I now have all the information needed to compile a thorough, teacher-ready presentation. Let me write the full detailed response.
FULL CLINICAL PRESENTATION: CERVICAL SPONDYLOSIS WITH REFERRED SHOULDER PAIN
Patient Profile
Name: Urmila | Age: 70 years | Gender: Female | Occupation: Housewife
SECTION 1 - PROVISIONAL DIAGNOSIS
Cervical Spondylosis (Discogenic Neck Pain / Cervical Facet Arthropathy with referred shoulder pain)
Possibly with a secondary component of Periarthritis Shoulder (Adhesive Capsulitis - early stage) given the shoulder involvement and rest pain - this combination is common in elderly women.
SECTION 2 - DEFINITION
Cervical Spondylosis is a degenerative condition of the cervical spine characterized by chronic disc degeneration and associated facet joint arthropathy (osteoarthritis of the facet joints, uncovertebral joints, and intervertebral discs). It is essentially "wear and tear" arthritis of the neck.
As people age, the intervertebral discs lose water content and height, the annulus fibrosus weakens, osteophytes (bony spurs) form at vertebral margins, and the facet joints undergo arthritic changes. This produces the classic cervical spondylosis picture.
- Miller's Review of Orthopaedics, 9th Ed. defines it as: "chronic disc degeneration and associated facet arthropathy" that can result in four clinical entities: discogenic neck pain, radiculopathy, myelopathy, or myeloradiculopathy.
SECTION 3 - ANATOMY INVOLVED
The cervical spine has 7 vertebrae (C1-C7). Each motion segment consists of:
- Intervertebral disc (nucleus pulposus + annulus fibrosus)
- Two facet (zygapophyseal) joints posteriorly - these have sensory receptors that contribute to pain and proprioception
- Two uncovertebral joints of Luschka (unique to cervical spine, C3-C7)
- Neural foramina through which nerve roots exit
Levels most commonly involved: C5-C6 (most frequent), followed by C6-C7.
In Urmila's case, facet arthropathy is likely causing referred pain in the shoulder (sclerotomal referral), because facet joint capsules are densely innervated and refer pain to specific sclerotomes - the shoulder is a classic referral zone for C4-C5-C6 facet pathology.
SECTION 4 - EPIDEMIOLOGY
- Peaks between 40 and 50 years, but remains prevalent in older age (70 years like Urmila is very common)
- Women are slightly more affected in older age groups
- Cervical osteoarthritis and spondylosis are described as "ubiquitous with increasing age" - Bradley and Daroff's Neurology in Clinical Practice
- A 70-year-old housewife is a very typical patient - repetitive household activities, forward head posture, and age-related degeneration all contribute
SECTION 5 - PATHOPHYSIOLOGY (Degenerative Cascade)
The pathological changes follow a degenerative cascade (first described by Kirkaldy-Willis in the 1970s):
Stage 1 - Disc Degeneration:
- Nucleus pulposus loses hydration and proteoglycan content
- Disc height decreases
- Annulus fibrosus develops circumferential cracks and radial tears
Stage 2 - Joint Instability:
- Loss of disc height loads the facet joints and uncovertebral joints abnormally
- Facet joint capsule stretches, causing segmental instability
- Micromotion at these joints triggers inflammatory response
Stage 3 - Stabilization / Osteophyte Formation:
- Body responds by forming osteophytes (bony spurs) at disc margins and facet joints
- Progressive loss of cervical lordosis
- Osteophytes can encroach on neural foramina or the spinal canal
In Urmila's case: She has discogenic neck pain + facet arthropathy with referred shoulder pain. She does NOT have neurological signs (no weakness, no sensory loss, full ROM), which places her in the category of axial (discogenic) neck pain with facet referral - the most manageable, conservative-treatment-responsive category.
SECTION 6 - CLINICAL FEATURES (Correlating with Urmila)
| Feature | Urmila's Finding | Clinical Significance |
|---|
| Age 70F | High-risk demographic | Age-related degeneration |
| Neck pain | Present | Primary complaint, axial origin |
| Referred shoulder pain | Present (shoulder only) | Facet sclerotomal referral (C4-C5-C6) |
| Rest pain | Present | Inflammatory phase; congestion of venous plexus at rest |
| Pain eases with activity | Present | Classic feature of cervical facet/discogenic pain - movement improves venous drainage and warms up joints |
| Swelling | Present | Periarticular soft tissue inflammation |
| Tenderness on palpation | Present | Facet joint tenderness, paravertebral muscle spasm |
| Full active ROM | Present | No bony ankylosis, no significant nerve root compromise |
| End-range pain | Present | Joint capsule stress at end of available range - typical facet arthritis sign |
| No neurological deficits | Implied | No radiculopathy; conservative management appropriate |
Why does pain occur at rest but NOT with activity?
- At rest, there is relative venous stasis and increased intra-articular pressure in the inflamed facet joints
- Movement promotes synovial fluid circulation, warms up joint cartilage, and improves local blood flow
- This "morning stiffness / rest pain that eases with movement" pattern is classic for osteoarthritis/spondylosis
SECTION 7 - INVESTIGATIONS (Recommended, Even Though Not Done)
Plain X-ray (Lateral Cervical Spine) - Most important first investigation:
Lateral cervical spine radiograph showing typical spondylosis and osteoarthritis changes - from Bradley and Daroff's Neurology in Clinical Practice
Expected findings in cervical spondylosis:
- Reduced disc space height (especially C5-C6, C6-C7)
- Osteophyte formation at vertebral margins
- Subchondral sclerosis at facet joints
- Loss of normal cervical lordosis
Five vertebral lines to examine on lateral X-ray (Miller's Orthopaedics):
- Prevertebral soft tissue line
- Anterior vertebral line
- Posterior vertebral line
- Spinolaminar line
- Spinous process line
MRI (if neurological signs develop): Shows disc degeneration as "dark disc" (decreased T2 signal), with or without annular tear.
For canal stenosis assessment: Normal canal diameter = 14 mm or greater; <10 mm = absolute stenosis (Miller's Orthopaedics, 9th Ed.).
SECTION 8 - DIFFERENTIAL DIAGNOSIS
- Cervical Radiculopathy - ruled out by absence of dermatomal numbness/tingling, normal reflexes, no weakness
- Periarthritis Shoulder / Rotator Cuff Pathology - should be assessed clinically (if shoulder ROM is restricted on its own, this co-exists)
- Cervical Myelopathy - ruled out by absence of gait disturbance, hand clumsiness, bladder symptoms
- Fibromyalgia - bilateral, widespread pain; not matching here
- Rheumatoid Arthritis - bilateral joint involvement, elevated ESR/CRP; C1-C2 involvement typical
SECTION 9 - PHYSIOTHERAPY TREATMENT PLAN (DETAILED)
GOALS OF TREATMENT
- Relieve pain and reduce inflammation
- Restore full pain-free range of motion
- Correct postural abnormalities (forward head posture)
- Strengthen weakened muscles (deep cervical flexors, scapular stabilizers)
- Stretch tight/shortened muscles (upper trapezius, levator scapulae, scalenes, pectorals)
- Educate patient on self-management and activity modification
- Prevent recurrence
PHASE 1 - ACUTE / PAIN RELIEF PHASE
A. TENS (Transcutaneous Electrical Nerve Stimulation)
Why we give it:
TENS is given to provide non-pharmacological pain relief by stimulating large-diameter sensory nerve fibers (Aβ fibers) in the skin and subcutaneous tissues of the neck region.
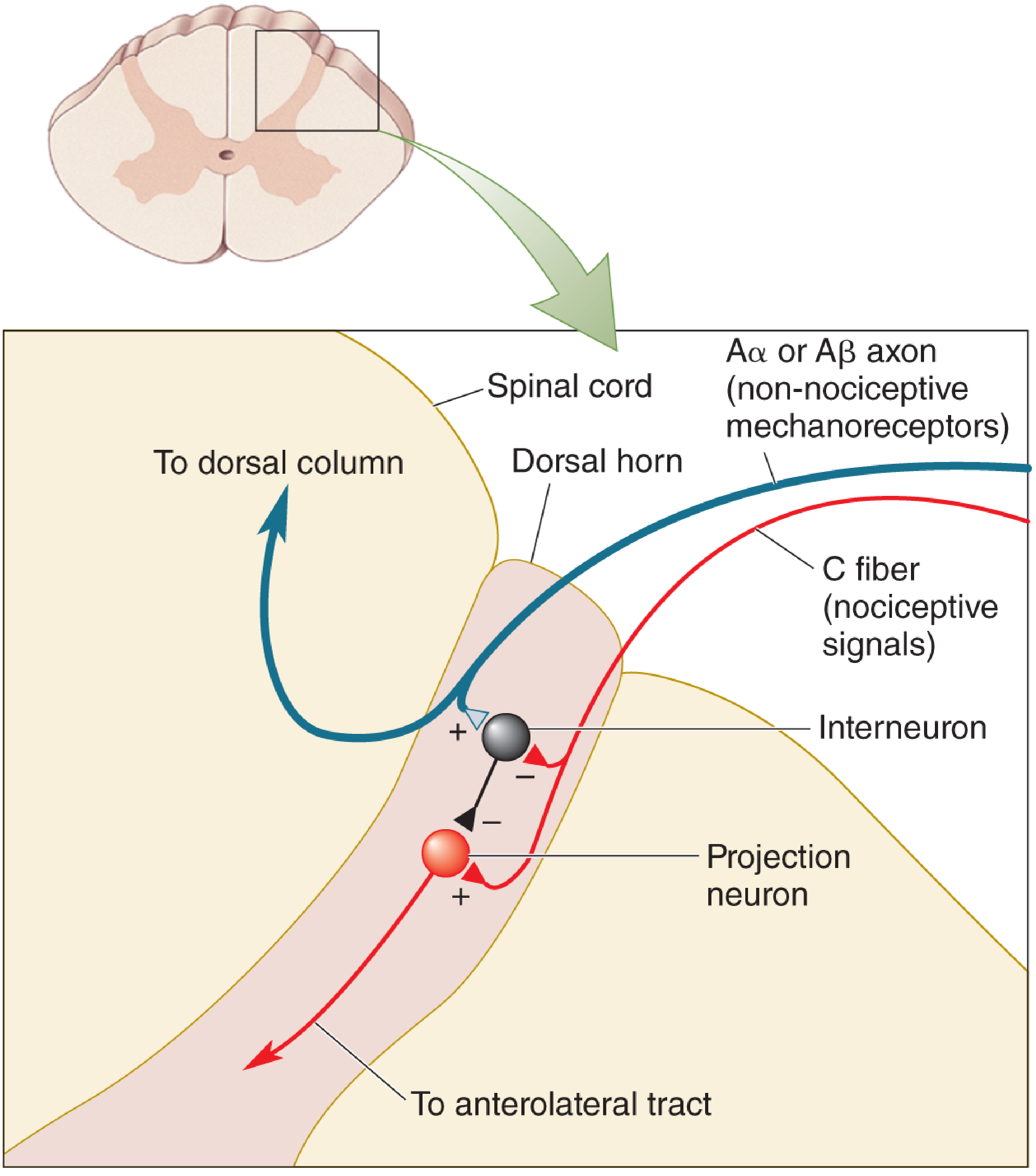
Mechanism - Gate Control Theory (Melzack & Wall, 1965):
Gate Control Theory of Pain - from Neuroscience: Exploring the Brain, 5th Edition
- TENS activates large-diameter Aβ (non-nociceptive) mechanoreceptor fibers
- These Aβ fibers synaptically excite inhibitory interneurons in the dorsal horn of the spinal cord
- These inhibitory interneurons then "close the gate" - they block the pain signals from the small-diameter C fibers (nociceptive) from reaching the projection neurons (anterolateral tract)
- Result: Pain transmission is reduced at the spinal cord level without any drugs
From Neuroscience: Exploring the Brain, 5th Edition: "When the large axons fire at high rates (e.g., because skin has been rubbed, or tickled by TENS), inhibitory interneurons are synaptically excited and close a neural 'gate', which reduces the ability of nociceptive axons to excite the anterolateral projection neurons."
Additionally, TENS at higher intensities can also trigger endorphin release (opioid-mediated analgesia), adding a second layer of pain relief.
TENS Parameters for Cervical Spondylosis:
| Parameter | Value |
|---|
| Mode | Conventional TENS (high frequency, low intensity) |
| Frequency | 80-100 Hz |
| Pulse width | 50-100 microseconds |
| Intensity | Sensory threshold (tingling, no muscle contraction) |
| Electrode placement | Bilateral paraspinal muscles of cervical spine (C4-C6 level) |
| Duration | 20-30 minutes per session |
| Frequency | Once daily or twice daily |
Why in Urmila specifically: She has rest pain and tenderness - TENS will modulate the chronic low-grade inflammatory pain, allow her to tolerate subsequent exercises, and improve her function without adding medication burden in this 70-year-old patient.
B. Infrared Radiation (IRR) / Heat Therapy
Why we give it:
Infrared radiation delivers superficial heat to the cervical muscles and soft tissues, producing the following therapeutic effects:
-
Vasodilation: Heat causes blood vessel dilation, increasing local blood flow. This brings more oxygen and nutrients to the degenerating tissues and removes metabolic waste products (lactate, bradykinin, substance P) that contribute to pain.
-
Muscle relaxation: Heat reduces muscle spindle activity, lowering the threshold for muscle relaxation. The paravertebral muscles in cervical spondylosis are typically in a state of protective spasm - heat breaks this cycle.
-
Analgesic effect: Increased tissue temperature raises the pain threshold by reducing nerve conduction velocity of nociceptive fibers and by activating thermoreceptors that modulate pain perception.
-
Increased tissue extensibility: Heat makes collagen fibers more pliable - this allows subsequent stretching to be more effective and safer (soft tissue warm before stretching = better elongation, less injury risk).
-
Counter-irritation (revulsive effect): Stimulation of thermal receptors in the skin competes with pain signals at the spinal cord level.
IRR Parameters:
| Parameter | Value |
|---|
| Type | Near infrared lamp (850-1000 nm) |
| Distance from skin | 45-60 cm |
| Duration | 15-20 minutes |
| Frequency | Daily |
| Precautions | Check skin sensation, avoid direct eye exposure |
Clinical significance in Urmila: Her swelling and tenderness indicate active inflammation in periarticular soft tissues. IRR helps reduce periarticular muscle spasm before exercise begins, and makes stretching safer and more comfortable. It is particularly gentle and safe for a 70-year-old patient.
Note: IRR is given BEFORE exercise/stretching as a warm-up. TENS can be given before or after, or independently.
C. Cervical Traction (Mechanical/Manual)
Why we give it: Traction creates gentle distraction forces on the cervical vertebrae, temporarily increasing the intervertebral foraminal space, reducing intradiscal pressure, and stretching tightened facet joint capsules.
- Relieves nerve root compression
- Reduces spasm in paraspinal muscles
- Restores normal disc height temporarily
- Reduces facet joint loading
Parameters: 5-10 kg weight, 20-30 degree flexion, intermittent traction, 10-15 minutes
PHASE 2 - STRETCHING (Detailed - Why, What, and Effects)
Before explaining the exercises, it is important to understand the muscle imbalance that develops in cervical spondylosis:
Muscle Imbalance Pattern in Cervical Spondylosis:
In cervical spondylosis and forward head posture (very common in housewives due to prolonged kitchen/household postures), a characteristic pattern develops:
| Muscles That Become TIGHT / SHORTENED (Overactive) | Muscles That Become WEAK / LENGTHENED (Inhibited) |
|---|
| Upper Trapezius | Deep Cervical Flexors (Longus Colli, Longus Capitis) |
| Levator Scapulae | Lower Trapezius |
| Scalenes (anterior, middle, posterior) | Serratus Anterior |
| Suboccipital muscles | Rhomboids |
| Sternocleidomastoid (SCM) | Middle Trapezius |
| Pectoralis Minor | Deep neck extensors (multifidus) |
Why this imbalance happens: In forward head posture, the head translates anteriorly. The posterior neck muscles (upper trapezius, levator scapulae) must work constantly to support the weight of the head against gravity - they shorten and become hyperactive. Meanwhile, the deep anterior neck stabilizers (longus colli, longus capitis) become inhibited and lengthened because they no longer need to work as primary stabilizers.
Every 2.5 cm of forward head translation adds approximately 4.5 kg of effective load on the cervical spine - this massively accelerates degenerative changes.
WHY WE STRETCH - PURPOSE:
- Restore normal resting length of shortened muscles
- Reduce compressive forces on cervical facet joints and discs (tight muscles act like a vice, compressing already degenerate joints)
- Improve ROM - tight upper trapezius and levator scapulae limit cervical lateral flexion and rotation
- Reduce pain - shortened muscles have increased tone, which increases intra-muscular pressure and triggers trigger points that refer pain to the shoulder
- Improve neural glide - tight scalenes can compress the brachial plexus (thoracic outlet), contributing to referred shoulder pain
SPECIFIC STRETCHES AND THEIR RATIONALE:
1. Upper Trapezius Stretch
What it stretches: Upper trapezius (runs from cervical spine/occiput to clavicle/acromion)
Why: Upper trapezius is the most consistently tight muscle in cervical spondylosis. When tight, it:
- Elevates the shoulder girdle, creating upper trapezius trigger points that refer pain to the neck and shoulder
- Compresses the C3-C4 facet joints
- Limits cervical lateral flexion
How: Sit upright. Tilt the head to the right (right ear toward right shoulder). Hold the chair with the left hand (to stabilize the left shoulder). Feel the stretch along the left side of the neck and upper shoulder. Hold 20-30 seconds. Repeat 3 times each side.
What it WEAKENS/Relaxes: Upper trapezius (reduces hypertonicity)
What it STRENGTHENS: Nothing directly - this is a passive stretch
2. Levator Scapulae Stretch
What it stretches: Levator scapulae (runs from C1-C4 transverse processes to superior angle of scapula)
Why: Levator scapulae is another consistently tight muscle. When shortened, it:
- Creates a tight band along the posterior-lateral neck
- Produces a characteristic trigger point at the superior angle of the scapula that refers pain to the neck and back of the shoulder
- Restricts cervical rotation and lateral flexion
- Elevates the scapula, contributing to scapular dyskinesis
How: Sit upright. Tilt the chin toward the chest. Then rotate the chin toward the left armpit (45-degree rotation + flexion). Hold the chair with the right hand. Hold 20-30 seconds, 3 repetitions each side.
What it WEAKENS/Relaxes: Levator scapulae
What it STRENGTHENS: Indirectly activates antagonist - lower trapezius and serratus anterior
3. Scalene Stretch (Anterior/Middle Scalene)
What it stretches: Scalene muscles (anterior, middle, posterior - run from cervical transverse processes C2-C7 to first and second ribs)
Why: Tight scalenes:
- Compress the brachial plexus and subclavian artery between the scalene muscles (thoracic outlet syndrome component), which can worsen referred shoulder pain
- Restrict ipsilateral lateral flexion of the neck
- In Urmila: the referred shoulder pain may partly be due to scalene tightness compressing the neural structures
How: Sit upright, depress the right shoulder (hold the chair). Tilt the head to the left. Gently rotate slightly away from the tight side. Hold 20-30 seconds.
What it WEAKENS/Relaxes: Scalenes, SCM
What it STRENGTHENS: Indirectly encourages deep neck flexor activation
4. Chin Tuck (Cervical Retraction Stretch)
What it does: This is BOTH a stretch AND an exercise.
-
STRETCHES: Suboccipital muscles and posterior cervical extensors (tightened by forward head posture). The chin tuck physically moves the head back into proper alignment, lengthening the shortened posterior suboccipital muscles.
-
STRENGTHENS: Deep cervical flexors (longus colli, longus capitis) - the most important WEAKENED muscles in cervical spondylosis. When you perform a chin tuck, you are actively contracting the deep neck flexors to draw the chin backward.
Why this is the most important single exercise:
- Restores the natural cervical lordosis
- Activates the deep cervical flexors (the "core" of the neck)
- Reduces compressive loads on the posterior elements (facets)
- Directly counteracts forward head posture
How: Sit or stand with spine erect. Gently draw the chin straight backward (like making a "double chin"). Hold 5-10 seconds. Repeat 10 times.
STRENGTHENS: Deep cervical flexors (longus colli, longus capitis) - the WEAK muscles
WEAKENS/RELAXES: Suboccipital extensors, SCM - the TIGHT muscles
PHASE 3 - STRENGTHENING EXERCISES (Why and What They Strengthen)
Why We Strengthen:
Strengthening is needed because:
- Weak muscles cannot protect the degenerating joints - strong muscles act as dynamic stabilizers, absorbing load and reducing stress on passive structures (discs, facets, ligaments)
- Muscle atrophy is accelerated in elderly patients - at age 70, Urmila's muscles are weaker than a younger patient; sarcopenia further reduces cervical muscle mass
- Without strengthening, the pain relief from TENS/IRR will be temporary - functional improvement requires muscular support
Specific Strengthening Exercises:
1. Isometric Neck Exercises (All Planes)
Why isometric: At the beginning of treatment, joints are painful. Isometric exercises generate muscle force WITHOUT joint movement, so they strengthen muscles without stressing inflamed facet joints.
What they strengthen:
- Isometric flexion: Deep cervical flexors
- Isometric extension: Cervical extensors (semispinalis, multifidus)
- Isometric lateral flexion: Scalenes, sternocleidomastoid (on working side)
- Isometric rotation: Sternocleidomastoid, splenius capitis
How: Apply gentle hand resistance to the forehead/side of head. Push head into hand without allowing movement. Hold 5-10 seconds. 10 repetitions in each direction.
2. Scapular Retraction (Lower Trapezius Strengthening)
Why: Lower trapezius is consistently WEAK in cervical spondylosis. When it is weak, the scapula tilts anteriorly and the shoulder girdle is pulled forward, worsening forward head posture and increasing neck muscle load.
What it strengthens: Lower and middle trapezius, rhomboids
What it relaxes: Pectorals, upper trapezius (reciprocal inhibition)
How: Sit upright. Squeeze shoulder blades together and down (not just together - also DOWN to activate lower trapezius). Hold 10 seconds. 15 repetitions.
3. Deep Neck Flexor Endurance Training (Advanced Chin Tuck)
Why: The deep cervical flexors (longus colli) are the primary stabilizers of the cervical spine. Research shows they are consistently inhibited and weak in patients with chronic neck pain. Strengthening them:
- Reduces anterior shear forces on cervical discs
- Reduces compressive loading of facet joints
- Restores proprioceptive control of head position
How: Lying supine, perform chin tuck then gently lift the head 1-2 cm off the floor. Hold 10 seconds. This is NOT a full sit-up - only a tiny head lift while maintaining the chin tuck.
STRENGTHENS: Longus colli, longus capitis (deep neck flexors)
WEAKENS/INHIBITS: Superficial neck flexors (SCM, anterior scalene) through reciprocal inhibition
4. Shoulder Blade Push-Ups (Serratus Anterior)
Why: Serratus anterior is weak in forward head posture. When weak, the scapula "wings" and the entire shoulder girdle mechanics are disturbed. This directly worsens shoulder pain in Urmila.
What it strengthens: Serratus anterior, lower trapezius
PHASE 4 - POSTURAL CORRECTION AND PATIENT EDUCATION
This is critical for Urmila as a housewife because she spends hours in:
- Kitchen work (sustained forward head posture)
- Bending over a stove or washing sink
- Carrying loads on her head or arms
Education points:
- Ergonomic advice: Raise cooking surface height if possible. Avoid sustained head-down positions.
- Sleeping posture: One pillow, appropriate height to maintain neutral cervical spine. Avoid sleeping prone (which requires 90-degree neck rotation and compresses facets).
- Posture correction: Ears should be directly over shoulders over hips - not forward.
- Activity modification: Avoid heavy lifting, prolonged overhead work, or sudden neck movements.
- Heat at home: Warm towel/heating pad to cervical region for 15 minutes before activity, to warm up the joints and reduce morning stiffness.
COMPLETE TREATMENT SUMMARY TABLE
| Modality/Technique | Rationale | Specific Effect in Urmila |
|---|
| TENS (80-100 Hz, 20-30 min) | Gate control - Aβ fibers close pain gate; endorphin release | Reduces rest pain and tenderness |
| Infrared Radiation (15-20 min, 45-60 cm) | Vasodilation, muscle relaxation, raises pain threshold, warms tissue for stretching | Reduces periarticular swelling, relaxes paraspinal spasm, prepares tissue for exercise |
| Cervical Traction (intermittent, 5-10 kg) | Decompresses foramina and facets, reduces intradiscal pressure | Reduces referred shoulder pain by relieving neural/joint compression |
| Upper Trapezius Stretch | Reduces tightness that compresses C3-C4 facets and refers to shoulder | Reduces referred shoulder pain |
| Levator Scapulae Stretch | Reduces tightness at C1-C4, trigger point at scapular angle | Reduces posterior neck and shoulder pain |
| Scalene Stretch | Decompresses brachial plexus at thoracic outlet | Reduces arm and shoulder referred pain |
| Chin Tuck (stretch + exercise) | Stretches suboccipitals, STRENGTHENS deep cervical flexors, corrects forward head | Core exercise for cervical spondylosis - corrects root cause |
| Isometric Exercises | Strengthens paraspinal muscles without stressing inflamed joints | Dynamic stability for degenerated cervical segments |
| Scapular Retraction | Strengthens lower trapezius, corrects scapular position | Reduces shoulder girdle load transmitted to cervical spine |
| Postural Education | Modifies activities that accelerate degeneration | Prevents recurrence, empowers Urmila in self-care |
PROGNOSIS
Urmila's case has a good prognosis for conservative physiotherapy because:
- No neurological signs (no radiculopathy or myelopathy)
- Full active ROM present
- Pain is primarily mechanical/inflammatory in nature
- Axial (discogenic/facet) pain is the most treatment-responsive category
From Miller's Orthopaedics: "Patient education emphasizing the self-limiting nature of symptoms is important" and "nonsurgical treatment - NSAIDs, cervical epidural injections, isometric exercises, traction, and occasionally temporary collar immobilization" are the standard approach.
Expected improvement: 4-6 weeks of consistent physiotherapy typically produces significant pain reduction and functional improvement in uncomplicated cervical spondylosis. Full resolution may take 8-12 weeks.
SOURCES
- Miller's Review of Orthopaedics, 9th Edition (cervical spondylosis, anatomy, treatment)
- Bradley and Daroff's Neurology in Clinical Practice (epidemiology, cervical spondylosis)
- Neuroscience: Exploring the Brain, 5th Edition (TENS mechanism, gate control theory)
- Neuroanatomy Through Clinical Cases, 3rd Edition (gate control, dorsal horn)
- Narrative review - physical therapy for cervical spondylosis (PMC)