
IMG-20260707-WA0003.jpg
Answer
Answer: b. Borderline tuberculoid leprosy
Reasoning:
The key features in this case are:
- Multiple hypoesthetic, mildly erythematous large plaques with elevated margins - this points away from pure tuberculoid (which has very few, well-defined lesions) and away from lepromatous (which has many small, poorly defined, symmetric lesions)
- Bilateral enlarged peripheral nerves (ulnar + lateral popliteal) - nerve enlargement is prominent in the tuberculoid spectrum
- Hypoesthesia - indicates significant immune-mediated nerve damage, typical of the tuberculoid end of the spectrum
Why the other options are wrong:
| Option | Why excluded |
|---|---|
| a. Lepromatous leprosy | Lesions are numerous, small, poorly defined, symmetric macules/nodules; nerves enlarged but less dramatically; sensation often preserved early |
| c. Borderline leprosy (BB) | Most unstable form; lesions are "Swiss cheese" shaped with punched-out centers; nerve involvement less prominent |
| d. Borderline lepromatous (BL) | Many small lesions, less defined margins, less hypoesthesia, more bacilli; nerve thickening less pronounced |
Borderline tuberculoid (BT) is characterized by:
- Few to several plaques (more than pure TT, but not numerous)
- Large plaques with raised, well-defined outer edges and sloping inner edges
- Marked hypoesthesia
- Peripheral nerve thickening (classically ulnar and lateral popliteal nerves)
- Paucibacillary on slit-skin smear
The combination of large plaques with elevated margins + bilateral nerve enlargement + hypoesthesia is classic for BT leprosy.
Help me learn about different types of leprosy in simple terms first and then in detail for a final year mbbs student
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, authoritative content from Harrison's 22e, Robbins Pathology, and Park's PSM to write an outstanding answer. Here it is:
Leprosy (Hansen's Disease) - Complete Guide
PART 1: SIMPLE EXPLANATION (Beginner Level)
What is leprosy?
Leprosy is a slow, chronic infection caused by the bacterium Mycobacterium leprae. It mainly attacks two things: skin and peripheral nerves (the nerves outside the brain and spinal cord). It is NOT highly contagious - most people (about 95%) who are exposed never get the disease.
The One Big Concept: It's a SPECTRUM
Think of leprosy like a slider between two extremes:
STRONG IMMUNITY ←————————————————————→ WEAK IMMUNITY
TT ——— BT ——— BB ——— BL ——— LL
Few lesions, Many lesions,
few bacteria, many bacteria,
lots of nerve damage less nerve damage early
- Left side (TT): Your immune system fights hard. It kills most bacteria. But in doing so, it destroys the nerves too. Few skin lesions, lots of nerve damage.
- Right side (LL): Your immune system barely responds. Bacteria multiply everywhere. Many skin lesions all over, but nerve damage comes later.
- Middle (Borderline types): Mix of both features.
Simple Memory Trick
| Feature | Tuberculoid (TT) | Lepromatous (LL) |
|---|---|---|
| Skin lesions | Few (1-3) | Many (dozens) |
| Bacteria in lesions | Almost none | Packed full |
| Nerve thickening | Prominent, asymmetric | Symmetric, less prominent early |
| Sensation loss | Severe | Less severe early |
| Immunity | Strong | Weak |
| Lepromin test | Positive | Negative |
PART 2: DETAILED GUIDE (Final Year MBBS Level)
The Organism
Mycobacterium leprae is an obligate intracellular pathogen that:
- Cannot be cultured in vitro (grown in labs)
- Grows best at 27-33°C (prefers cool body areas: skin, peripheral nerves, testes, nasal mucosa, ear lobes)
- Its virulence is partly due to PGL-1 (phenolic glycolipid-1), which helps it invade host cells
- Primarily infects Schwann cells and dermal macrophages
- A newer species, M. lepromatosis (discovered 2008), causes diffuse lepromatous leprosy mainly in Mexico/Central America
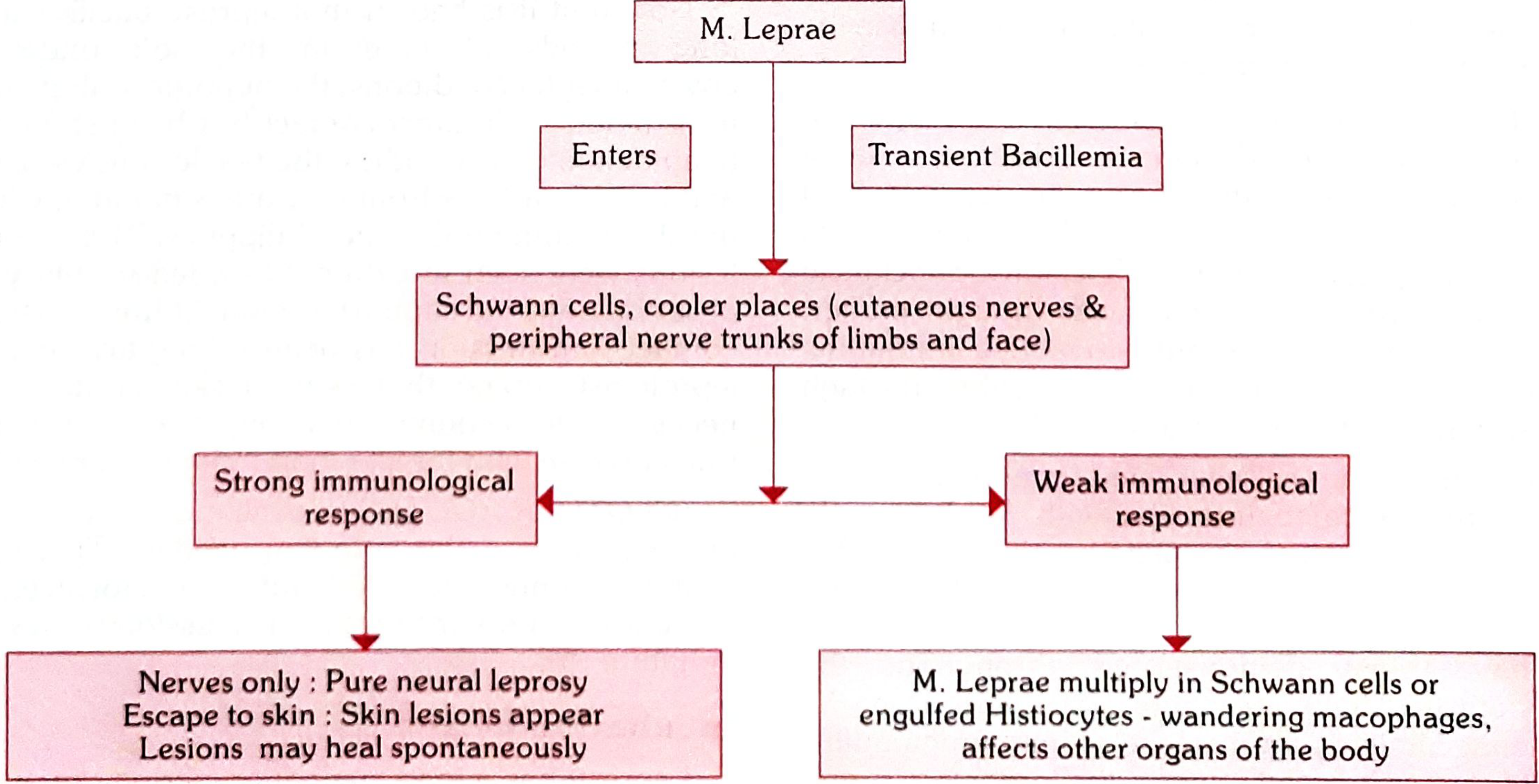
Park's Textbook of Preventive and Social Medicine - Pathogenesis of Leprosy
Transmission
- Primarily via respiratory secretions (nasal droplets) from untreated multibacillary patients
- Rare zoonotic transmission from armadillos
- Prolonged close contact required; the disease is NOT highly contagious
- Incubation period: 2-12 years (average ~5 years)
Immunology - The Key to Understanding the Spectrum
The type of leprosy that develops depends entirely on the cell-mediated immune (CMI) response:
| Immune response | Th1 (IFN-γ, IL-2) | Th2/Tregs | CMI | Result |
|---|---|---|---|---|
| Tuberculoid end | Strong | Weak | Strong | Few lesions, paucibacillary |
| Lepromatous end | Weak | Dominant | Weak | Many lesions, multibacillary |
HLA associations:
- HLA-DR2 and HLA-DR3 → tuberculoid form
- HLA-DQ1 → lepromatous form
In TT leprosy: Macrophages + lymphocytes → epithelioid cells + Langerhans giant cells → tight granuloma → kills bacteria but destroys nerves
In LL leprosy: Macrophages engulf bacteria but cannot kill them → histiocytes become "lepra cells" (Virchow cells) packed with bacteria → "globi" = clumps of acid-fast bacilli inside macrophages
Classifications of Leprosy
1. Ridley-Jopling Classification (Most important for exams)
| Type | Code | Key Features |
|---|---|---|
| Indeterminate | IL | Earliest form; may self-heal or progress |
| Tuberculoid | TT | Polar; few lesions, strong immunity |
| Borderline Tuberculoid | BT | Several lesions, asymmetric nerve involvement |
| Mid-Borderline | BB | Unstable; "Swiss cheese" lesions |
| Borderline Lepromatous | BL | Many lesions, less defined |
| Lepromatous | LL | Polar; many lesions, weak immunity |
2. WHO Classification (Used in field/control programs)
| Type | Criteria | Treatment |
|---|---|---|
| Paucibacillary (PB) | 1-5 lesions, ≤1 nerve, smear negative | 6 months MDT |
| Multibacillary (MB) | ≥6 lesions, >1 nerve, OR smear positive | 12 months MDT |
3. Indian Classification (Used in India)
- Indeterminate, Tuberculoid, Borderline, Lepromatous, Pure Neuritic (no skin lesions - unique to Indian classification)
Cardinal Features of Leprosy (Diagnose if ANY ONE present)
- Hypopigmented/erythematous skin patch with loss of sensation
- Thickened peripheral nerve trunk
- AFB positive on slit-skin smear or biopsy
Each Type in Detail
1. Indeterminate Leprosy (IL)
- Earliest stage - may be the only manifestation
- 1-2 ill-defined hypopigmented or faintly erythematous macules, 1-5 cm
- Occurs on limbs, buttocks, face
- Mild to moderate loss of touch/thermal sensation
- No nerve thickening
- Either self-heals or progresses to any determinate type depending on immunity
- Biopsy shows only lymphocytic infiltration (no granuloma yet)
2. Tuberculoid Leprosy (TT)
Skin:
- Single or very few (up to 3) well-defined lesions
- Raised, erythematous/copper-colored plaque with clearly defined outer edge sloping inward to a hypopigmented, depressed center (central healing)
- Can be of any size; surface is dry, hairless, anhidrotic, and completely anesthetic
- Complete loss of fine touch and temperature sensation over the lesion
Nerves:
- One peripheral nerve near the lesion may be thickened
- Asymmetric nerve involvement
- Nerve thickening with sensory loss and possible motor deficit
Bacteriology: AFB absent on slit-skin smear (paucibacillary)
Lepromin test: Strongly positive (Mitsuda reaction ≥5mm)
Histology: Tight, well-formed epithelioid cell granulomas with Langerhans giant cells and lymphocytes; nerves may be completely destroyed; no AFB seen
Prognosis: Relatively stable; may self-heal
3. Borderline Tuberculoid (BT) Leprosy
- 3 to 9+ lesions, asymmetrically distributed
- Plaques with edges sloping outward (opposite to TT)
- Smaller "satellite" lesions around the main lesion
- Variable loss of sensation (less than TT)
- Several peripheral nerves enlarged asymmetrically (ulnar, lateral popliteal commonly)
- Highly prone to Type 1 (reversal) reactions
- Bacteriologic Index (BI): 0 to 1+
- Lepromin test: Positive (weakly)
- If untreated, may downgrade toward BB or BL
This is the most common type seen in Indian clinical exams (as in the MCQ from your image)
4. Mid-Borderline (BB) Leprosy
- Most immunologically unstable form - can upgrade or downgrade
- Multiple lesions of varying sizes and shapes
- Characteristic "Swiss cheese" (punched-out) lesions - central clearing with a sharp inner edge but sloping outer edge
- Lesions may look like annular plaques with a "punched-out" pale center
- Sensation impaired but not totally lost
- Nerves involved but less severely than BT
- BI: 2+ to 3+
- Lepromin test: Negative or weakly positive
- Most likely to undergo lepra reactions
5. Borderline Lepromatous (BL) Leprosy
- Many lesions (more numerous and smaller than BB)
- Less-defined margins, more symmetric distribution than BT/BB
- Macules, papules, plaques, nodules
- Reduced sensation but not absent
- Nerve involvement: multiple nerves, more symmetric than BT
- BI: 3+ to 5+
- Lepromin test: Negative
- Can undergo Type 2 reactions (ENL - Erythema Nodosum Leprosum)
6. Lepromatous Leprosy (LL)
Skin:
- Many (dozens to hundreds) of lesions, symmetric distribution
- Early: poorly defined hypopigmented macules
- Late: papules, nodules, and plaques - especially on face, ears, wrists, elbows, knees
- Leonine facies = thickened, corrugated skin of face due to nodule coalescence
- Madarosis = loss of lateral eyebrows (pathognomonic)
- Saddle-nose deformity (nasal collapse from septal destruction)
- Ear lobes thickened and infiltrated
- Sensation relatively preserved early
Nerves:
- Symmetric peripheral nerve involvement
- Nerves invaded with bacteria but minimal inflammation
- Commonly affected: ulnar, median, lateral popliteal, posterior tibial, radial cutaneous, facial, greater auricular
- "Glove and stocking" sensory loss pattern
Systemic features:
- Orchitis → testicular atrophy → sterility and gynaecomastia
- Eye involvement: iridocyclitis, corneal anesthesia, lagophthalmos
- Laryngeal involvement → hoarseness
- Lymphadenopathy
- Hepatosplenomegaly
- In advanced disease: bacilli in blood and sputum
Bacteriology: AFB 4+ to 6+ (massive numbers)
- "Globi" = clumps of AFB in macrophages
- Virchow cells (lepra cells) = lipid-laden macrophages packed with AFB
Lepromin test: Negative (no CMI)
Histology: Sheets of foamy macrophages (Virchow cells); very few lymphocytes; nerves invaded but architecture preserved; AFB easily found in clumps ("globi")
Histology at a Glance
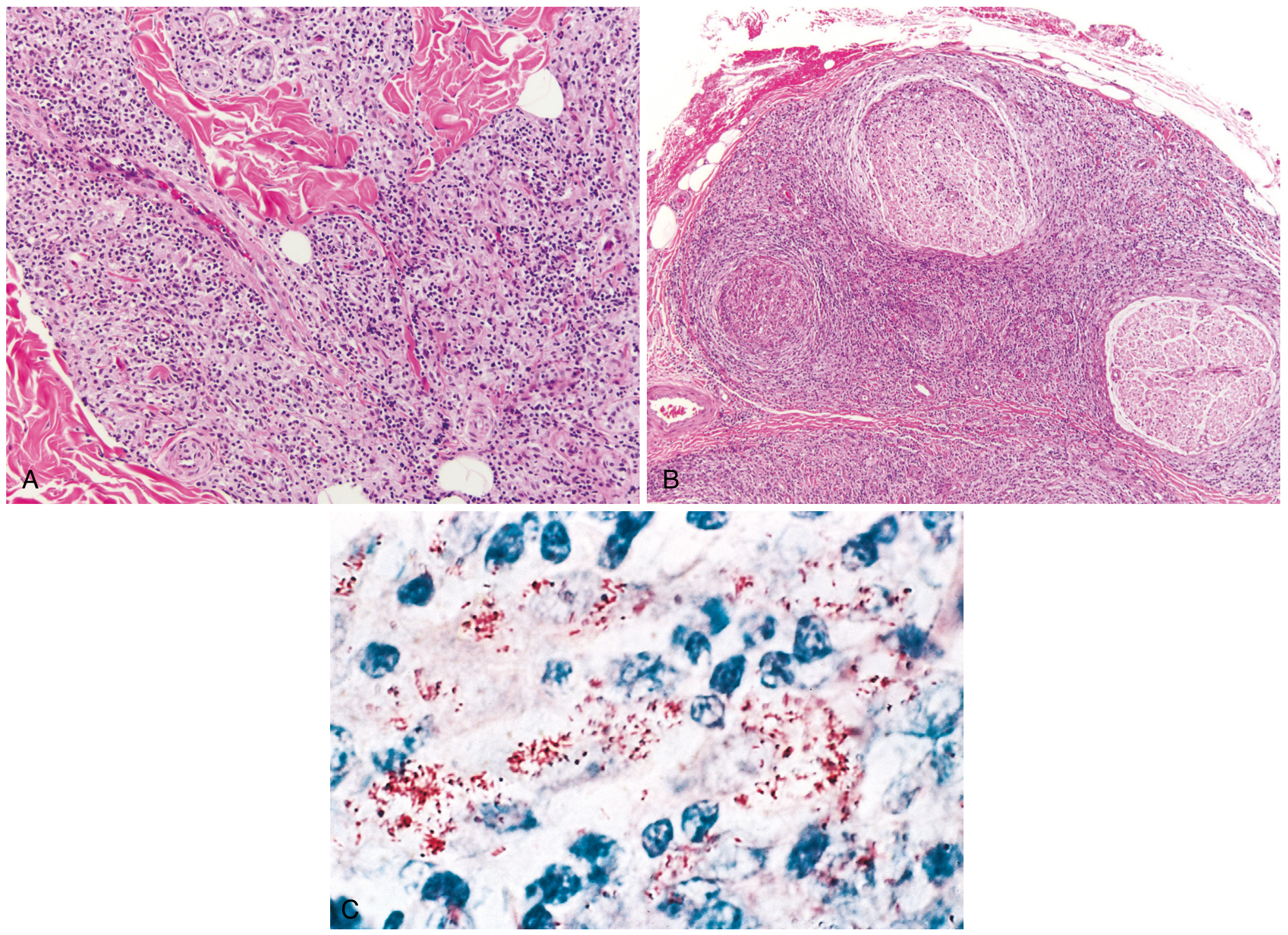
Robbins Pathology - (A) Tuberculoid leprosy: macrophage infiltration surrounding nerves and adnexa; (B) Lepromatous leprosy: dense lymphocytic infiltration into large nerve bundles; (C) AFB (red) within macrophages in lepromatous form
| Feature | Tuberculoid (TT) | Lepromatous (LL) |
|---|---|---|
| Granuloma type | Tight epithelioid + Langerhans giant cells | Loose; foamy macrophages (Virchow/lepra cells) |
| Lymphocytes | Many | Very few |
| AFB | Absent | Abundant (globi) |
| Nerve architecture | Destroyed | Preserved but infiltrated |
| Subepidermal clear zone | Absent | Present (Grenz zone) |
Nerves Commonly Affected (Must Know)
| Nerve | Site of thickening | Consequence |
|---|---|---|
| Ulnar nerve | Behind medial epicondyle | Claw hand (4th, 5th fingers) |
| Median nerve | At wrist | Claw hand (2nd, 3rd fingers), ape hand |
| Radial nerve | Lateral arm | Wrist drop |
| Lateral popliteal (common peroneal) | Neck of fibula | Foot drop |
| Posterior tibial | Behind medial malleolus | Plantar anesthesia, trophic ulcers |
| Facial nerve | Zygomatic branch | Lagophthalmos |
| Greater auricular nerve | Neck | Visible/palpable thickening |
| Supra-orbital nerve | Forehead |
Leprosy Reactions (Acute Episodes)
Type 1 Reaction (Reversal Reaction)
- Who: BT, BB, BL patients (borderline types only)
- Mechanism: Sudden increase in CMI (delayed hypersensitivity) - upgrade reaction
- Features: Existing lesions become acutely inflamed (red, hot, edematous, tender); new lesions; acute nerve palsies (very important!)
- Treatment: Prednisolone 40-60 mg/day, tapered over months
Type 2 Reaction - Erythema Nodosum Leprosum (ENL)
- Who: BL and LL patients only (multibacillary end)
- Mechanism: Immune complex deposition (Type III hypersensitivity) - NOT a change in CMI
- Features: Painful, tender, erythematous nodules on skin; fever, malaise; can have uveitis, orchitis, neuritis, arthritis, lymphadenopathy
- Treatment: Thalidomide (drug of choice), or clofazimine, or prednisolone
Lucio's Phenomenon
- Only in diffuse lepromatous leprosy (M. lepromatosis)
- Necrotizing vasculitis → skin necrosis and ulceration
Diagnosis
| Test | Finding |
|---|---|
| Slit-skin smear (SSS) | AFB on Ziehl-Neelsen stain; Bacteriologic Index (BI) 0-6+ |
| Skin biopsy | Histopathology (key for classification) |
| Lepromin test (Mitsuda) | Tests CMI; positive in TT, negative in LL (not a diagnostic test - measures resistance) |
| PCR | Confirms M. leprae DNA |
| Nerve conduction studies | Assess nerve damage |
WHO MDT Treatment (Current Regimen)
Paucibacillary (PB) - 6 months
| Drug | Dose | Frequency |
|---|---|---|
| Rifampicin | 600 mg | Monthly (supervised) |
| Dapsone | 100 mg | Daily (self-administered) |
Multibacillary (MB) - 12 months
| Drug | Dose | Frequency |
|---|---|---|
| Rifampicin | 600 mg | Monthly (supervised) |
| Clofazimine | 300 mg monthly + 50 mg daily | Monthly + daily |
| Dapsone | 100 mg | Daily |
Side effects to remember:
- Rifampicin: hepatotoxicity, orange urine
- Dapsone: hemolytic anemia (especially in G6PD deficiency), methemoglobinemia, dapsone hypersensitivity syndrome
- Clofazimine: skin pigmentation (orange-brown discoloration), ichthyosis, GI symptoms
High-Yield Points for Exams
- Most common nerve affected in leprosy overall: Ulnar nerve
- Most common cause of foot drop in leprosy: Lateral popliteal (common peroneal) nerve
- Pathognomonic skin finding: Madarosis (loss of lateral eyebrow)
- Only nerve visible AND palpable: Greater auricular nerve
- Lepromin test = test of immunity, NOT a diagnostic test
- Most unstable type: BB (mid-borderline)
- Type 1 reaction only in borderline; Type 2 (ENL) only in BL and LL
- Drug of choice for ENL: Thalidomide (contraindicated in pregnancy - teratogenic)
- BCG vaccination gives partial protection (~50%) against leprosy
- Deformity of nose in LL = Saddle nose deformity (not "button nose")
- "Leonine facies" = LL leprosy
- Most common cause of blindness in leprosy = Lagophthalmos (facial nerve palsy → corneal exposure)
- Pure neuritic leprosy (no skin lesions) - recognized in Indian classification only
- Armadillos are the only non-human animal reservoir
Sources
- Harrison's Principles of Internal Medicine, 22nd Edition, 2025 - Chapter 184
- Robbins, Cotran & Kumar - Pathologic Basis of Disease - Chapter 8
- Park's Textbook of Preventive and Social Medicine - Chapter on Leprosy
This is a shared conversation. Sign in to Orris to start your own chat.