Alkaline phosphatase 10 marks pg answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Now I have comprehensive data. Let me compose the full 10-mark PG-level answer.
Alkaline Phosphatase (ALP) - 10 Marks
1. Introduction & Chemistry
Alkaline phosphatase (ALP) is a group of zinc-containing metalloenzymes that catalyze the hydrolysis of organic phosphate esters in an alkaline environment (optimum pH ~9). The enzyme is bound to cell membranes (ectoenzyme) and is widely distributed throughout the body. ALP requires zinc as a cofactor; copper can displace zinc (as in Wilson disease), reducing its activity.
- Normal reference range (adults): ~30-120 IU/L (varies by lab and method)
- Serum half-life: ~7 days
- Measurement: Colorimetric method - rate of p-nitrophenol (pNP) formation from hydrolysis of para-nitrophenylphosphate (pNPP) at 410 nm
2. Isoenzymes and Sources
ALP activity is concentrated in bone, liver, intestine, and placenta. By electrophoresis, 4 major isoenzymes are identified:
| Source | Heat/Urea Inhibition | L-Phenylalanine Inhibition | Anodal Mobility |
|---|---|---|---|
| Biliary (Liver) | + (50%) | - | 1 (fastest) |
| Bone | +++ (90%) | - | 2 |
| Placental | - (0%) | +++ | 3 |
| Intestinal | + | +++ | 4 |
Key memory aid:
- Bone burns (90% heat inactivation)
- Placenta is heat-stable (0% inactivation) but L-phenylalanine-sensitive
- Intestinal isoenzyme is also L-phenylalanine-sensitive
Special isoenzyme:
- Regan isoenzyme: A placental-like ALP isoenzyme found in small proportions of malignant disease (e.g., lung, breast cancers) - acts as a tumor marker
In the liver, ALP is located on the canalicular membrane of hepatocytes; its precise function is not fully defined.
(Source: Quick Compendium of Clinical Pathology 5e; Sleisenger & Fordtran's GI and Liver Disease)
3. Normal Physiologic Variations
ALP levels vary significantly with physiologic state:
- Age: Adolescents have levels 2x adult values due to active bone growth (bone ALP). Levels rise again after age 30 in both sexes
- Sex: Slightly higher in men; perimenopausal women approach male levels; a healthy 65-year-old woman has ALP ~50% higher than a 30-year-old woman
- Pregnancy: Third trimester significantly elevates ALP due to placental isoenzyme
- Postprandial: Eating a fatty meal elevates ALP by ~30% for up to 12 hours in blood group O and B secretors (intestinal isoenzyme released) - hence fasting sample is preferred
- Oral contraceptives and medications: May elevate ALP
4. Conditions Causing ELEVATED ALP
A. Hepatobiliary Causes (Cholestatic pattern)
Hepatobiliary disease increases ALP through induced synthesis and leakage into serum, mediated by bile acids.
| Condition | Mechanism |
|---|---|
| Obstructive jaundice (choledocholithiasis, cholangiocarcinoma) | Bile duct obstruction - bile acid-induced synthesis |
| Primary biliary cholangitis (PBC) | Antimitochondrial antibody-positive; intrahepatic cholestasis |
| Primary sclerosing cholangitis (PSC) | Associated with IBD |
| Drug-induced cholestasis | e.g., chlorpromazine, oral contraceptives |
| Hepatic infiltration / metastases | ALP is the most sensitive marker of hepatic metastases among liver enzymes |
| Granulomatous disease (sarcoidosis, TB) | Infiltrative hepatic involvement |
| Sepsis, amyloidosis, Langerhans cell histiocytosis | Rare infiltrative causes |
B. Bone Causes
Bone ALP is produced by osteoblasts and reflects bone-forming activity (not resorption).
| Condition | Notes |
|---|---|
| Paget disease | Most common cause of markedly elevated bone ALP in adults |
| Healing fractures | Transient elevation |
| Rickets / Osteomalacia | Compensatory osteoblastic activity |
| Hyperparathyroidism (primary/secondary) | Increased bone turnover |
| Osteogenic sarcoma / Bone metastases | |
| Acromegaly | Increased bone turnover |
| Physiologic (growth spurts, pregnancy) |
C. Other Causes
- Malignancy: Regan isoenzyme (ectopic ALP production)
- Renal disease: Renal tubular cells
- Thyroid disorders: Hyperthyroidism (bone effect)
- Benign familial elevation: Intestinal ALP (asymptomatic)
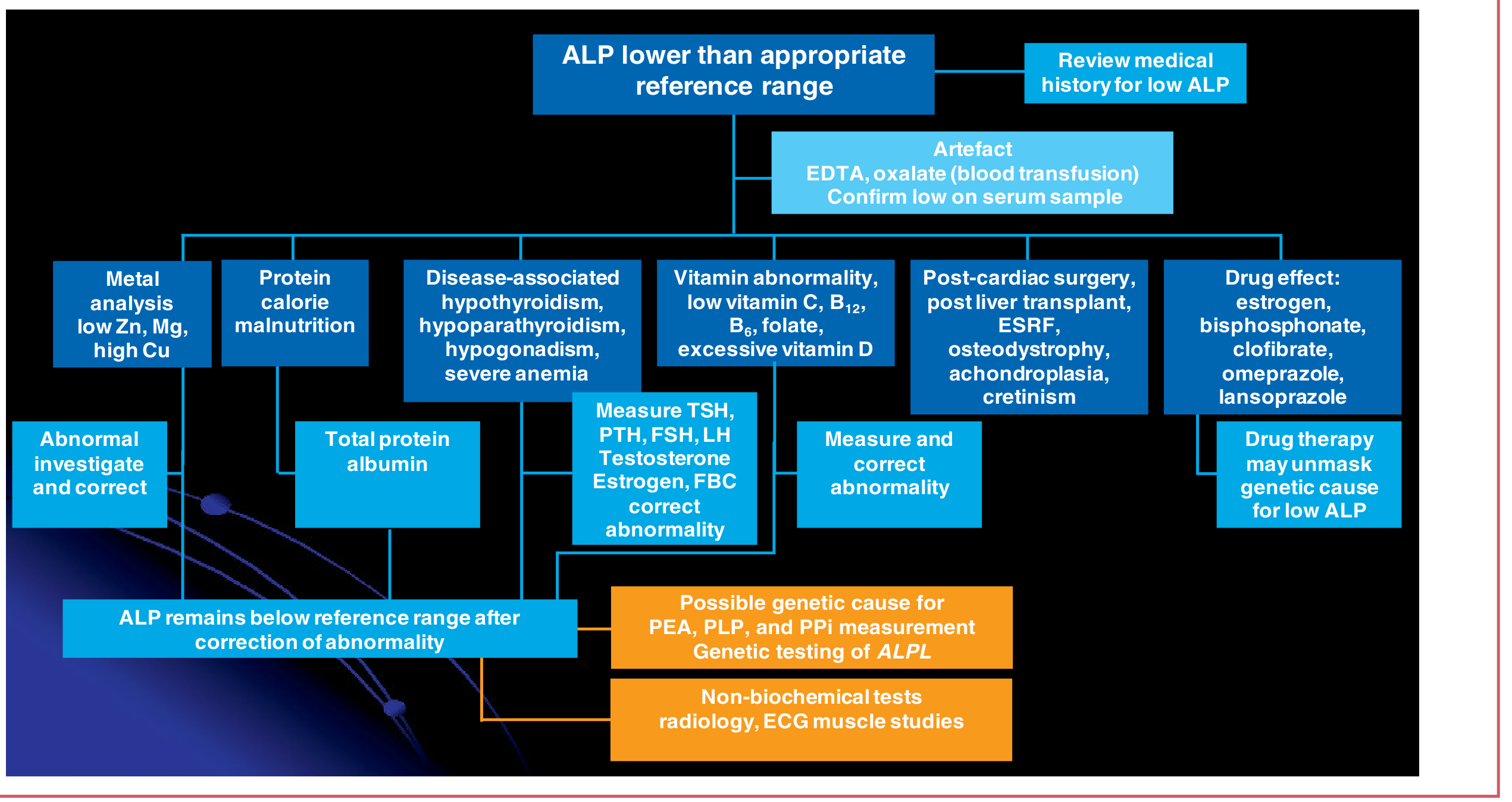
5. Conditions Causing DECREASED ALP
| Condition | Mechanism |
|---|---|
| Hypophosphatasia | Inborn deficiency of ALP gene (ALPL) - leads to rickets-like bone disease |
| Malnutrition / Zinc deficiency | ALP requires zinc as cofactor |
| Wilson disease | Copper displaces zinc from the enzyme; classic in acute liver failure with hemolysis |
| Hypothyroidism | Reduced bone turnover |
| Pernicious anemia | |
| Cardiac surgery with bypass (transient) | |
| Hemolysis | Falsely lowers ALP in vitro |
| Estrogen therapy, theophylline | Drug-related |
(Source: Quick Compendium of Clinical Pathology 5e; Goldman-Cecil Medicine)
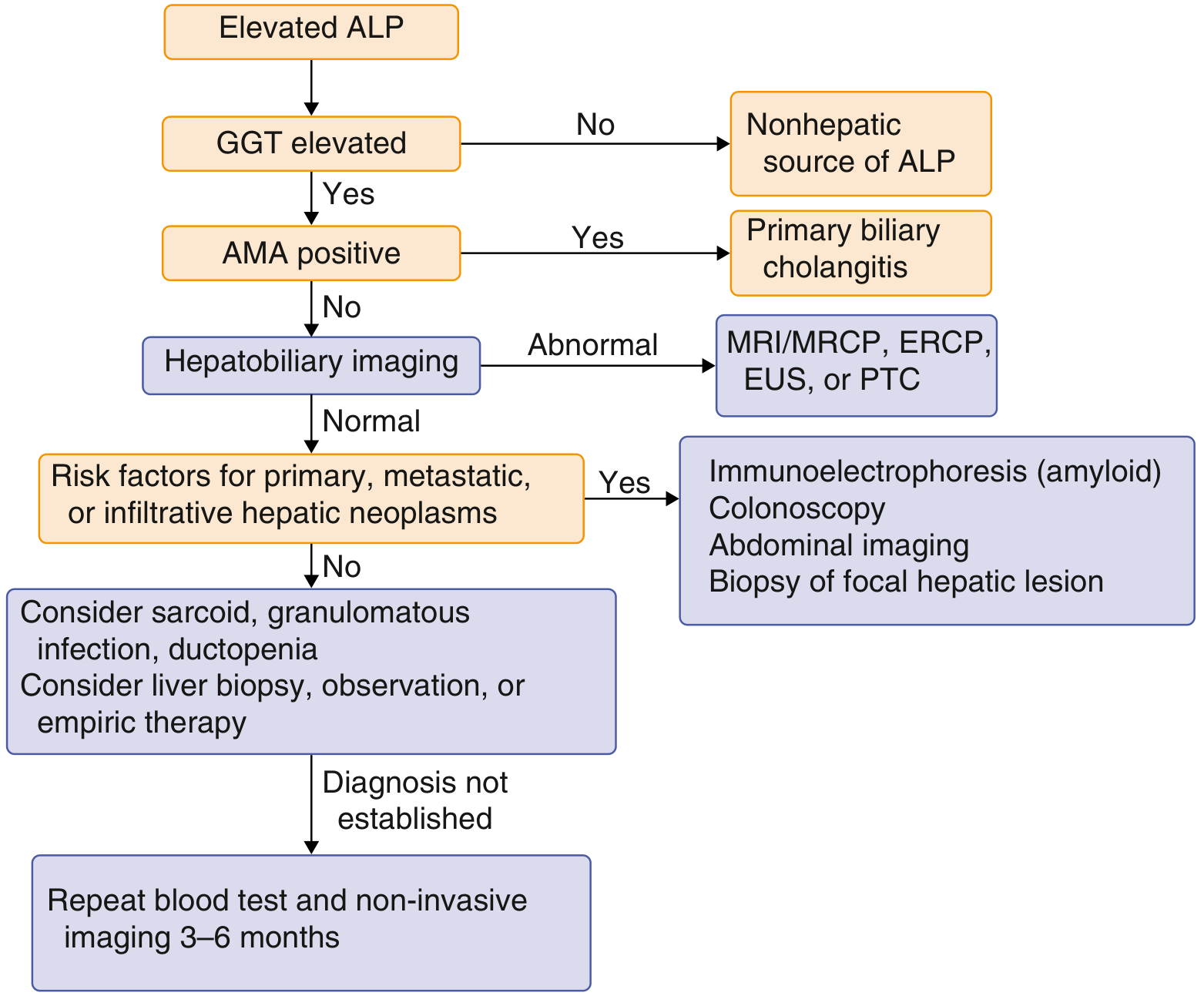
6. Clinical Approach to Elevated ALP
When ALP is isolated (aminotransferases normal or minimally elevated), the key question is: hepatic vs. non-hepatic origin?
Step 1: Check GGT (gamma-glutamyl transferase) or 5'-nucleotidase (5'-NT):
- If GGT/5'-NT is also elevated → hepatobiliary source likely
- If GGT/5'-NT is normal → bone or other non-hepatic source
Step 2 (if hepatobiliary):
- Check antimitochondrial antibody (AMA): positive = primary biliary cholangitis
- Liver ultrasound as first imaging step
- If biliary dilation or suspicious lesion: MRCP, ERCP, or EUS
- Consider liver biopsy if etiology unclear
7. Differentiating ALP Isoenzymes in the Lab
When electrophoresis is unavailable, two adjunctive tests are used:
| Test | Hepatic ALP | Bone ALP |
|---|---|---|
| GGT | Elevated | Normal |
| 5'-Nucleotidase | Elevated | Normal |
| Heat stability | 50% inactivated | 90% inactivated |
The use of isoenzyme fractionation has largely been supplanted by GGT and 5'-NT in routine practice.
8. Clinical Significance - High-Yield Points for PG
- Cholestatic pattern on LFT: ALP + GGT elevated disproportionately vs. transaminases = obstructive/cholestatic pathology
- ALP most sensitive for hepatic metastases - more than ALT/AST
- Wilson disease = low ALP + jaundice + Coombs-negative hemolysis = classic triad (ALP displaced by copper)
- Paget disease = markedly elevated bone ALP with normal GGT
- Hypophosphatasia = low ALP + rickets-like picture in children
- Regan isoenzyme = ectopic ALP in malignancy
- Isolated ALP elevation in pregnancy = normal (placental origin, third trimester)
- Bone ALP as a biomarker = used in monitoring treatment response in Paget disease and bone metastases
Summary Table
| ALP elevated | ALP decreased |
|---|---|
| Obstructive jaundice | Hypophosphatasia |
| PBC / PSC | Wilson disease (ALF) |
| Hepatic metastases | Malnutrition / Zinc deficiency |
| Paget disease | Hypothyroidism |
| Healing fractures | Hemolysis (artifactual) |
| Rickets / Osteomalacia | Estrogen therapy |
| Pregnancy (placental) | |
| Malignancy (Regan isoenzyme) |
Sources:
- Quick Compendium of Clinical Pathology, 5th ed. (p. 4, isoenzyme table and LFTs section)
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease (p. 1394-1395, ALP physiology)
- Goldman-Cecil Medicine, International Ed. (p. 1562, approach to elevated ALP)
- Henry's Clinical Diagnosis and Management by Laboratory Methods (ALP measurement and interferences)
Generate answer in Orthopaedic Post graduate exam point of view
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have all the data needed for a focused orthopaedic PG answer. Here it is:
Alkaline Phosphatase (ALP) - Orthopaedic PG Exam Answer (10 Marks)
1. Introduction
Alkaline phosphatase (ALP) is a zinc-dependent membrane-bound ectoenzyme that hydrolyzes phosphate monoesters under alkaline conditions (optimum pH ~9). From an orthopaedic standpoint, bone ALP is the most clinically relevant isoenzyme, produced by osteoblasts during active bone formation and mineralization.
- Normal adult serum ALP: ~30-120 IU/L
- Half-life in serum: ~40-48 hours (bone ALP); ~7 days (total ALP)
2. Biochemical Role in Bone - The Orthopaedic Core
Bone ALP (tissue-nonspecific ALP, encoded by the ALPL gene on chromosome 1) is attached to the osteoblast membrane via a glycosylphosphatidylinositol (GPI) anchor. Its primary role is in bone mineralization:
- Hydrolyzes inorganic pyrophosphate (PPi) → inorganic phosphate (Pi)
- PPi is a potent inhibitor of hydroxyapatite crystal formation
- By destroying PPi, bone ALP removes this inhibition and promotes hydroxyapatite deposition
- Matrix vesicles budding from osteoblasts are markedly enriched in bone ALP
Key concept: Bone ALP = marker of osteoblast number and activity = marker of BONE FORMATION (not resorption)
(Source: Tietz Textbook of Laboratory Medicine, 7th ed., p. 2186)
3. ALP as a Bone Turnover Marker
In orthopaedics, ALP is classified alongside other bone formation markers:
| Marker Type | Test | Correlates With |
|---|---|---|
| Bone Formation | Total ALP | Osteoblast numbers, liver/kidney disease |
| Bone Formation | Bone-specific ALP (BALP) | Osteoblast numbers (more specific) |
| Bone Formation | Osteocalcin | Osteoblast numbers |
| Bone Formation | PINP, PICP | Type I collagen synthesis |
| Bone Resorption | CTX, NTX | Bone collagen degradation |
| Bone Resorption | TRAP | Osteoclast numbers |
| Bone Resorption | Deoxypyridinoline | Bone collagen degradation |
(Source: Rockwood and Green's Fractures in Adults, 10th ed., Table 4-2)
4. Orthopaedic Conditions - ALP Levels with Calcium/Phosphorus Profile
This is the most exam-critical table for orthopaedic surgery PGs:
| Disorder | Serum Calcium | Serum Phosphorus | Serum ALP | Urine |
|---|---|---|---|---|
| Osteoporosis | Normal | Normal | Normal | Normal Ca |
| Osteomalacia / Rickets | Low/Normal | Low | HIGH | Low Ca |
| Hyperparathyroidism | Normal-High | Normal-Low | Normal-High | High Ca |
| Renal Osteodystrophy | Low | High | High | - |
| Paget Disease | Normal | Normal | Very HIGH | ↑Hydroxyproline |
| Multiple Myeloma | Normal | Normal | Normal | Bence-Jones protein |
(Source: Rockwood and Green's Fractures in Adults, 10th ed., Table 25-5)
5. Disease-Specific Orthopaedic Relevance
A. Paget Disease of Bone (Highest Yield)
- ALP is the single most sensitive and specific marker for diagnosis and monitoring of Paget disease
- ALP reflects the markedly increased osteoblastic bone formation in Paget's
- Extent of elevation correlates with the extent of skeletal involvement (highest when skull is involved)
- In current Paget disease, ALP is typically 2-4x ULN (previously 10x ULN - milder phenotype now seen)
- Bone-specific ALP is more sensitive than total ALP in mild/monostotic disease
- ALP along with urine pyridinium cross-links is used to monitor disease activity
- With bisphosphonate treatment, ALP normalizes - used to monitor treatment response
- Serum and urine calcium are usually normal; may rise with immobilization (e.g., post-fracture)
- Complication: ~1% develop secondary osteosarcoma (higher in polyostotic disease)
(Source: Campbell's Operative Orthopaedics 15th ed.; Tietz Textbook of Laboratory Medicine)
B. Rickets and Osteomalacia
- Elevated ALP with low calcium and low phosphorus is classic
- In severe osteomalacia, bone ALP may be markedly raised without increased bone mineralization (due to mineralization defect)
- ALP elevation is due to compensatory osteoblastic hyperactivity
- Familial hypophosphatemic rickets (X-linked dominant, FGF23 mutation): low phosphorus, normal calcium, high ALP - treatment with burosumab (anti-FGF23 monoclonal antibody)
C. Hyperparathyroidism / Brown Tumors
- ALP, calcium, phosphorus, and PTH levels are used to diagnose hyperparathyroidism and differentiate "brown tumors" from giant cell tumors
- In hyperparathyroidism: high Ca, low PO4, elevated ALP, high PTH
- Orthopaedic management = treating actual or impending pathologic fractures
D. Renal Osteodystrophy
- Low calcium, high phosphorus, elevated ALP (due to secondary hyperparathyroidism)
- Bone-specific ALP is useful here because it is not cleared by glomerular filtration (unlike osteocalcin) - preferred marker in renal failure patients
E. Bone Metastases
- ALP is elevated in osteoblastic metastases (e.g., from prostate cancer) reflecting osteoblastic reaction
- ALP is the most sensitive hepatic chemistry analyte for hepatic metastases
- ALP may be normal in purely osteolytic lesions (e.g., multiple myeloma - important distinction)
F. Osteosarcoma
- ALP levels may be elevated in osteosarcoma
- Elevated pre-treatment ALP is associated with worse prognosis
- Post-chemotherapy normalization of ALP indicates good tumor response
- ALP is not a specific tumor marker but is a useful prognostic indicator
G. Fracture Healing
- ALP rises transiently during fracture healing, reflecting osteoblastic callus formation
- Peak at ~2-3 weeks post-fracture; returns to normal once consolidation is complete
- Persistent ALP elevation beyond expected time = non-union or ongoing metabolic bone disease
6. Hypophosphatasia - Low ALP (Critical Orthopaedic Condition)
- Autosomal recessive inborn error of metabolism
- Loss-of-function mutation in ALPL gene (tissue-nonspecific ALP)
- Results in low serum ALP - unable to break down PPi, so PPi accumulates and inhibits mineralization
- Features mimic rickets: bone pain, fractures, deformity, premature tooth loss
- Diagnostic marker: elevated urinary phosphoethanolamine (PEA) - pathognomonic
- Elevated plasma pyridoxal 5'-phosphate (PLP) - another substrate that accumulates
- Treatment: Asfotase alfa (recombinant TNSALP enzyme replacement - now approved)
- Bisphosphonates are contraindicated in hypophosphatasia (they further inhibit mineralization)
(Source: Miller's Review of Orthopaedics 9th ed.; Tietz Textbook of Laboratory Medicine)
7. Monitoring Treatment with ALP
| Condition | Treatment | ALP Response |
|---|---|---|
| Paget disease | Bisphosphonates (zoledronate) | Normalization = adequate disease control |
| Rickets/Osteomalacia | Vitamin D + Calcium | ALP falls as mineralization improves |
| Hyperparathyroidism | Parathyroidectomy | ALP may transiently rise (hungry bone syndrome), then normalize |
| Renal osteodystrophy | Dialysis, phosphate binders, Vit D | Bone ALP used to guide therapy |
| Osteosarcoma | Neoadjuvant chemotherapy | Normalization = good histological response |
8. Key Exam Points - High-Yield Summary
- Bone ALP = osteoblast marker = bone formation marker (NOT resorption)
- Paget disease = highest ALP elevation of all metabolic bone diseases
- Myeloma = normal ALP despite widespread bone disease (osteolytic, no osteoblastic reaction)
- Hypophosphatasia = LOW ALP + rickets-like picture - bisphosphonates contraindicated
- Wilson disease = LOW ALP + jaundice + hemolysis (copper displaces zinc cofactor)
- Bone-specific ALP preferred in renal failure (not filtered by kidney, unlike osteocalcin)
- Bisphosphonate treatment response in Paget's is monitored by serial ALP levels
- Elevated pre-treatment ALP in osteosarcoma = poor prognosis
- Hungry bone syndrome post-parathyroidectomy: ALP may transiently spike as osteoblasts become hyperactive
- Physiologic elevation: ALP is 2x adult levels in growing children (bone growth) and in third-trimester pregnancy (placental isoenzyme) - NOT pathological
Sources:
- Rockwood and Green's Fractures in Adults, 10th ed. (2025) - Bone turnover marker table; metabolic bone disease lab values
- Campbell's Operative Orthopaedics, 15th ed. (2026) - Paget disease management and monitoring
- Miller's Review of Orthopaedics, 9th ed. - Metabolic bone disease table; hypophosphatasia
- Tietz Textbook of Laboratory Medicine, 7th ed. - Bone ALP biochemistry, role in mineralization, Paget disease monitoring
- Firestein & Kelley's Textbook of Rheumatology, 2-Volume Set - Bone turnover markers; Paget disease treatment
Create pdf
Reading File
Running Command
Running Command
Writing File
Running Command
Running Command
Your PDF is ready! Here's the download link:
Alkaline Phosphatase Ortho PG
PDF Document · PDF
What's inside the PDF:
| Section | Content |
|---|---|
| 1 | Introduction - biochemistry, normal values, gene |
| 2 | Role in bone mineralization (PPi → Pi pathway) |
| 3 | ALP as a bone turnover marker - full classification table |
| 4 | Metabolic bone disease lab profile table (Ca / PO4 / ALP) - most exam-critical |
| 5 | Disease-specific sections: Paget, Rickets, HPT, Renal osteodystrophy, Metastases, Osteosarcoma, Fracture healing |
| 6 | Hypophosphatasia - low ALP, contraindication of bisphosphonates |
| 7 | Monitoring treatment with ALP |
| 8 | 10 High-Yield exam points (highlighted table) |
| 9 | Isoenzymes heat stability table |
Formatted with navy/teal color scheme, clean tables, and exam-ready layout.
Unable to download pdf gile
Running Command
Running Command
Try this direct path link:
ALP Ortho PG
PDF Document · PDF
If that still doesn't work, here are 3 alternative ways to get the file:
Option 1 - Try the original path directly:
/home/daytona/workspace/alp-ortho/Alkaline_Phosphatase_Ortho_PG.pdfOption 2 - Right-click the link above and choose "Save link as" or "Download linked file"
Option 3 - I can convert the full answer into a Word document (.docx) instead, which may download more reliably in your interface. Just say "Create Word doc" and I'll generate it.
Option 4 - I can share the content as a formatted HTML page that you can print-to-PDF from your browser.
Which would you prefer?
Create a Word document (.docx) instead
Reading File
Writing File
Running Command
Running Command
Running Command
The file is valid (18 KB, proper .docx structure with valid XML). Here's the download link:
ALP Ortho PG Exam
Word Document · DOCX
What's in the Word document:
- Navy/teal professional formatting with color-coded tables
- 9 sections covering all orthopaedic-relevant ALP content
- The critical metabolic bone disease lab profile table (Ca / PO4 / ALP) with color highlights
- Hypophosphatasia row in red with bisphosphonate contraindication warning
- High-yield 10-point exam summary in a dark navy table with gold numbering
- Header with document title and footer with page numbers on every page
- All 7 textbook references cited at the end
This is a shared conversation. Sign in to Orris to start your own chat.