Normal tension glaucoma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"normal tension glaucoma" pathophysiology management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Normal Tension Glaucoma (NTG)
Definition
Normal tension glaucoma (NTG) - also called low-tension glaucoma or normal-pressure glaucoma - is a form of primary open-angle glaucoma (POAG) in which characteristic optic nerve damage and visual field loss occur despite intraocular pressure (IOP) consistently at or below 21 mmHg. It is defined by:
- IOP consistently ≤ 21 mmHg on diurnal testing
- Open anterior chamber angle on gonioscopy
- Characteristic glaucomatous optic nerve cupping
- Visual field defects consistent with nerve appearance
- No features of secondary glaucoma or a non-glaucomatous cause
Depending on ethnic background, 30-65% of all open-angle glaucoma patients may have IOP within the normal range at initial assessment. NTG is especially prevalent in Japanese patients.
- Kanski's Clinical Ophthalmology, 10th ed., p. 386
Pathogenesis
The mechanisms underlying NTG are multifactorial and not fully resolved. While IOP still plays a role, IOP-independent mechanisms are relatively more important than in POAG:
| Mechanism | Details |
|---|---|
| Vascular dysregulation | Vasospasm, nocturnal hypotension, loss of autoregulation; associated with migraine and Raynaud phenomenon |
| Reduced ocular perfusion pressure | Relatively lower than in POAG |
| Lamina cribrosa | Larger translaminar pressure gradient; structural vulnerability may predispose to damage at normal IOP |
| Low CCT | Thin corneas cause IOP underestimation; corneas are thinner in NTG than POAG |
| Accelerated apoptosis | Retinal ganglion cell loss via non-mechanical pathways |
| Autoimmune factors | Higher autoantibody levels in some NTG groups |
| Nocturnal IOP spikes | A small proportion have marked nocturnal IOP elevation detectable only in the supine position |
From Robbins: "...visual field and optic nerve changes typical of glaucoma develop with normal intraocular pressure...there is a spectrum of neuronal susceptibility to the effects of elevated intraocular pressure."
- Robbins Pathologic Basis of Disease, p. 1223
Risk Factors
- Age - tends to be older than POAG patients (may reflect delayed diagnosis)
- Sex - higher prevalence in females in some studies
- Race - significantly more common in Japanese individuals
- Family history - OPTN gene (optineurin) mutations identified in some NTG cases
- Low CCT - thinner corneas than POAG
- Vascular conditions - migraine, Raynaud phenomenon, diabetes, carotid insufficiency, hypercoagulability
- Systemic hypotension - nocturnal BP dips >20% are particularly important; beta-blockers taken at bedtime may worsen this
- Obstructive sleep apnoea - impairs ocular perfusion
- Myopia - associated with glaucoma and progression
- Thyroid disease - may be more common
- Low serum retinol
- Autoantibodies
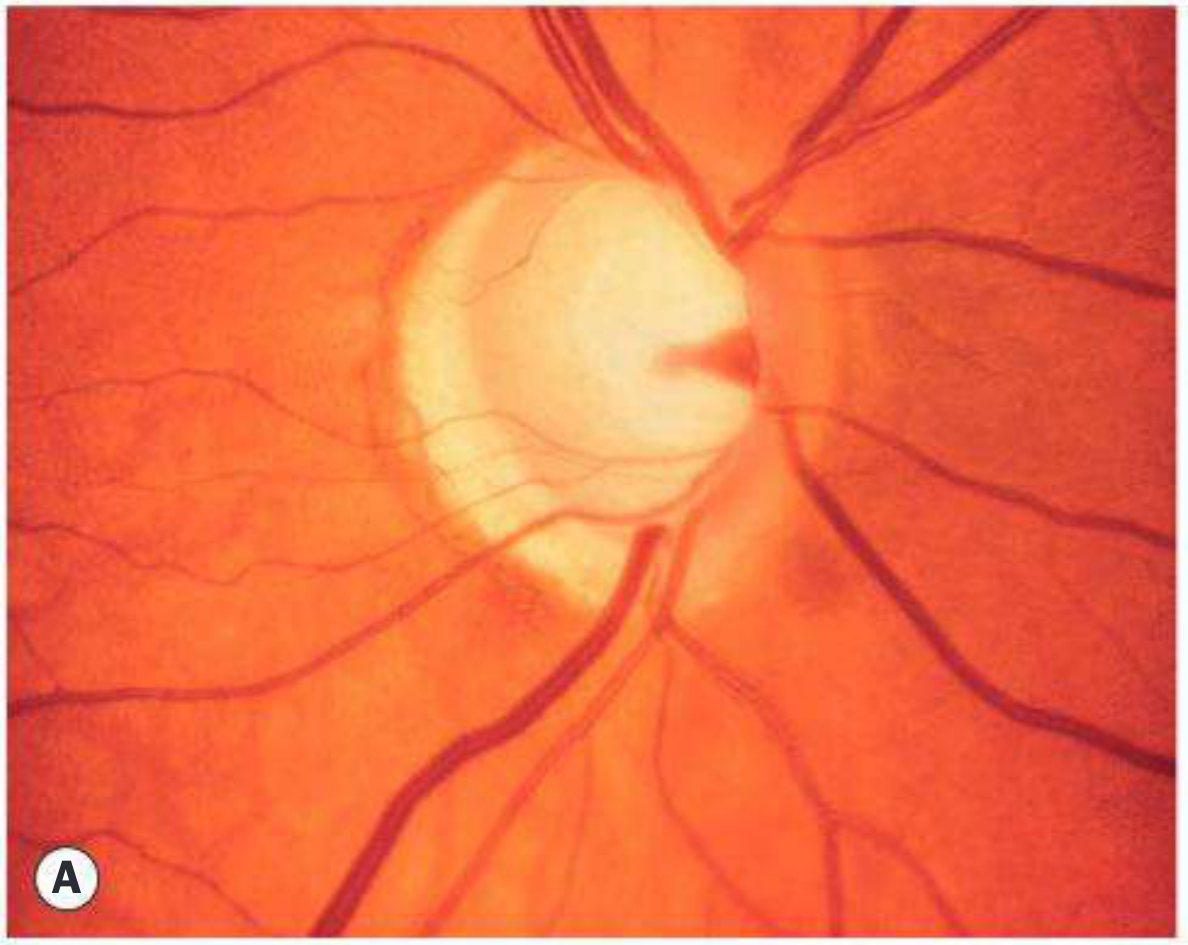
Clinical Features
Optic Nerve Head (distinctive features vs POAG):
- Optic nerve head tends to be larger on average
- Acquired optic disc pits and focal nerve fibre layer defects are more common
- Splinter haemorrhages on the disc margin are more frequent - they are associated with a greater likelihood of progression and are often missed without disc photography
- Peripapillary atrophic changes may be more prevalent
- Pallor disproportionate to cupping should raise suspicion of an alternative (non-glaucomatous) diagnosis
Visual Field Defects:
-
Denser, more localised, and closer to fixation than in POAG
-
A dense nasal paracentral defect is typical
-
Same pattern types as POAG (arcuate, etc.) but with above features
-
Wills Eye Manual, p. 561
Differential Diagnosis
Before accepting an NTG diagnosis, the following must be excluded:
- Angle closure - rule out by dark-room gonioscopy
- Low CCT causing spuriously low IOP readings (post-refractive surgery, corneal ectasia)
- POAG with wide diurnal IOP fluctuation - diurnal phasing required; nocturnal spikes require home monitoring or in-patient assessment
- Previous masking by systemic beta-blockers started after glaucomatous damage
- Spontaneously resolved glaucoma (pigmentary, traumatic, steroid-induced)
- Shock-related optic neuropathy - from acute blood loss, MI, bypass surgery; visual loss should not progress
- Neurological compressive lesions - optic nerve/chiasmal compression (neuroimaging mandatory if visual fields suggest non-glaucomatous pattern, if colour vision is disturbed, or in young patients)
- AION (arteritic or non-arteritic) - may mimic NTG exactly; check ESR/CRP if GCA suspected
- Other optic neuropathies - inflammatory, infiltrative, drug-induced (e.g., ethambutol), Leber hereditary optic neuropathy, dominant optic atrophy
Workup
History:
- Vasospasm (migraine, Raynaud), hypotensive episodes (surgery, haemorrhage), prior steroid use, ocular trauma/uveitis, GCA symptoms, cardiovascular risk factors
Investigations:
- Repeat IOP - diurnal curve (phasing); consider supine IOP
- Gonioscopy - rule out angle closure, angle recession, PAS
- Visual fields (perimetry at 6-monthly intervals initially)
- OCT - RNFL thinning (thinner in NTG)
- Colour plates (Ishihara/HRR) - rule out optic neuropathy
- Blood pressure monitoring - 24-hour ambulatory BP; look for nocturnal dipping
- Carotid Dopplers - assess ocular blood flow
- CT or MRI - to exclude compressive lesions, especially if visual acuity reduced, colour vision affected, or fields suggest non-glaucomatous pattern
- FBC, ESR, CRP (if GCA or inflammatory cause suspected)
- Lipid profile, glucose, thrombophilia screen if vascular risk suspected
Treatment
The Collaborative Normal Tension Glaucoma Study (CNTGS)
The landmark CNTGS established that IOP lowering by at least 30% reduced the 5-year risk of visual field progression from 35% to 12% in untreated patients. However, approximately 50% of untreated patients do not deteriorate at 5-7 years, so treatment should be targeted at those at highest risk.
Indications to treat:
- Demonstrated progression on serial perimetry
- Advanced glaucomatous damage, especially if central vision is threatened
- Long life expectancy
- Disc haemorrhages (marker of higher progression risk)
Medical Treatment
| Agent | Notes |
|---|---|
| Prostaglandin analogues (latanoprost, bimatoprost) | First-line IOP-lowering agents |
| Brimonidine | IOP lowering + potential neuroprotective effect; preferred over beta-blockers in NTG |
| Beta-blockers | Use with caution - systemic absorption can worsen nocturnal BP dip; if used, betaxolol is preferred (cardioselective) |
| Selective laser trabeculoplasty (SLT) | Reasonable initial option |
Surgical Treatment
- Consider if progression occurs despite IOP in the low teens
- Trabeculectomy with antimetabolite (MMC or 5-FU) is usually required to achieve sufficiently low target pressure
Non-IOP-Directed Measures
- Systemic vascular control - optimise management of diabetes, hypertension, hyperlipidaemia
- Nocturnal BP dips - reduce antihypertensive dose (especially bedtime dosing); consider increased salt intake (in consultation with cardiologist)
- Calcium-channel blockers (e.g., nimodipine) - for vasospasm; advocated by some authorities
- Head-up sleeping position (30°) - mean IOP is ~20% lower than flat position; beneficial in at least one-third of patients
- Regular exercise - encouraged
- Avoid head-stand yoga - transiently raises IOP
- Ginkgo biloba (40 mg TID) - may confer some benefit in selected cases
- Neuroprotection - no agent of proven benefit yet; memantine showed no benefit in clinical trials
Prognosis & Progression
- Approximately 50% of untreated patients remain stable at 5-7 years
- Progression is more likely with: disc haemorrhages, female sex, lower IOP at baseline (paradoxically), migraine, myopia, and nocturnal hypotension
- The EMGT confirms low blood pressure as an independent risk factor for progression
- Splinter haemorrhages are the strongest clinical marker of ongoing progression
Recent Evidence (PubMed, 2025)
- A 2025 Cochrane systematic review (PMID 41370133) on prognostic factors in open-angle glaucoma progression confirms that low perfusion pressure, disc haemorrhages, and thin RNFL are the strongest predictors of progression.
- A 2025 meta-analysis (PMID 40340860) found that microinvasive glaucoma surgery (MIGS), alone or combined with phacoemulsification, is effective at achieving IOP reduction in NTG patients.
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., pp. 385-388
- Wills Eye Manual, Office and Emergency Room Diagnosis, pp. 561-562
- Robbins & Cotran Pathologic Basis of Disease, p. 1223
This is a shared conversation. Sign in to Orris to start your own chat.