome): germline PTCH1 mutation → hundreds of BCCs + jaw cysts + skeletal anomalies + medulloblastoma
- Vismodegib (SMO inhibitor) effective in advanced/unresectable BCC
Morphology:
- Arises on hair-bearing skin; most common site = face (especially nose)
- Grossly: pearly or translucent papule with telangiectatic vessels; may develop central ulceration ("rodent ulcer")
- Histology: nests and cords of basaloid cells (large oval nuclei, scant cytoplasm) emanating from the epidermis
- Peripheral palisading of nuclei at the edge of tumour nests
- Retraction artefact (clefting) between tumour nests and surrounding stroma - characteristic
- Mucin-rich stroma between nests
Subtypes:
| Subtype | Features |
|---|---|
| Nodular | Most common; well-defined pearly nodule |
| Superficial | Erythematous scaly plaque; least aggressive |
| Morpheaform/Sclerosing | Scar-like, indurated plaque; infiltrative cords in dense fibrous stroma; highest recurrence rate after excision |
8. Merkel Cell Carcinoma
- Rare, highly aggressive neuroendocrine carcinoma of the skin
- Arises from Merkel cells (mechanoreceptors in basal epidermis)
- ~80% associated with Merkel cell polyomavirus (MCV) integration into the tumour genome; remaining ~20% have UV-related mutations
- Predominantly in elderly and immunocompromised patients
- Histology: small blue cells, scant cytoplasm, vesicular nuclei, many mitoses
- CK20 immunostain: paranuclear dot-like positivity - pathognomonic
- High rates of lymph node metastasis; poor prognosis
Quick Comparison: Benign vs Malignant Epithelial Tumours
| Feature | Benign (e.g. Seb. Keratosis) | SCC | BCC |
|---|---|---|---|
| Atypia | None | Full-thickness (in situ) / invasive | Basaloid - low-grade |
| Metastasis | Never | <5% | Essentially never |
| Key mutation | FGFR3 | TP53, RAS | PTCH1 (HH pathway) |
| Key histology | Horn cysts, basaloid cells | Keratin pearls, intercellular bridges | Peripheral palisading + retraction artefact |
| Paraneoplastic sign | Leser-Trélat sign | - | Gorlin syndrome |
Source: Robbins, Cotran & Kumar Pathologic Basis of Disease, Chapter 25
This is a shared conversation. Sign in to Orris to start your own chat.