

Can you explain pleth waveform interpretation, it's types
pleth waveform interpretation types pulse oximetry clinical
https://www.myamericannurse.com/the-evolution-of-pulse-oxime…
pleth waveform types normal abnormal pulsus paradoxus respiratory variation perfusion index
Pleth Waveform - Complete Interpretation Guide
What is the Pleth Waveform?
- Signal quality / reliability of SpO2 reading
- Cardiovascular and perfusion status
- Respiratory-cardiac interactions (in intubated/ventilated patients)
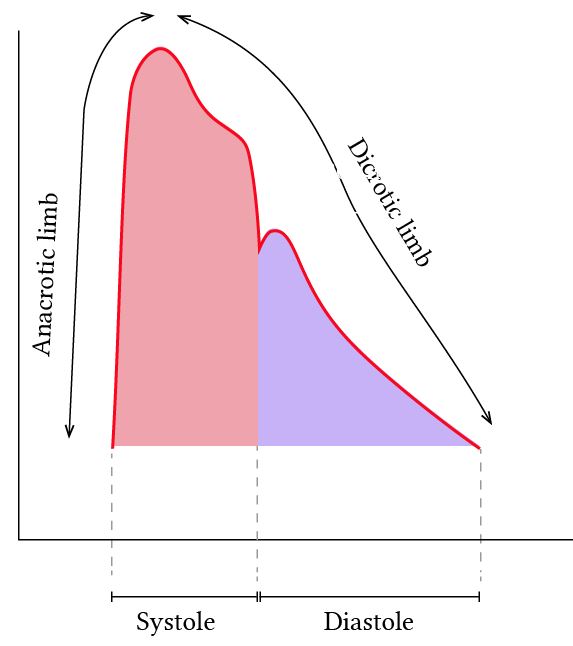
Anatomy of a Single Normal Pleth Wave
Peak (systole)
___
/ \
/ \ <- Dicrotic notch (aortic valve closure)
/ \_/\
/ \___ <- Diastolic trough (baseline)
/
Anacrotic limb (steep upstroke)
| Component | What It Represents |
|---|---|
| Anacrotic limb | Steep upstroke during ventricular systole - rapid ejection of blood |
| Systolic peak | Maximum pulsatile amplitude |
| Dicrotic notch | Aortic valve closure, onset of diastole |
| Catacrotic limb | Descending slope during diastolic runoff |
| Diastolic trough | Baseline, end of cardiac cycle |
Types of Pleth Waveforms
1. Normal Pleth
- Appearance: Regular, consistent amplitude; tall, well-defined peaks; visible dicrotic notch; one wave per heartbeat
- What it means: Good perfusion at probe site, reliable SpO2 reading
- Clinical correlation: Normal cardiac output, adequate vascular tone, well-perfused extremity
2. Low-Amplitude / Dampened Pleth
- Appearance: Small, flat, or barely visible waves
- Causes:
- Peripheral vasoconstriction (cold, shock, vasopressors)
- Hypovolemia
- Poor probe placement or motion artifact
- Hypothermia
- Clinical significance: SpO2 reading is UNRELIABLE when waveform is dampened - treat the reading with caution
3. Respiratory Variation (Respiratory Swing / delta-POP)
- Appearance: Waveform amplitude oscillates up and down with the respiratory cycle
- What it means: Classic sign of hypovolemia / preload responsiveness in mechanically ventilated patients
- Threshold: >13% amplitude variation (delta-POP or PVI >14%) suggests the patient will respond to fluid bolus
- Seen on your monitor as subtle waxing-waning of wave height in the SpO2 channel
- Caution: Only valid in sedated, passively ventilated patients (no spontaneous breathing)
4. Pulsus Paradoxus Pattern
- Appearance: Waveform amplitude drops significantly (visually shrinks) during spontaneous inspiration
- What it means: >10 mmHg drop in systolic BP during inspiration
- Causes: Cardiac tamponade, severe asthma, tension pneumothorax, large pericardial effusion
- Clinical use: A qualitative visual assessment of pulsus paradoxus is possible from the pleth alone, even without an arterial line
5. Pulsus Alternans Pattern
- Appearance: Alternating tall-and-short waveforms in a beat-to-beat pattern
- What it means: Alternating strong and weak cardiac contractions
- Causes: Severe LV dysfunction / heart failure, post-cardioversion, severe hypertension
- Clinical significance: Sign of critically impaired myocardial function
6. Irregular Pleth (Arrhythmia)
- Appearance: Varying amplitude AND irregular intervals between waves
- Causes: Atrial fibrillation (most common), frequent ectopics (PVCs), other arrhythmias
- Clinical note: In AF, each wave has a different height because stroke volume varies beat-to-beat; SpO2 may still be accurate but will seem to flicker
7. Motion Artifact / Noisy Pleth
- Appearance: Chaotic, irregular waves with no recognizable morphology; "noisy" baseline
- Causes: Patient movement, shivering, poor probe contact, electrical interference
- Action: Reposition probe, consider alternative site (ear lobe, forehead); SpO2 value is unreliable
8. Notched / Bifid Pleth
- Appearance: Double peak or exaggerated dicrotic notch
- Causes: Aortic regurgitation (wide pulse pressure), hyperdynamic circulation, sepsis (low SVR states)
- Correlated to: "Bisferiens pulse" on arterial line tracing
Perfusion Index (PI) and Pleth Variability Index (PVI)
| PI Value | Interpretation |
|---|---|
| <0.3% | Very poor perfusion - readings unreliable |
| 0.3 - 1% | Low perfusion - treat SpO2 with caution |
| 1 - 5% | Adequate perfusion |
| >5% | Excellent perfusion / hyperdynamic state |
Quick Bedside Interpretation Checklist
| Check | Normal | Abnormal Action |
|---|---|---|
| One wave per heartbeat? | Yes | Consider arrhythmia |
| All waves same height? | Yes | Look for alternans / AF |
| Waveform tall and well-defined? | Yes | Reposition if flat/small |
| Respiratory swing present? | Minimal | >13% swing - assess fluid status |
| Dicrotic notch visible? | Yes (sometimes) | Not required, but loss may indicate vasoconstriction |
| PI displayed? | >1% | <0.3% - SpO2 unreliable |
Regarding Your Monitor Images
- Monitor 1 (HR 101, SpO2 100%, RR 12): The pleth waveform visible shows somewhat smaller amplitude waves - check PI/PERF value and ensure probe position is adequate.
- Monitor 2 (HR 134, SpO2 100%, BP 106/69, RR 13, 40Y male): The pleth shows larger, more regular waves with visible respiratory variation. Note the PERF value shown is 2.32 - this is adequate. The teal RESP waveform below shows regular breathing cycles. The slight waxing-waning in the pleth at HR 134 with BP 106/69 is worth noting - assess fluid status if this is a post-operative or hemodynamically monitored patient.
Using images
pleth waveform types images normal abnormal pulse oximetry clinical
plethysmography waveform interpretation diagram anacrotic dicrotic notch types
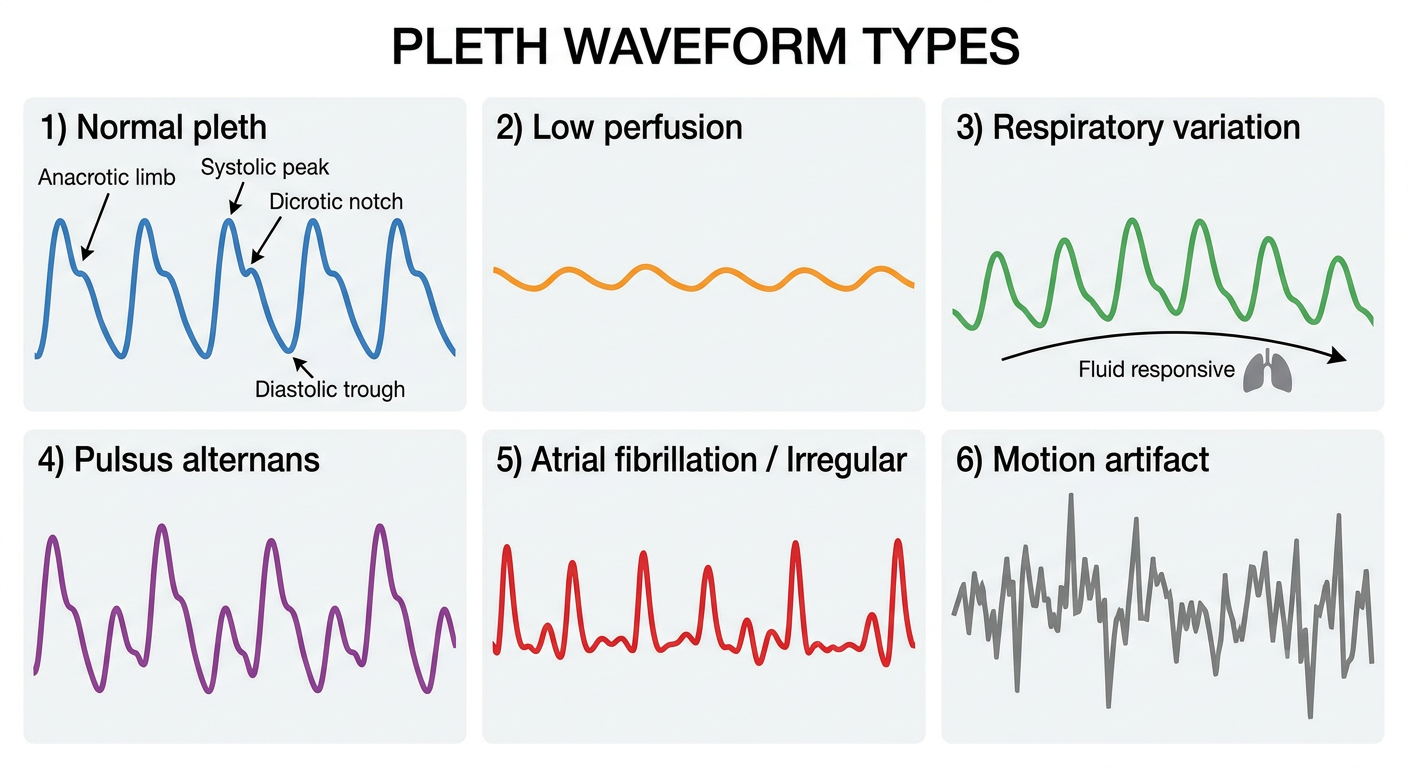
A medical educational diagram showing pleth waveform types side by side with labels: 1) Normal pleth - tall regular waves with visible dicrotic notch, labeled anacrotic limb, systolic peak, dicrotic notch, diastolic trough. 2) Low perfusion - small flattened sinusoidal waves. 3) Respiratory variation - waves that gradually increase then decrease in height in sync with breathing cycle, labeled "fluid responsive". 4) Pulsus alternans - alternating tall and short waves. 5) Atrial fibrillation / Irregular - waves of varying height and irregular spacing. 6) Motion artifact - chaotic noisy waveform. Clean white background, color coded, clinical style.
Pleth Waveform Interpretation - Visual Guide
1. Anatomy of a Single Pleth Wave
| Component | What It Represents |
|---|---|
| Anacrotic limb (upstroke) | Ventricular systole - rapid blood ejection into aorta |
| Systolic peak | Maximum pulsatile flow |
| Dicrotic notch | Aortic valve closure - onset of diastole |
| Dicrotic limb (downstroke) | Diastolic runoff into periphery |
| Diastolic trough | End of one cardiac cycle |
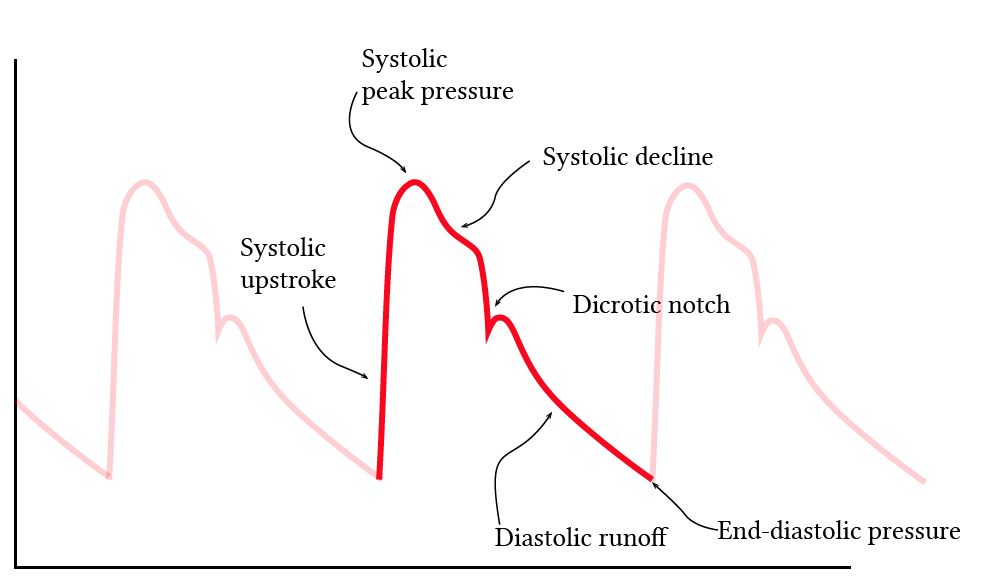
2. Labeled Normal Waveform with Cardiac Events

3. The 4 Core Pleth Types at the Bedside
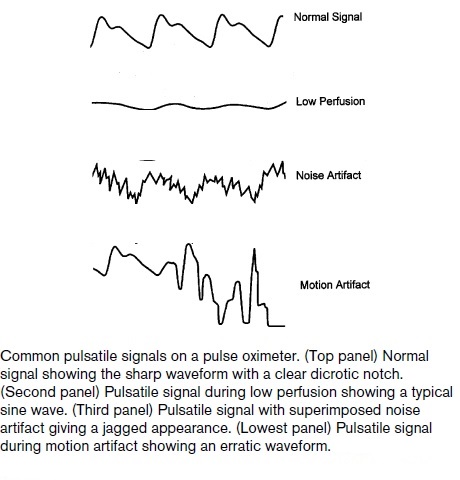
| Type | Appearance | Meaning |
|---|---|---|
| Normal | Sharp, tall waves with clear dicrotic notch | Good perfusion, reliable SpO2 |
| Low perfusion | Small, sine-wave-like, flattened | Vasoconstriction, hypovolemia, hypothermia |
| Noise artifact | Jagged, irregular baseline | Electrical interference, shivering |
| Motion artifact | Erratic, unpredictable spikes | Patient movement - SpO2 unreliable |
4. Clinical Pleth Interpretation Table (Nursing/Clinical Reference)
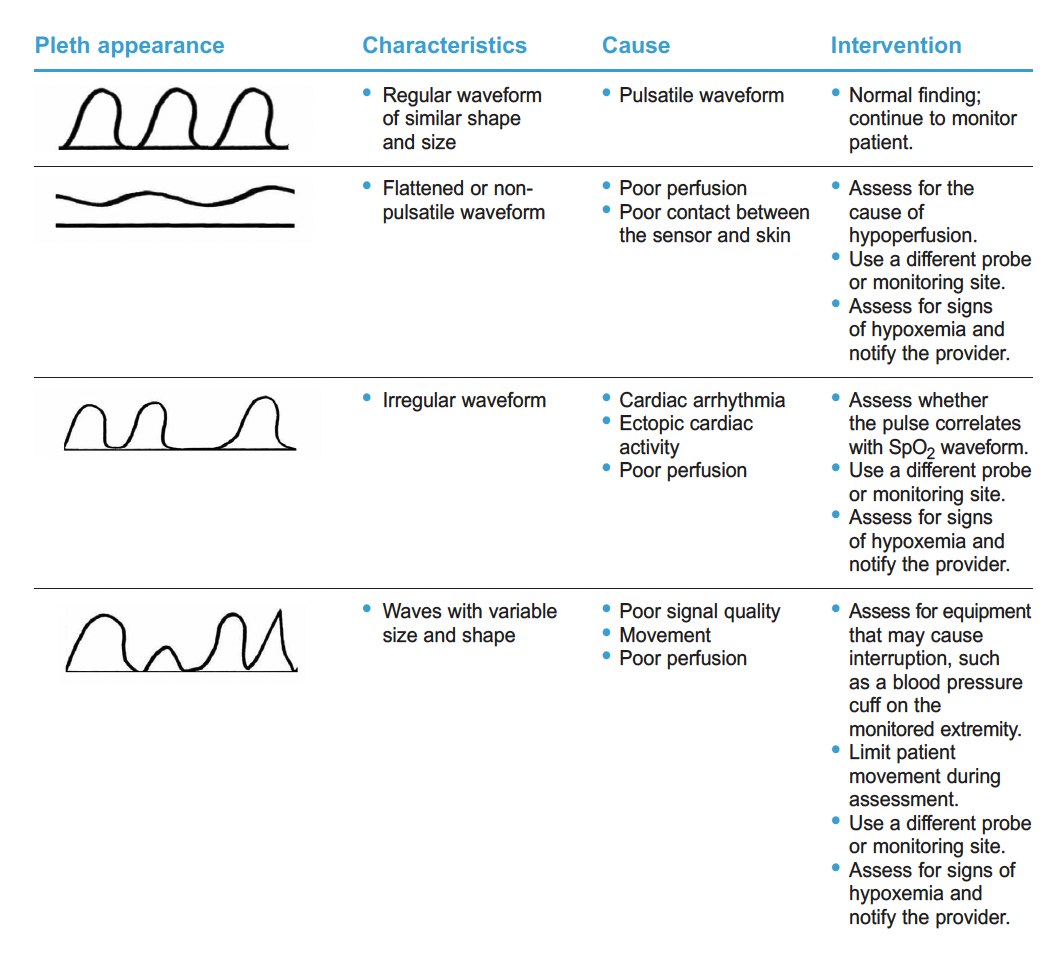
- Regular, same size = Normal, continue monitoring
- Flattened/non-pulsatile = Poor perfusion or poor probe contact - investigate and reposition
- Irregular spacing/varying heights = Arrhythmia (AF, ectopics) - check ECG
- Variable size AND shape = Movement or poor signal - limit movement, resite probe
5. Pulse Type Classification with Disease Correlation

| Waveform Type | Physiological Cause | Possible Disease |
|---|---|---|
| Normal | Normal stroke volume + SVR | - |
| Small and weak | Decreased stroke volume / increased peripheral resistance | Heart failure, hypovolemia |
| Large and bounding | Increased stroke volume / decreased SVR | Fever, anaemia, aortic regurgitation, TBI |
| Pulsus alternans | Alternating stroke volumes beat-to-beat | LV failure |
| No dicrotic notch | Increased arterial resistance | Coronary heart disease, arteriosclerosis |
| Chaotic | Arrhythmia / motion artifact | VT, VF, AF, movement |
6. Waveform Changes with Aortic Valve Pathology
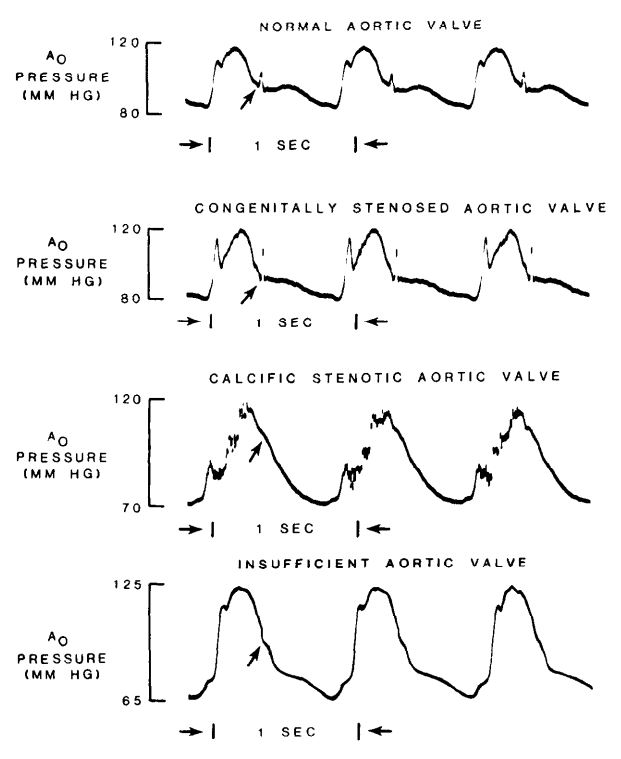
- Normal aortic valve: Clean dicrotic notch visible
- Congenital/calcific aortic stenosis: Slurred upstroke, delayed peak (pulsus parvus et tardus), blunted or absent notch
- Aortic insufficiency: Wide pulse pressure, absent notch, tall bounding wave
7. Overview - All Pleth Types in One Diagram
8. Advanced: Respiratory Variation in the Pleth (Ventilated Patients)
- Minimal variation (<13%) = Normal, adequate preload
- Significant variation (>13-14%) = Fluid responsiveness - the patient will likely respond to IV fluids
- This is called delta-POP (respiratory variation in plethysmographic waveform amplitude)
- On Masimo monitors, this is automatically calculated as PVI (Pleth Variability Index)
- Valid only in fully sedated, passively ventilated patients on controlled-mode ventilation
Quick Bedside Decision Chart
Pleth visible?
├── NO → Reposition probe, try earlobe/forehead
└── YES
├── Regular + same height?
│ ├── YES → Normal. SpO2 reliable.
│ └── NO
│ ├── Alternating tall/short → Pulsus alternans (check cardiac function)
│ ├── Varying height + irregular → AF or ectopics (check ECG)
│ └── Waxing-waning with breathing → Assess fluid responsiveness
└── Small/flat waves?
├── Check PI (Perfusion Index)
├── <0.3% → SpO2 unreliable
└── Warm the limb, resite probe, consider shock/vasoconstriction
Anachrotic and dicrotic notch
anacrotic limb dicrotic notch arterial pulse waveform physiology explanation
anacrotic notch aortic stenosis dicrotic notch absent clinical significance waveform
Anacrotic Limb & Dicrotic Notch - Deep Dive
The Two Limbs of the Arterial/Pleth Waveform
Part 1: The ANACROTIC Limb (Upstroke)
- Aortic valve opens → LV ejects blood rapidly into the aorta
- Pressure rises steeply as blood volume suddenly fills the aortic root
- Continues rising until ejection rate slows (reduced ejection phase)
- Reaches systolic peak pressure (SBP)
| Upstroke character | Meaning |
|---|---|
| Steep, sharp upstroke | Good LV contractility, normal SVR |
| Slow, gradual upstroke (pulsus tardus) | Obstruction to ejection = Aortic stenosis |
| Very steep + tall | High CO, low SVR (sepsis, fever, AR) |
The Anacrotic NOTCH (shoulder on the upstroke)
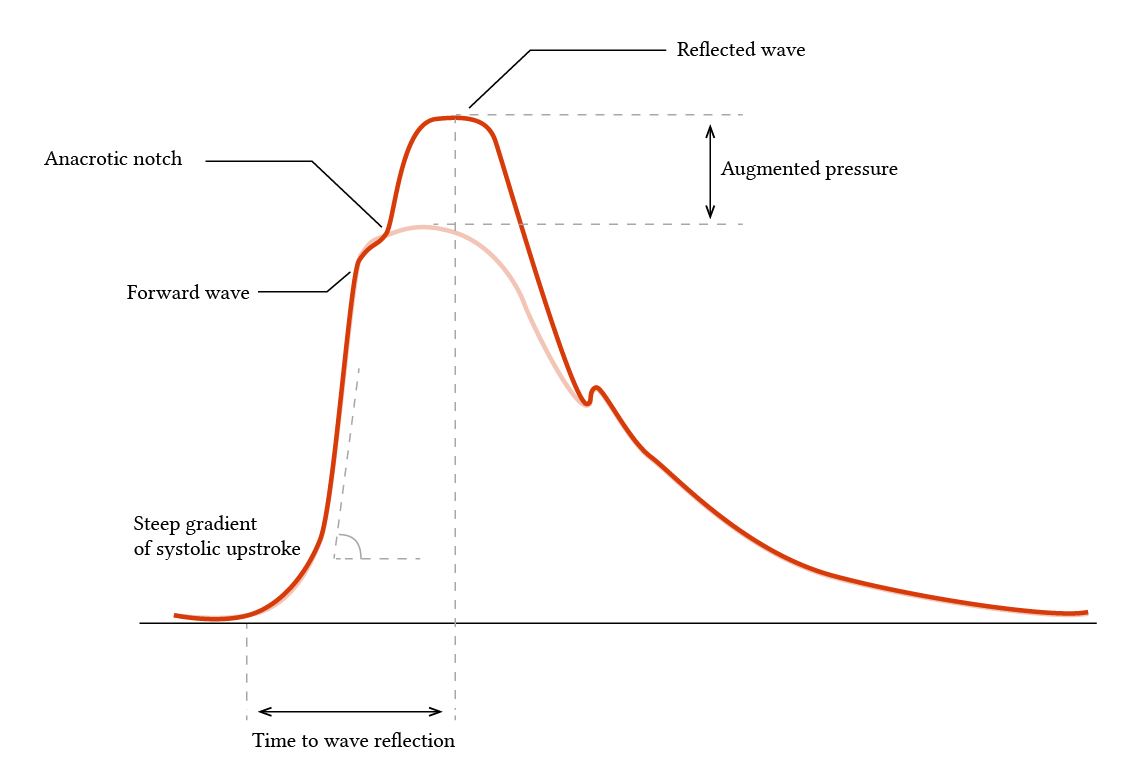
- Seen in hypertension and elderly patients (stiff arteries, early wave reflection)
- Specifically prominent in aortic stenosis - where it distorts the slurred upstroke
- On the pleth: appears as a double hump or shoulder on the rising edge of each wave
Part 2: The DICROTIC Notch
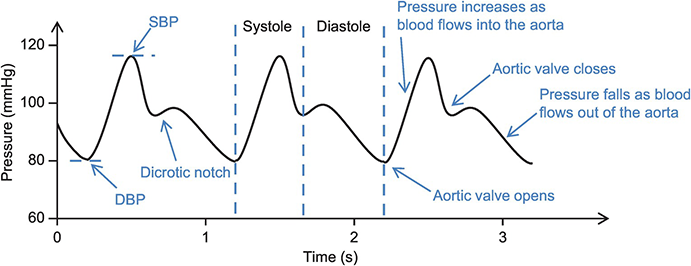
Mechanism Step-by-Step:
LV pressure drops below aortic pressure
↓
Blood briefly reverses flow back toward the ventricle
↓
Aortic valve snaps SHUT
↓
Small transient pressure rise as the closed valve
bounces blood back into the aorta
↓
This appears as the DICROTIC NOTCH on the waveform
↓
Followed by gradual diastolic runoff to periphery
Incisura vs. Dicrotic Notch - Important Distinction
| Feature | Incisura | Dicrotic Notch |
|---|---|---|
| Location | Measured in the aorta | Measured in peripheral arteries |
| Cause | True aortic valve closure | Mixture of reflected waves + valve closure |
| Appearance | Sharp, deep cut into waveform | Softer, more rounded |
| On your pleth monitor | Not seen directly | This is what you see on SpO2 pleth |
As you move from aorta → radial → fingertip, the sharp incisura becomes a rounder dicrotic notch, and gradually shifts lower and later on the downstroke.
Part 3: Age-Related Changes in Both Notches
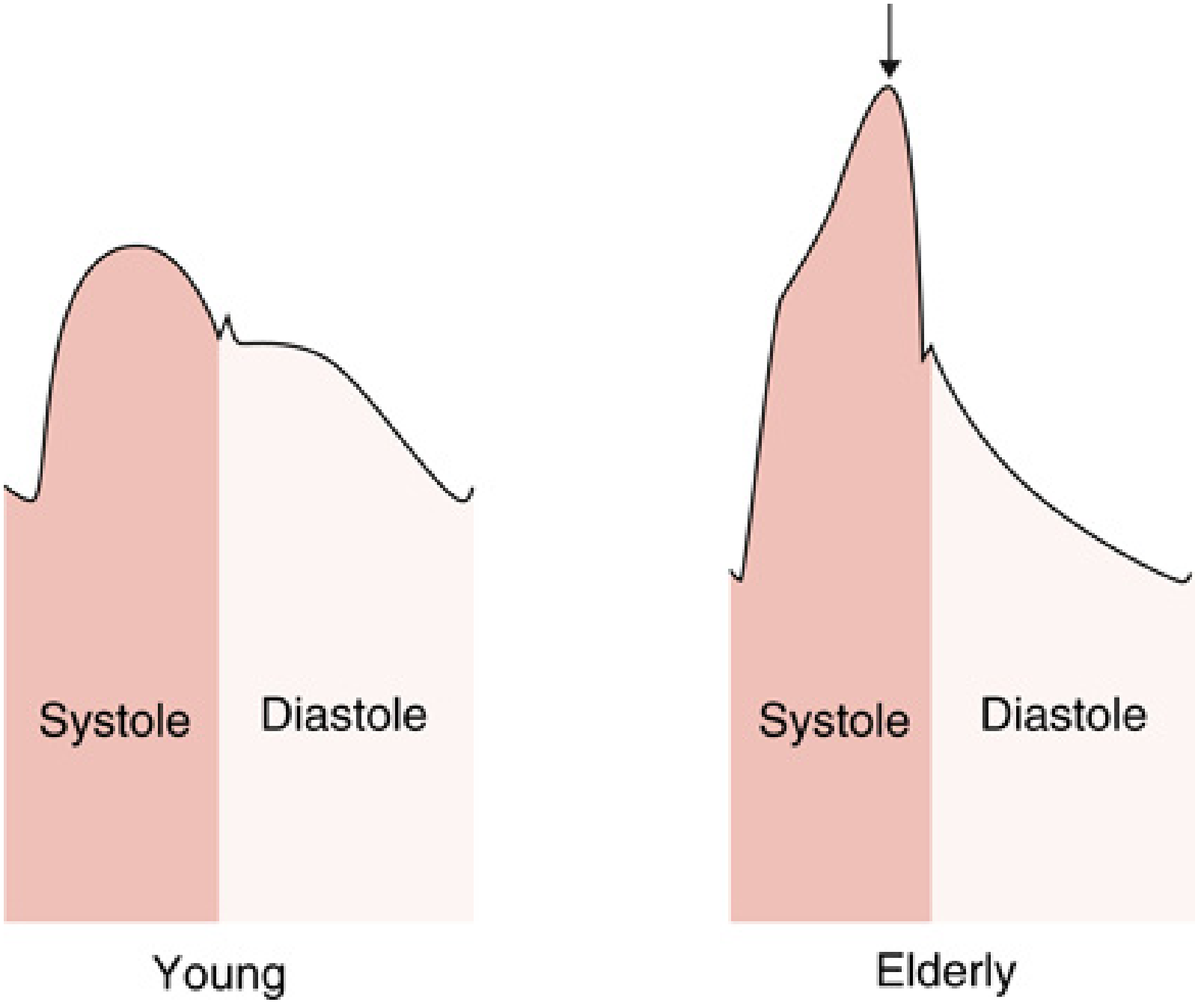
| Young (compliant arteries) | Elderly (stiff arteries) |
|---|---|
| Reflected wave returns late in diastole | Reflected wave returns early in systole |
| Dicrotic notch visible and well-placed | Notch may be absent or blurred |
| Rounded systolic peak | Sharp, narrow systolic peak + anacrotic notch |
| Lower pulse pressure | Higher pulse pressure |
Part 4: Clinical Significance - What Notch Changes Tell You
Dicrotic Notch Position
| Notch position | Meaning |
|---|---|
| High on downstroke (early) | High SVR / vasoconstriction |
| Low on downstroke (delayed) | Low SVR / vasodilation, hypovolemia |
| Absent notch | Severe vasoconstriction, aortic stenosis, overdamped arterial line |
| Very prominent / accentuated | Low SVR states (sepsis), hyperdynamic circulation |
Anacrotic Notch / Abnormal Upstroke - Disease States
| Finding | Disease |
|---|---|
| Slow upstroke + anacrotic shoulder on upstroke | Aortic stenosis (pulsus parvus et tardus) |
| Double systolic peak (bisferiens) | Aortic regurgitation or HOCM |
| Spike-and-dome shape | Hypertrophic obstructive cardiomyopathy (HOCM) |
| Steep upstroke + absent notch + wide pulse pressure | Aortic regurgitation |
From Miller's Anesthesia: "In aortic stenosis, a distinct shoulder termed the anacrotic notch often distorts the pressure upstroke and the dicrotic notch may not be discernible. These features may make the arterial pressure waveform appear overdamped."
Summary Diagram
Systolic Peak (SBP)
/\
Anacrotic / \ Systolic decline
limb / \
(upstroke) / \___ ← Dicrotic notch (aortic valve closes)
/ \
Baseline / \___________ End-diastolic pressure (DBP)
↑
Anacrotic notch
(shoulder on upstroke,
= early reflected wave,
prominent in HTN/AS/elderly)
- Anacrotic limb = upstroke = LV ejection power
- Anacrotic notch = shoulder on upstroke = reflected wave or obstruction (think AS)
- Dicrotic notch = notch on downstroke = aortic valve closes = end of systole
- Dicrotic limb = downstroke = diastolic runoff