How to correct Hyponatremia
Reading File
Finding Sources
Searching PubMed
"hyponatremia" AND "treatment"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Here is the full, structured guide to correcting hyponatremia:
Correction of Hyponatremia
Hyponatremia is defined as serum [Na⁺] < 135 mEq/L. Treatment depends on three axes: symptom severity, acuity (acute vs. chronic), and volume status.
Step 1 - Classify by Volume Status
| Type | Clinical Features | Urine Na⁺ | Key Cause |
|---|---|---|---|
| Hypovolemic | Tachycardia, dry mucosa, orthostasis | <20 mEq/L (non-renal) or >20 (renal) | GI losses, diuretics |
| Euvolemic (normovolemic) | No edema, normal skin turgor | >20 mEq/L | SIADH, hypothyroidism, adrenal insufficiency |
| Hypervolemic | JVD, peripheral edema, pulmonary congestion | <20 mEq/L | Heart failure, cirrhosis, CKD |
Step 2 - Assess Urgency (Symptoms + Acuity)
Two groups require immediate treatment:
- Severe symptomatic hyponatremia - seizures, coma, obtundation, brainstem herniation (regardless of sodium level)
- Severe asymptomatic hyponatremia - serum Na⁺ ≤ 110 mEq/L
Symptoms worsen with falling Na⁺ and with acuity of onset. Acute hyponatremia (< 24-48 hours) carries higher risk of cerebral edema; chronic hyponatremia (> 48 hours) carries higher risk of osmotic demyelination syndrome (ODS) if corrected too fast.
Step 3 - Correction Rates (The Most Critical Part)
Overly rapid correction causes Osmotic Demyelination Syndrome (ODS) - previously called central pontine myelinolysis - presenting with flaccid paralysis, dysarthria, dysphagia, and hypotension. It is most common in alcoholics, malnourished patients, and the elderly.
Safe Correction Targets
| Scenario | Target Rate |
|---|---|
| Acute symptomatic (true acute <24-48 h) | Raise by 4-6 mmol/L urgently; no upper daily limit if truly acute |
| Chronic / unknown duration - normal ODS risk | ≤ 10-12 mmol/L in 24 h, ≤ 18 mmol/L in 48 h |
| Chronic - HIGH ODS risk (Na⁺ <120 with >48 h duration, thiazide-induced, alcoholism, malnutrition) | ≤ 8 mmol/L in 24 h; aim 4-6 mmol/L/day |
| Asymptomatic | ≤ 0.5 mEq/L per hour, max 12 mEq/L/day |
- Goldman-Cecil Medicine, p. 1202-1203; Schwartz's Surgery, p. 122
Step 4 - Treatment by Clinical Scenario
A. Acute Symptomatic Hyponatremia (Seizures / Coma)
3% Hypertonic Saline is the treatment of choice.
- Bolus protocol (preferred - less risk of overcorrection than continuous infusion): Give 100 mL of 3% NaCl IV over 10 minutes, repeat up to twice as needed
- Goal: raise serum Na⁺ by 4-6 mmol/L - this is usually enough to stop seizures and reduce cerebral edema
- For mild-to-moderate symptoms with low herniation risk: infuse 3% NaCl at 0.5-2 mL/kg/hour
- Monitor serum Na⁺ every 1-2 hours
- Goldman-Cecil Medicine, p. 1203; Rosen's Emergency Medicine, p. 2521
B. Chronic Hyponatremia - Euvolemic (SIADH)
- Free water restriction - first-line; restrict oral intake to 500 mL/day below 24-hour urine output
- May be insufficient if urine osmolality > 500 mOsm/kg, urine (Na⁺ + K⁺) > serum Na⁺, or 24-h urine < 1500 mL/day
- Tolvaptan (Vaptan) - oral AVP V2-receptor antagonist; start at 15 mg once daily, max 60 mg once daily
- Indicated in hospitalized patients with SIADH refractory to fluid restriction
- Monitor Na⁺ every 6-8 hours for first 24-48 h; allow free fluid intake (avoid simultaneous fluid restriction - risk of overcorrection)
- NOT for cirrhosis (hepatotoxicity risk); NOT for hypovolemic hyponatremia
- Urea (SIADH-specific) - 15-90 g/day divided in 2-3 doses; promotes urinary free water excretion; well-tolerated for chronic use
- Demeclocycline - 600-1200 mg/day; alternative for refractory SIADH
- Treat underlying cause - discontinue offending drug, treat hypothyroidism or adrenal insufficiency
For severe symptomatic SIADH or Na⁺ < 120 mmol/L: use 3% NaCl (more reliable than vaptans for urgent correction).
- Goldman-Cecil Medicine, p. 1203-1204; Rosen's Emergency Medicine, p. 2522
Note: In SIADH, isotonic normal saline can paradoxically worsen hyponatremia because the kidneys excrete the sodium while retaining the free water (hypertonic urine).
C. Hypovolemic Hyponatremia
- Isotonic normal saline (0.9% NaCl) is the treatment of choice
- Hypotensive patients: resuscitate with NS at 500-1000 mL/hr until BP stabilized, then slow to ~200 mL/hr with frequent Na⁺ checks
- As volume is restored, ADH levels fall and free water diuresis begins - this can cause rapid overcorrection; monitor urine output and osmolality hourly and be ready to switch to hypotonic solutions or DDAVP if correction becomes too fast
- If Na⁺ < 120 mEq/L, keep rise ≤ 0.5 mEq/hr or ~8 mEq/day until Na⁺ reaches ~120
D. Hypervolemic Hyponatremia (Heart Failure, Cirrhosis, CKD)
- Fluid and sodium restriction - primary approach
- Loop diuretics (furosemide) - increase water excretion
- Heart failure: diuretics that also cause vasodilation to improve cardiac output
- Cirrhosis: albumin + diuretics ± paracentesis; tolvaptan is contraindicated (hepatotoxicity)
- Renal failure with volume overload: hemodialysis (monitor closely to avoid rapid Na⁺ correction)
- Avoid hypertonic saline in hypervolemic patients (risk of pulmonary edema)
E. Mild-to-Moderate Asymptomatic Hyponatremia (Na⁺ 115-135 mEq/L)
- Free water restriction is typically the most important intervention
- Identify and treat the underlying cause
- Raise Na⁺ at ≤ 0.5 mEq/L/hour, max 12 mEq/L/day
Step 5 - If Overcorrection Occurs
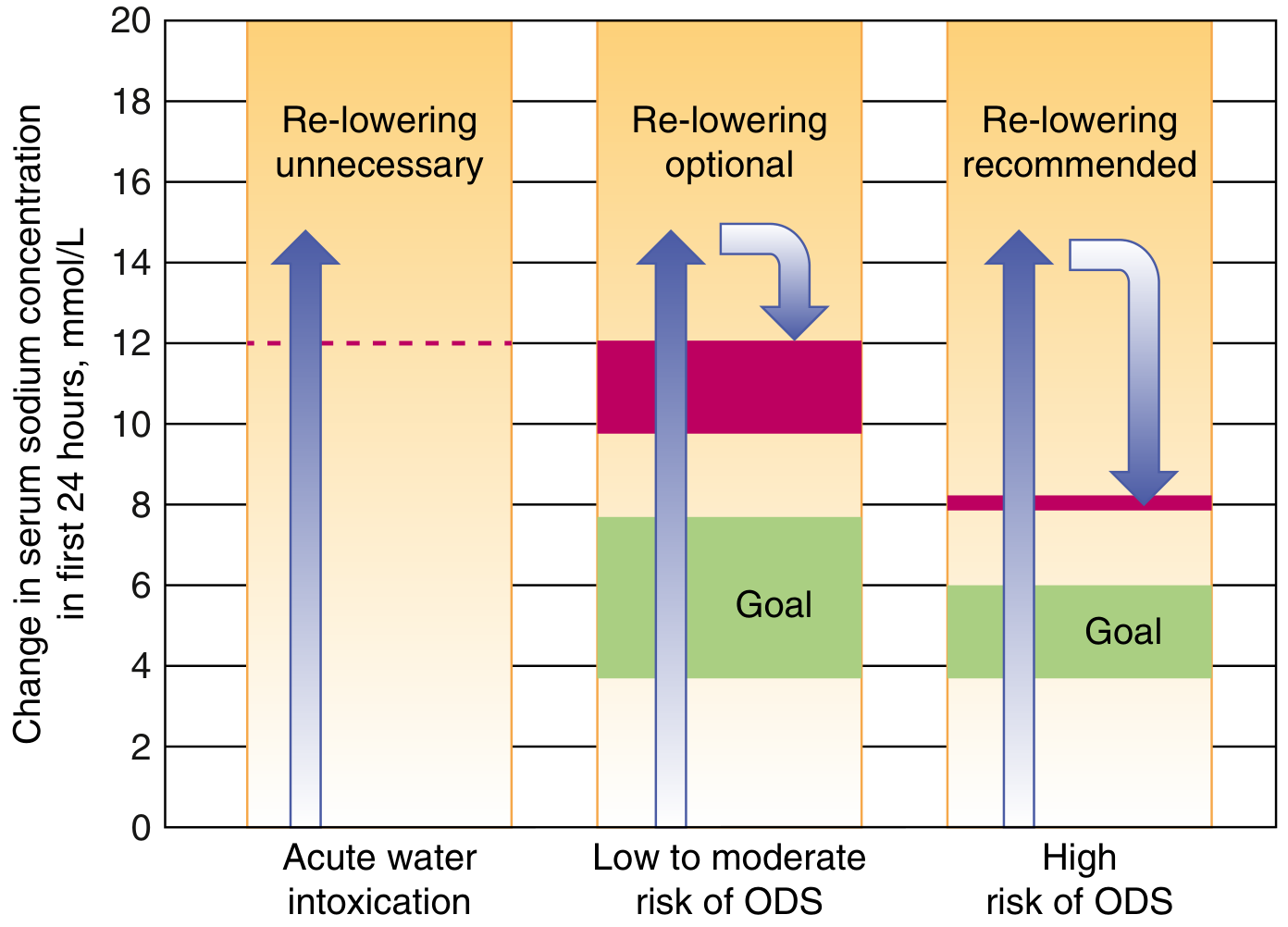
Chart: Recommendations for re-lowering serum [Na⁺] when correction limits are exceeded - Goldman-Cecil Medicine, p. 1203
If correction exceeds safe limits and starting Na⁺ was < 120 mmol/L:
- Stop all sodium-containing fluids immediately
- Administer desmopressin (DDAVP) 2-4 mcg IV every 8 hours to prevent further free water loss
- Infuse 5% dextrose in water (D5W) at 3 mL/kg/hour to re-lower Na⁺ back to target
- Consider high-dose dexamethasone 4 mg IV every 6 hours for 24-48 hours if significant overcorrection occurred
- Monitor Na⁺ hourly until at goal
- If starting Na⁺ was ≥ 120 mmol/L, re-lowering is generally not needed
Useful Formula - Adrogue-Madias Equation
To estimate the effect of 1 liter of any infusate on serum Na⁺:
ΔNa⁺ = (Infusate Na⁺ - Serum Na⁺) / (TBW + 1)
Where TBW = 0.6 × weight (kg) in males; 0.5 × weight in females.
| Infusate | Na⁺ Content |
|---|---|
| 3% NaCl (hypertonic saline) | 513 mEq/L |
| 0.9% Normal saline | 154 mEq/L |
| Lactated Ringer's | 130 mEq/L |
| 0.45% Half-normal saline | 77 mEq/L |
| D5W | 0 mEq/L |
- Rosen's Emergency Medicine, p. 2521
Potassium Replacement
Potassium deficits must be corrected aggressively alongside hyponatremia, as potassium replacement itself raises serum Na⁺ (it shifts into cells in exchange for Na⁺). Failure to account for this can cause inadvertent overcorrection.
Recent Evidence
A 2025 systematic review and meta-analysis in JAMA Internal Medicine (PMID 39556338) examined correction rates and clinical outcomes in hospitalized adults with severe hyponatremia, providing updated data on optimal correction targets. A separate 2025 meta-analysis in American Journal of Kidney Diseases (PMID 39362395) confirmed that urea is effective and safe for treating SIADH-related hyponatremia, supporting its use as an alternative when fluid restriction or vaptans are insufficient.
Sources: Goldman-Cecil Medicine, pp. 1202-1204 | Rosen's Emergency Medicine, pp. 2521-2522 | Schwartz's Principles of Surgery, p. 122 | Brenner and Rector's The Kidney
This is a shared conversation. Sign in to Orris to start your own chat.