Explain bi pap
Reading File
Searching the Web
BiPAP bilevel positive airway pressure mechanism indications settings
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a thorough explanation of BiPAP drawn from multiple authoritative textbooks.
BiPAP (Bilevel Positive Airway Pressure)
What Is It?
BiPAP (also written BPAP) is a form of non-invasive ventilation (NIV) that delivers air through a tightly fitting face mask - no endotracheal tube required. The term "bilevel" refers to its defining feature: it uses two separate, independently adjustable pressure levels during the breathing cycle, unlike CPAP which maintains a single constant pressure.
- IPAP (Inspiratory Positive Airway Pressure) - the higher pressure delivered when you breathe in
- EPAP (Expiratory Positive Airway Pressure) - the lower pressure maintained when you breathe out
The difference between IPAP and EPAP is called pressure support, and this is what actively assists breathing and drives CO2 elimination.
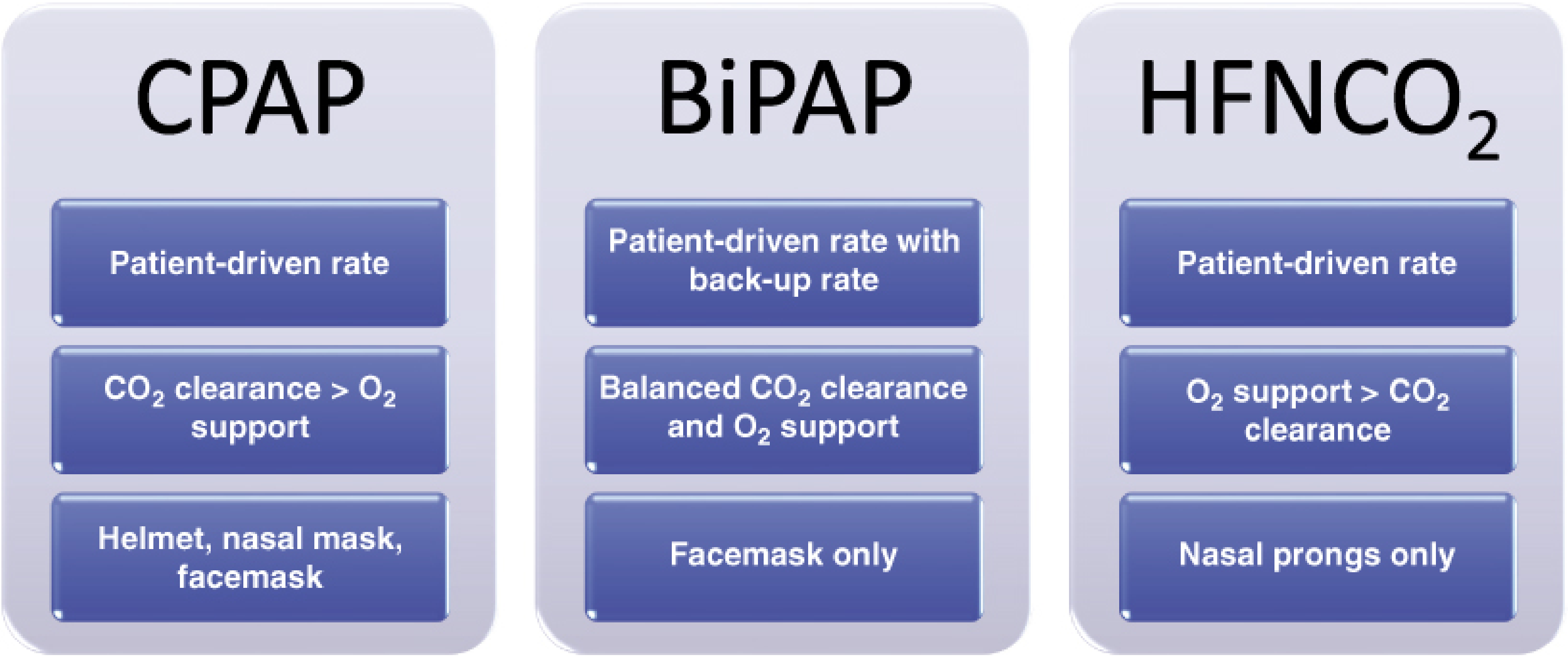
Figure: BiPAP compared to CPAP and high-flow nasal oxygen. Key distinction - BiPAP provides balanced CO2 clearance AND O2 support, whereas CPAP favors CO2 clearance and HFNCO2 favors oxygenation. BiPAP is delivered via facemask only. - Fischer's Mastery of Surgery
How It Works (Mechanism)
The machine senses the patient's inspiratory effort (via a drop in flow or pressure) and switches from EPAP to IPAP, then cycles back to EPAP when flow tapers at end-inspiration.
IPAP does two things:
- Offloads the respiratory muscles - reduces the work of breathing
- Overcomes intrinsic PEEP (iPEEP), especially important in COPD where air trapping increases end-expiratory lung volume
- Delivers larger tidal volumes, improving alveolar ventilation and CO2 clearance
EPAP (the expiratory pressure) acts like PEEP:
- Keeps alveoli open (prevents collapse/atelectasis)
- Recruits lung units, improving oxygenation
- Counterbalances iPEEP in obstructive disease
When NIV is initiated, the patient's respiratory rate decreases, allowing more effective lung emptying and larger tidal volumes. - ROSEN's Emergency Medicine
Newer BiPAP devices also include a backup rate (BPAP-ST mode) which guarantees cycling between IPAP and EPAP at a set minimum rate, in case the patient's drive is insufficient. This distinguishes it from older models that relied entirely on patient effort. - Murray & Nadel's Respiratory Medicine
BiPAP vs CPAP - Key Differences
| Feature | CPAP | BiPAP |
|---|---|---|
| Pressures | Single fixed pressure | IPAP (higher) + EPAP (lower) |
| CO2 clearance | Moderate | Strong |
| O2 support | Moderate | Balanced |
| Respiratory rate | Patient-driven | Patient-driven + optional backup rate |
| Respiratory muscle unloading | No | Yes |
| Interface | Helmet, nasal mask, or facemask | Facemask only |
Indications
Strongly recommended / first-line:
- COPD exacerbation with hypercapnic respiratory failure (pH ≤7.35, PaCO2 ≥45 mmHg) - this is the best-supported indication; BiPAP reduces mortality, intubation rates, and hospital length of stay
- Acute cardiogenic pulmonary edema - BiPAP reduces left ventricular afterload by lowering transmural pressure
- Asthma exacerbation - as a bridge while treating the underlying cause
Other uses:
- Type 2 (hypercapnic) respiratory failure from any cause
- Obstructive sleep apnea (OSA) with residual central events after CPAP
- Neuromuscular disease causing respiratory insufficiency (e.g., ALS, Duchenne muscular dystrophy)
- Obesity hypoventilation syndrome
- Bridge to intubation in impending acute respiratory failure
BiPAP is preferred over CPAP for type 2 (hypercapnic) respiratory failure because it actively assists ventilation and CO2 clearance, whereas CPAP does not.
Initial Settings
According to ROSEN's Emergency Medicine and Roberts & Hedges' Clinical Procedures in Emergency Medicine:
| Parameter | Starting Value | Notes |
|---|---|---|
| IPAP | 10-12 cm H2O | Titrate up to a max of ~20 cm H2O |
| EPAP | 5 cm H2O | Increase to 8 if obese or significant iPEEP |
| FiO2 | 100% initially | Titrate down to SpO2 88-92% (COPD), or ≥94% (others) |
Titration rules:
- Increase IPAP (increase pressure support = IPAP minus EPAP) if patient remains hypercapnic or has high work of breathing
- Increase EPAP if patient remains hypoxic
- Adjust by 1-2 cm H2O increments at a time
- IPAP >20 cm H2O should be avoided - causes discomfort and gastric insufflation
- Reassess at 30-60 minutes; check ABG at 1-2 hours
Contraindications
Absolute:
- Respiratory or cardiac arrest
- Active vomiting / high aspiration risk
- Inability to protect airway
- Facial trauma preventing mask fit
- Neuromuscular blockade (BiPAP requires an open glottis)
Relative:
- Depressed consciousness not due to hypercapnia (GCS <10)
- Copious secretions unable to be cleared
- Hemodynamic instability unresponsive to fluids/vasopressors
- Bacterial pneumonia (mask pressure makes sputum clearance difficult)
When BiPAP Fails
Failure rate is approximately 10-15%, rising with lower presenting pH and greater illness severity. Signs of NIV failure and indications to escalate to intubation include:
- Persistent tachypnea, accessory muscle use, or worsening acidosis after 30-60 minutes
- No improvement in pH or PaCO2 on repeat ABG
- Worsening mental status
- Hemodynamic instability
- Life-threatening hypoxemia
Patient-Ventilator Asynchrony
A key complication with BiPAP is asynchrony - when the ventilator's cycling does not match the patient's neural respiratory timing. This occurs in up to 43% of patients receiving NIV. The main cause is mask leaks: inspiratory leaks cause prolonged machine inspiration, while expiratory leaks cause auto-triggering. Modern NIV ventilators include leak-compensation algorithms to minimize this. - Murray & Nadel's Respiratory Medicine
Sources:
- ROSEN's Emergency Medicine, 9th ed. - Non-Invasive Ventilation (COPD chapter & General NIV chapter)
- Fischer's Mastery of Surgery, 8th ed. - Common Approaches to Noninvasive Ventilation
- Murray & Nadel's Textbook of Respiratory Medicine - BPAP with Backup Rate; Modes and Settings
- Roberts & Hedges' Clinical Procedures in Emergency Medicine - Initiation of NPPV
A useful video overview comparing CPAP and BiPAP:
This is a shared conversation. Sign in to Orris to start your own chat.