How to assess glenohumeral bone loss
Reading File
Finding Sources
Finding Sources
Searching PubMed
"glenohumeral bone loss" AND assessment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the information needed to provide a comprehensive answer. Here is a structured, evidence-based overview:
Assessment of Glenohumeral Bone Loss
Glenohumeral bone loss occurs on both sides of the joint — the glenoid (anteroinferior) and the humerus (posterosuperior Hill-Sachs lesion). Accurate pre-operative assessment of both is essential because significant bone loss predicts failure of soft-tissue stabilization and dictates the need for bony augmentation.
1. Clinical Context
- Some degree of glenoid bone loss is present in 40% of first-time dislocations and 85% of recurrent dislocations.
- A Hill-Sachs lesion is seen in 40% of patients with recurrent subluxation, 90% after first dislocation, and approaching 100% with recurrent dislocations.
- Bipolar lesions (combined glenoid + Hill-Sachs) occur in 33% of primary instability and 62% of recurrent instability cases.
2. Imaging Modalities
Plain Radiography
Several special views improve sensitivity:
| View | Technique | Purpose |
|---|---|---|
| Stryker Notch | Supine, arm over head, beam 10° cephalad | Detects Hill-Sachs lesion |
| West Point | Prone, forearm hanging, beam 25° downward + 25° medial | Detects anteroinferior glenoid rim (bony Bankart) |
| Bernageau (Glenoid Profile) | Arm flexed, beam along scapular spine at 30-40° | Glenoid profile, anterior rim loss |
| True AP (Grashey) | Standard shoulder series | Overall joint assessment |
CT Scan (Primary Modality)
CT is the standard for evaluating bone loss. High-resolution thin-slice acquisition with 3D volume-rendered reconstructions and digital subtraction of the humeral head provides the best visualization.
- Identifies smallest osseous fragments and glenoid asymmetry
- 3D CT with humeral subtraction: gold standard for glenoid bone loss quantification
- Also detects Hill-Sachs lesions with accuracy comparable to arthroscopy
- Essential when bipolar lesions are suspected
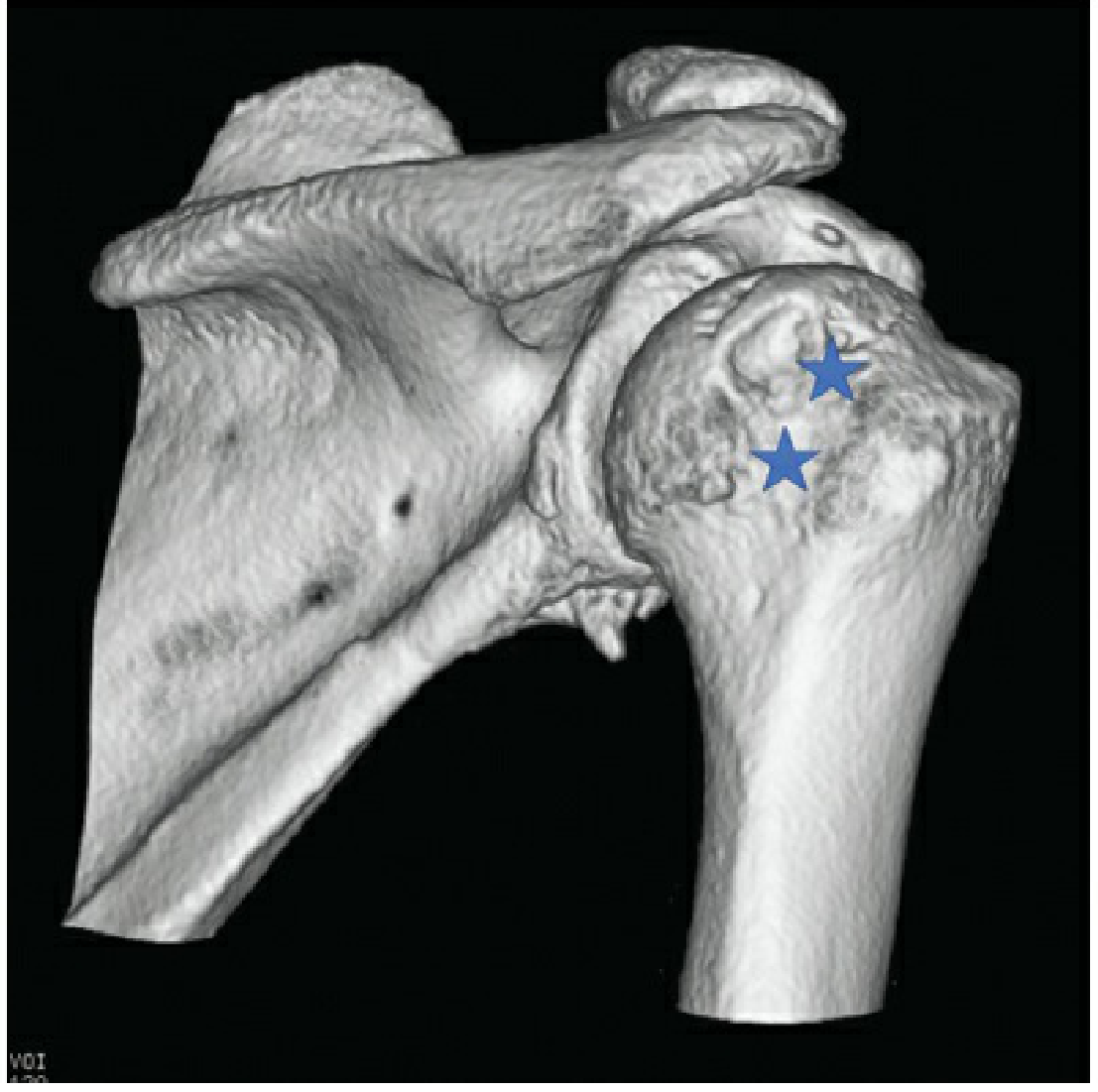
3D CT reconstruction showing Hill-Sachs lesions (★) on the posterolateral humeral head — Rockwood & Green's Fractures in Adults, 10th ed.

3D CT reconstruction of the glenoid and scapula demonstrating approximately 20% anterior glenoid bone loss — Miller's Review of Orthopaedics, 9th ed.
MRI / MR Arthrogram (MRA)
- MRA preferred over plain MRI for greater sensitivity for labral and ligamentous lesions
- ABER position (abduction-external rotation) increases sensitivity for anteroinferior labral injuries
- Circle method on MRI is accurate to within 1.3% of 3D CT for measuring glenoid bone loss
- Demonstrates capsular volume, glenoid version, and associated soft-tissue pathology
3. Quantifying Glenoid Bone Loss
A. Circle Method (most widely used)
A best-fit circle is drawn over the intact posterior glenoid on the en face view (CT or sagittal MRI). The missing segment anteriorly represents the bone loss.
% Bone loss = (diameter of best-fit circle − remaining anterior-posterior width) / diameter × 100
B. Burkhart Bare-Spot Arthroscopic Method
Arthroscopic measurement using a calibrated probe:
- Distance from bare spot to posterior glenoid margin = Dp
- Distance from bare spot to anterior glenoid margin = Da
- % Bone loss = (Dp − Da) / (2 × Dp) × 100
C. Width-Based Formula (Owens et al.)
Predicts normal glenoid width from height measurements on MRI:
- Males: Normal glenoid width = ⅓ height + 15 mm
- Females: Normal glenoid width = ⅓ height + 13 mm
4. Critical Thresholds
| Threshold | Significance |
|---|---|
| ≥20–25% glenoid bone loss (≈6–8 mm) | "Critical" defect → recurrence rate after arthroscopic Bankart repair rises to 67%; bony augmentation (Latarjet, bone graft) required |
| >21% of glenoid length | Biomechanically causes instability and ROM limitation after Bankart repair |
| Inverted-pear glenoid morphology | Corresponds to ~25–27% anteroinferior width loss |
5. Hill-Sachs Lesion Assessment and the Glenoid Track Concept
A Hill-Sachs lesion is not just quantified by size but by whether it is on-track or off-track — whether it will engage the anterior glenoid rim in functional positions.
Glenoid Track Calculation
Glenoid Track (GT) = 0.84 × actual glenoid width
(The 84% factor accounts for the medial glenoid insertion of the inferior glenohumeral ligament, which limits how far laterally the humeral head can translate.)
Hill-Sachs Interval (HSI)
Measured on coronal MRI as the distance from the rotator cuff footprint to the medial margin of the Hill-Sachs lesion.
Classification
- On-track (safe): HSI < GT → no engagement risk → arthroscopic Bankart repair alone is appropriate
- Off-track (high risk): HSI ≥ GT → engagement occurs → requires remplissage or Latarjet in addition
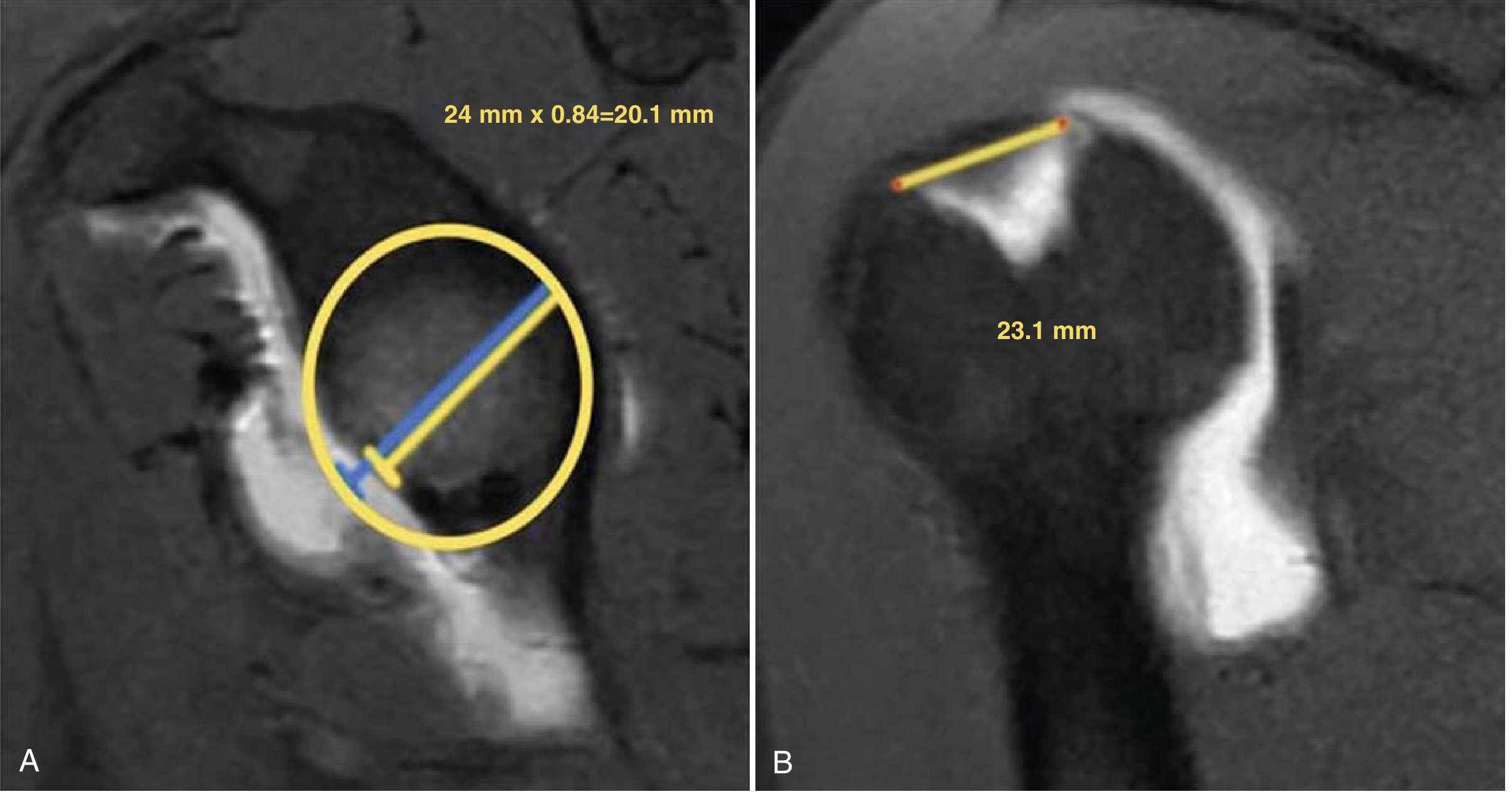
(A) Sagittal oblique MRI: best-fit circle on glenoid; glenoid track = 24 mm × 0.84 = 20.1 mm with 17% bone loss. (B) Coronal MRI: Hill-Sachs interval = 23.1 mm. Since HSI (23.1 mm) > GT (20.1 mm) → off-track lesion at high risk for engaging. (Miller's Review of Orthopaedics, 9th ed.)
6. Summary Algorithm
Plain XR (Stryker Notch, West Point, Bernageau)
↓
Suspected bone loss?
↓
3D CT with humeral subtraction ← primary quantification
+/- MRI/MRA (soft tissue, labrum, version)
↓
Measure glenoid bone loss (circle method)
↓
< 20% 20–25% > 25%
↓ ↓ ↓
Arthroscopic Borderline: Bony augmentation
Bankart repair glenoid track (Latarjet / bone graft)
analysis
↓
On-track → ABR
Off-track → ABR + remplissage or Latarjet
Sources:
- Rockwood and Green's Fractures in Adults, 10th ed., 2025 — Chapter 35
- Miller's Review of Orthopaedics, 9th ed. — Chapter 4, Anterior Instability
Forces acting on shoulder during anterior shoulder dislocation
Finding Sources
Finding Sources
Searching PubMed
"shoulder dislocation" AND biomechanics AND mechanism
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive content on mechanisms, forces, and stabilizers. I have everything needed to construct a thorough answer.
Forces Acting on the Shoulder During Anterior Glenohumeral Dislocation
1. Overview of Mechanism
Anterior dislocation accounts for >95% of all glenohumeral dislocations. It results when the combination of external forces and arm position overcomes the joint's passive and active stabilizers, driving the humeral head anteroinferiorly out of the glenoid fossa.
There are two principal mechanisms, both producing an anteriorly directed force vector on the humeral head:

(A) Fall onto a forward-flexed, externally rotated arm → anterior subluxation/dislocation. (B) Tackling with arm extended → posteriorly directed force on the humeral head → anterior dislocation. (C) Fall onto forward-flexed, internally rotated arm → posterior force vector → posterior dislocation. — Rockwood & Green's Fractures in Adults, 10th ed.
2. Primary Force Vectors
A. Indirect Force — Abduction + External Rotation (ABER)
The most common mechanism. The arm is placed in abduction (~90°) and external rotation (e.g., fall while diving, tackling with arm outstretched).
| Component | Effect |
|---|---|
| Abduction | Tightens the inferior glenohumeral ligament complex (IGHLC); shifts the humeral head toward the anteroinferior glenoid rim |
| External rotation | Rotates the posterior humeral head anteriorly; places the anterior capsule and IGHLC under maximal tension; unwinds the subscapularis |
| Combined ABER | Creates a lever-arm effect: the glenoid rim acts as a fulcrum, the humeral head is the load, and the externally rotated forearm/distal arm is the lever |
| Posterior-to-anterior directed force | Delivered through the outstretched hand or the opposing player's body, completing the dislocation vector |
In sport contexts (tackling/collision), an external posteriorly directed force applied to the posterior shoulder/arm during ABER directly translates the humeral head anteriorly out of the glenoid.
B. Direct Force — Fall onto Forward-Flexed, Externally Rotated Arm
When the hand contacts the ground first:
- The axial load transmits proximally up the shaft of the humerus
- The force vector is directed posteriorly relative to the humeral head — but because the arm is forward-flexed, this translates into an anterior displacement of the humeral head relative to the glenoid
- The subscapularis, anterior capsule, and IGHLC fail under the combined compressive + shear load
C. Non-contact / Muscular Imbalance Mechanisms
- Seizures and electrocution most commonly cause posterior dislocation (the stronger internal rotators — subscapularis, pectoralis major, anterior deltoid — overwhelm the weaker external rotators)
- Missed punches, sudden eccentric loads, or muscular imbalance can precipitate anterior subluxation/dislocation in hyperlax individuals at lower force thresholds
3. Forces That Must Be Overcome for Dislocation to Occur
Static Stabilizers (Passive Restraints)
| Stabilizer | Role | Failure in Anterior Dislocation |
|---|---|---|
| Inferior Glenohumeral Ligament Complex (IGHLC) — anterior band | Primary static restraint to anterior translation at ≥90° abduction | Torn (Bankart lesion) or avulsed from glenoid (bony Bankart) |
| Middle Glenohumeral Ligament (MGHL) | Resists anterior translation at 45–60° abduction | May be torn; more relevant in mid-range positions |
| Superior Glenohumeral Ligament (SGHL) | Limits inferior translation and external rotation at 0° abduction | Less relevant for traumatic anterior dislocation |
| Joint capsule | Provides a sealed volume (negative intraarticular pressure ~−4 mmHg) that resists distraction | Capsule tear eliminates the vacuum stabilizing effect |
| Glenoid labrum | Deepens the glenoid by ~50%; increases contact area and acts as a chock-block | Bankart lesion avulses it from the anteroinferior glenoid |
| Glenoid concavity | Congruency produces a compressive stabilizing reaction force | Bony erosion or glenoid bone loss reduces this force |
| Coracohumeral ligament | Limits inferior translation | Incidentally stretched |
Dynamic Stabilizers (Active Restraints)
| Stabilizer | Role | Failure |
|---|---|---|
| Subscapularis | Primary anterior muscular barrier; actively resists external rotation and anterior translation | Overwhelmed at maximum ER; HAGL lesion may occur with very high-energy events |
| Rotator cuff (overall) | Provides concavity-compression — compresses the humeral head into the glenoid to resist translation | Insufficient force to resist high-energy shear |
| Biceps long head | Assists anterior stability, especially at higher abduction | Contributes but not primary |
| Periscapular muscles | Maintain scapular position; orient the glenoid to maximize compressive reaction force | Scapular dyskinesia can reduce dynamic stabilization |
| Proprioceptive feedback | Allows anticipatory muscle activation to stiffen the joint | Overwhelmed at high velocity or during surprise loading |
4. Resultant Tissue Injuries from Force Transmission
The sequence of tissue failure during a traumatic anterior dislocation:
- Bankart lesion — avulsion of the anteroinferior capsulolabral complex from the glenoid rim (occurs in ~90% of recurrent instability)
- Bony Bankart — if force is sufficient, the attached glenoid rim fractures with the labrum (present in ~40% of first dislocations)
- Hill-Sachs lesion — impaction fracture of the posterosuperior humeral head against the hard anteroinferior glenoid rim as the head dislocates; occurs in ~90% after first dislocation and ~100% with recurrent dislocations
- Capsular distension/tear — stretching or frank tearing of the anterior capsule; HAGL (humeral avulsion of the glenohumeral ligament) occurs in 1–9% when the IGHLC avulses from the humerus rather than the glenoid
- ALPSA lesion — anterior labroligamentous periosteal sleeve avulsion; the capsulolabral complex strips medially with the intact periosteum (as opposed to the frank rupture of a Bankart lesion)
- Associated injuries (more common in older patients, up to 40%):
- Greater tuberosity fracture (most common, ~15% of older patients)
- Rotator cuff tear
- Axillary nerve palsy (susceptible due to its tethered position in the axilla)
- Brachial plexus injury
- Axillary artery injury (rare, high-energy)
5. Force Summary Diagram
ARM IN ABDUCTION + EXTERNAL ROTATION
↓
Posterior / axial force applied to arm or shoulder
↓
IGHLC anterior band → maximally tensioned
Subscapularis → overcome at extremes of ER
Labrum-glenoid interface → shear force exceeds attachment strength
↓
Humeral head levers over anteroinferior glenoid rim
↓
ANTERIOR DISLOCATION
├─ Bankart / bony Bankart (glenoid side)
├─ Hill-Sachs impaction (humeral side)
├─ Capsular tear / HAGL
└─ Axillary nerve / rotator cuff injury
Sources:
- Rockwood and Green's Fractures in Adults, 10th ed., 2025 — Mechanisms of Injury & Injuries Associated with Glenohumeral Instability
- Miller's Review of Orthopaedics, 9th ed. — Anterior Instability
Hill sachs index
Finding Sources
Finding Sources
Searching PubMed
"Hill-Sachs index" shoulder instability
Reading File
Searching PubMed
"Hill-Sachs index" depth width remplissage
Searching the Web
Hill-Sachs index calculation depth width length shoulder instability surgical decision
Searching PubMed
"Hill-Sachs" lesion size classification measurement CT humeral head
Reading File
Finding Sources
Reading Web Page
Hill-Sachs index quotient depth width length calculation classification
Searching PubMed
"Hill-Sachs" humeral head defect quantification articular surface
Loading Image
Searching PubMed
Provencher "Hill-Sachs" diagnosis classification management
Reading Article
I now have all the information needed. Let me compile a comprehensive answer on the Hill-Sachs Index and related quantification systems.
Hill-Sachs Index (Hill-Sachs Lesion Quantification)
The term "Hill-Sachs Index" (also called the Hill-Sachs Quotient) refers to a family of methods used to quantify the size of the Hill-Sachs lesion — the impaction fracture of the posterosuperior humeral head that occurs when the head dislocates anteriorly and strikes the hard anteroinferior glenoid rim.
1. Why Quantify the Hill-Sachs Lesion?
- Present in ~40% of first dislocations, ~90% after first true dislocation, approaching 100% with recurrent dislocations
- Average lesion size: 22 mm width × 5 mm depth
- Size directly correlates with number of dislocation events
- Determines whether the lesion is engaging (off-track) or non-engaging (on-track)
- Guides surgical decision-making: observation, remplissage, bone grafting, or arthroplasty
2. Imaging Modalities for Measurement
| Modality | Use |
|---|---|
| Plain X-ray (AP in 60° internal rotation / Stryker Notch) | Initial screening; measures width and depth |
| 2D CT | Reliable depth measurement; may underestimate width |
| 3D CT with humeral head reconstruction | Gold standard — best accuracy for volume, depth, width, and orientation |
| MRI / MRA | Comparable accuracy to 3D CT when using standardized methods |
3. Hill-Sachs Quotient (Kralinger Classification)
The most practical plain-radiograph-based index. Also referred to as the Hill-Sachs Index in many texts.
Measurement
- True AP radiograph with the arm in 60° internal rotation → measure:
- x = width of the lesion
- y = depth of the lesion
- Bernageau (glenoid profile) view → measure:
- z = length of the lesion
Formula
Hill-Sachs Quotient (HSQ) = x × y × z (in cm³)
Grading
| Grade | HSQ | Significance |
|---|---|---|
| Grade I | < 1.5 cm³ | Small — usually non-engaging |
| Grade II | 1.5–2.5 cm³ | Moderate — requires glenoid track analysis |
| Grade III | > 2.5 cm³ | Large — high risk of engagement |
4. Percentage of Articular Surface Involved
A simpler and widely used clinical metric. Critical thresholds:
| Parameter | Critical Value | Significance |
|---|---|---|
| % Articular surface area | > 20–25% | Significant; may require surgical address |
| Depth as % of humeral head diameter | > 16% | Associated with instability |
| Volume | > 250 mm³ (Voos) or > 1000 mm³ | Associated with recurrent instability |
| Radius involvement | > 5/8 of humeral head radius | Severe |
5. Rowe Classification (Descriptive — Axillary Projection)
One of the earliest size-based systems:
| Grade | Length | Depth |
|---|---|---|
| Mild | < 2 cm | < 0.3 cm |
| Moderate | 2–4 cm | 0.3–1 cm |
| Severe | > 4 cm | > 1 cm |
6. Calandra / Franceschi Classification (Arthroscopic)
Based on depth of involvement on direct visualization:
| Grade | Findings |
|---|---|
| Grade I | Articular cartilage defect only |
| Grade II | Extends into subchondral bone |
| Grade III | Significant loss of subchondral bone |
7. Glenoid Track / Hill-Sachs Interval (Most Clinically Important)
The Hill-Sachs Interval (HSI) is not strictly a "size" index but is the most surgically relevant measurement, integrating both glenoid and humeral bone loss.
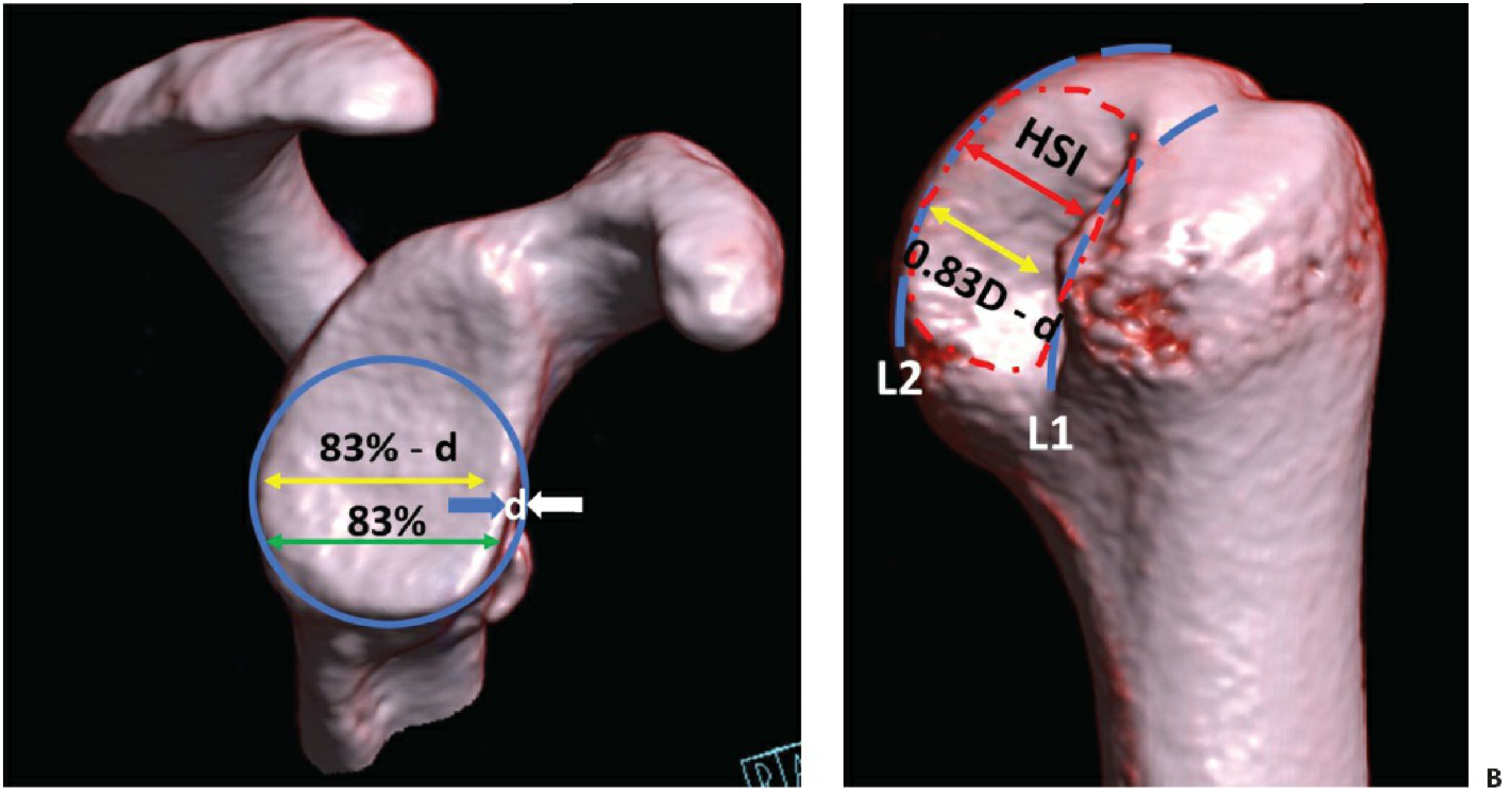
(A) En-face CT of the glenoid: Glenoid track = 0.83 × D (intact glenoid diameter). If glenoid bone loss (d) is present, true glenoid track = 0.83D − d. (B) Posterior view of the humeral head: HSI = distance from the lateral rotator cuff footprint to the medial margin of the Hill-Sachs lesion. — Rockwood & Green's Fractures in Adults, 10th ed.
Decision Rule
| Finding | Classification | Clinical Implication |
|---|---|---|
| HSI < 0.83D − d | On-track | No engagement risk → Bankart repair alone acceptable |
| HSI ≥ 0.83D − d | Off-track | Engagement risk → Remplissage or Latarjet required |
Two types of engaging Hill-Sachs lesions exist:
- Large, wide defect engaging in functional positions
- Narrow but medially located defect — engages due to proximity to glenoid rim
8. Summary: Which Index to Use?
| Clinical Scenario | Preferred Index |
|---|---|
| Initial screening / emergency | Rowe classification on plain X-ray |
| Pre-operative planning | 3D CT → % articular surface + Glenoid Track / HSI |
| Determining surgical approach | Glenoid Track / HSI (on-track vs. off-track) |
| Volume-based research | Hill-Sachs Quotient (x × y × z) |
| Arthroscopic intraoperative | Calandra/Franceschi grade |
Sources:
- Rockwood & Green's Fractures in Adults, 10th ed., 2025 — Evaluation of the Hill-Sachs Lesion
- Provencher MT et al. "The Hill-Sachs lesion: diagnosis, classification, and management." J Am Acad Orthop Surg 2012 [PMID: 22474094]
- Kralinger et al. — Hill-Sachs Quotient grading system
- Open Orthopaedics Journal — Management of Humeral Defects in Anterior Shoulder Instability, 2017
This is a shared conversation. Sign in to Orris to start your own chat.