Nephrotic syndrome and nephrotic syndrome
Reading File
Finding Sources
Finding Sources
Searching PubMed
"nephrotic syndrome"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have rich, comprehensive information from multiple authoritative textbooks. Let me compile the full response.
Nephrotic Syndrome - Comprehensive Overview
Definition
Nephrotic syndrome is defined by the tetrad of:
- Proteinuria >3.5 g/24 hours (nephrotic range)
- Hypoalbuminemia (serum albumin <3.5 g/dL; practically <2.5 g/dL in most criteria)
- Edema (pitting peripheral edema, often anasarca)
- Hyperlipidemia (total cholesterol usually >180 mg/dL)
The spot urine protein:creatinine ratio can reliably estimate 24-hour proteinuria without a timed collection.
- National Kidney Foundation Primer on Kidney Diseases, 8e, p. 190
- Frameworks for Internal Medicine, p. 464
Pathophysiology
Glomerular Filtration Barrier Disruption
Normal glomerular permeability is maintained by three structures working together:
- Fenestrated endothelial cells - with their glycocalyx providing a charge barrier
- Glomerular basement membrane (GBM) - a collagen IV scaffold rich in heparan sulfate proteoglycans (anionic, repels albumin)
- Podocytes - specialized epithelial cells with interdigitating foot processes bridged by the slit diaphragm, composed mainly of nephrin and podocin
In nephrotic syndrome, impairment of charge and/or size selectivity - primarily through podocyte injury and foot process effacement - allows large anionic molecules like albumin (70 kDa) to escape into the urine.
A consistent morphologic finding in all causes of nephrotic syndrome is fusion/effacement of epithelial foot processes on electron microscopy, though it is debated whether this is a cause or effect of proteinuria.
- Robbins & Kumar Basic Pathology, p. 452-453
Edema Mechanism: "Underfill" vs. "Overfill"
Two competing mechanisms explain edema formation:
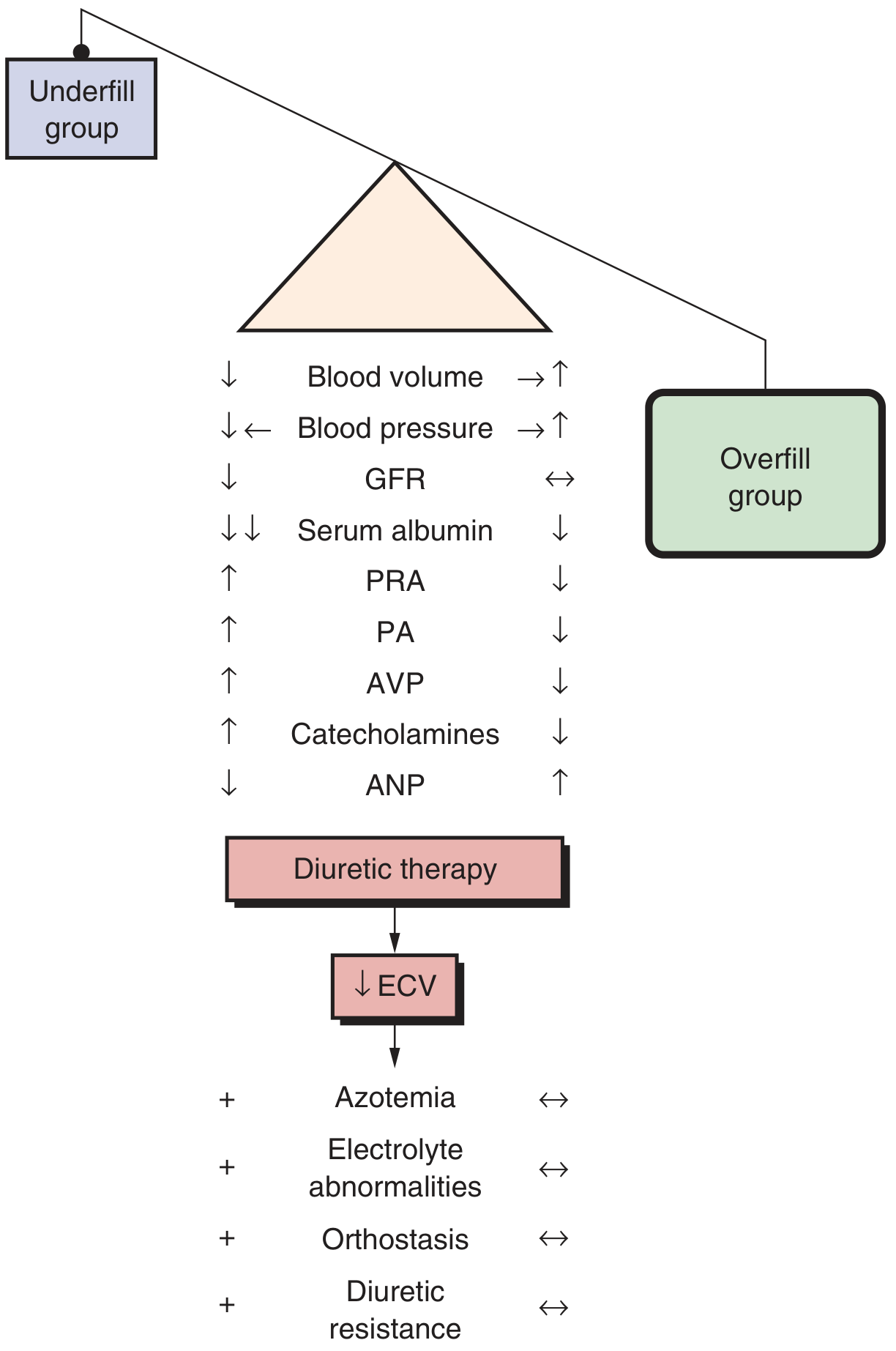
| Parameter | Underfill Group | Overfill Group |
|---|---|---|
| Blood volume | Decreased | Increased |
| Blood pressure | Decreased | Increased |
| Plasma renin (PRA) | Increased | Decreased |
| Plasma aldosterone (PA) | Increased | Decreased |
| ANP | Decreased | Increased |
| Typical disease | Minimal change disease | Most other NS |
- Underfill: Loss of albumin reduces plasma oncotic pressure → fluid shifts to interstitium → intravascular volume contraction → RAAS activation → sodium/water retention
- Overfill (more common): Primary distal tubular sodium retention occurs independently of the RAAS, driving volume expansion
Patients with minimal change disease predominantly have the underfill pattern, while those with other causes of NS (FSGS, membranous nephropathy) more often have an overfill/expanded plasma volume.
- Brenner and Rector's The Kidney, p. 2277
Classification of Causes

Primary (Idiopathic) Causes - Incidence in Adults
| Subtype | Incidence in Adults |
|---|---|
| Membranous nephropathy | 25-30% |
| Focal segmental glomerulosclerosis (FSGS) | 20-25% |
| Other proliferative/sclerosing GN | 15-30% |
| Minimal change disease | 5-10% |
| Membranoproliferative GN | ~5% |
- Goldman-Cecil Medicine, Table 107-2
Secondary Causes
| Category | Examples |
|---|---|
| Systemic diseases | Diabetes mellitus (most common overall), SLE, amyloidosis (AA/AL) |
| Infections | Hepatitis B, Hepatitis C, HIV, malaria, syphilis, CMV |
| Medications | Gold, mercury, penicillamine, NSAIDs/COX-2 inhibitors, lithium, heroin, pamidronate |
| Malignancies | Hodgkin lymphoma (classically MCD pattern), solid tumors (membranous pattern) |
| Hereditary/metabolic | Alport syndrome, Fabry disease, sickle cell, APOL1 variants, podocyte gene mutations |
| Other | Preeclampsia, obesity-related glomerulopathy, renal artery stenosis, reflux |
- Goldman-Cecil Medicine, Table 107-3
Major Disease Entities
1. Minimal Change Disease (MCD)
- Accounts for >70-90% of nephrotic syndrome in children but only ~5-10% in adults
- Pathogenesis is unknown; associations with NSAID use, Hodgkin lymphoma, and thymoma suggest a T-cell-mediated mechanism
- Light microscopy: Normal (hence the name - "minimal changes")
- Electron microscopy: Diffuse foot process effacement
- Immunofluorescence: Negative
- In children with pure nephrotic syndrome (no hematuria, normal GFR), MCD is presumed and biopsy is not routinely required; adults require biopsy
- Treatment: Corticosteroids are the cornerstone; anti-CD20 monoclonal antibodies (rituximab) for steroid-resistant/dependent cases
- Underfill edema pattern; RAAS activated
2. Focal Segmental Glomerulosclerosis (FSGS)
- Focal (only some glomeruli affected) and segmental (only part of the affected glomerulus scarred) on light microscopy, but EM shows foot process effacement even in "unaffected" glomeruli
- ~25% of adult nephrotic syndrome; most common cause among African-Americans (linked to APOL1 risk variants)
- Presents with nephrotic-range proteinuria, often with hypertension, reduced GFR, and microscopic hematuria
- Classification:
- Primary FSGS: Circulating podocyte permeability factor; >80% foot process effacement on EM; abrupt onset
- Secondary FSGS: Viral (HIV, parvovirus B19, COVID-19), drugs (heroin, pamidronate, interferon, anabolic steroids), adaptive (obesity, reduced nephron mass); <80% foot process effacement
- Genetic FSGS: Mutations in NPHS1 (nephrin), NPHS2 (podocin), PLCE1, ACTN4, INF2, APOL1
- Collapsing FSGS (a variant): Strongly associated with HIV; presents with abrupt, severe nephrotic syndrome and rapidly progressive renal failure
- Treatment: Corticosteroids for primary FSGS; addressing the underlying cause for secondary
3. Membranous Nephropathy (MN)
- Most common cause of nephrotic syndrome in White adults (25-30%)
- More frequently associated with thromboembolism than other causes, especially renal vein thrombosis (particularly with severe proteinuria >10 g/24hr and albumin <2 g/dL)
- Pathogenesis: Subepithelial immune complex deposition with in situ antibody-antigen reactions
- Key antigens:
- PLA2R (M-type phospholipase A2 receptor) - primary MN
- THSD7A - primary MN and malignancy-associated
- NELL-1 - primary MN and malignancy-associated
- EXT1/2 - autoimmunity (SLE)
- Semaphorin 3b - younger/pediatric patients
- Secondary causes: SLE, hepatitis B, penicillamine, solid tumors (colon cancer, lung)
- Light microscopy: Thickening of GBM with "spike and dome" pattern (silver stain)
- EM: Subepithelial dense deposits with podocyte effacement
- IF: Granular IgG + C3 deposits along GBM
- Treatment: Observation for partial remission, then immunosuppression (cyclophosphamide + steroids, or rituximab) for high-risk patients
4. Membranoproliferative Glomerulonephritis (MPGN)
- ~5% of nephrotic syndrome; can present as nephrotic, nephritic, or mixed syndrome
- Two main mechanisms:
- Immune complex-mediated (hepatitis B/C, autoimmune diseases)
- Complement-mediated (C3 glomerulopathy, dense deposit disease)
- Light microscopy: "Tram track" appearance (GBM duplication/splitting) due to mesangial interposition
Clinical Features
Symptoms
- Peripheral edema (often progressing to anasarca)
- Periorbital edema (classically prominent on awakening)
- Fatigue, dyspnea
- Foamy urine (surfactant effect of protein in urine)
- Weight gain
Physical Signs
- Hypertension
- Generalized dependent pitting edema
- Ascites, pleural effusions
- Muehrcke's lines (paired white transverse lines on nails, from hypoalbuminemia)
- Eruptive xanthomata, xanthelasma (from hyperlipidemia)
Complications
1. Hypercoagulability / Thromboembolism
Urinary loss of:
- Antithrombin III (major)
- Protein C and Protein S
- Plasminogen
Combined with increased hepatic synthesis of procoagulant factors (fibrinogen, factor V, factor VIII) and platelet activation.
Most common sites: renal veins and lower extremity deep veins. Pulmonary embolism is a feared complication. Risk is highest in membranous nephropathy and amyloidosis.
2. Infection
- Loss of IgG in urine leads to hypogammaglobulinemia
- Reduced complement activity (loss of Factor B/D)
- Impaired T-cell function
- Increased susceptibility to encapsulated organisms (Streptococcus pneumoniae, Haemophilus influenzae) - spontaneous bacterial peritonitis in ascites is a classic complication
3. Hyperlipidemia
- Low oncotic pressure upregulates hepatic apolipoprotein synthesis
- Elevated total cholesterol, LDL, VLDL, lipoprotein(a); low or normal HDL
- Increased risk of atherosclerotic cardiovascular disease
- Lipiduria ("fatty casts," oval fat bodies, Maltese cross pattern under polarized light)
4. Nutritional Deficiencies
- Iron deficiency anemia - loss of transferrin
- Vitamin D deficiency - loss of vitamin D-binding protein (leading to hypocalcemia, secondary hyperparathyroidism)
- Hypothyroidism - loss of thyroid-binding globulin
- Zinc deficiency - loss of zinc-binding proteins
5. Acute Kidney Injury
- Due to reduced effective circulating volume (underfill)
- Thrombosis
- Tubular toxicity from heavy proteinuria
Diagnosis
Laboratory Workup
| Test | Finding in NS |
|---|---|
| Urine protein (24h or spot P:Cr) | >3.5 g/day |
| Serum albumin | <3.5 g/dL |
| Lipid panel | High LDL/total cholesterol, low HDL |
| Urine microscopy | Oval fat bodies, fatty casts, Maltese cross; lipiduria |
| Serum creatinine | Variable |
Screening for secondary causes:
- Fasting glucose + HbA1c (diabetes)
- ANA, anti-dsDNA, complement levels (SLE)
- Hepatitis B surface antigen, Hepatitis C antibody
- HIV serology
- SPEP/immunofixation (myeloma, amyloid)
- Anti-PLA2R antibody (primary membranous)
- ANCA, anti-GBM (if nephritic features also present)
- Low complement (C3, C4) suggests immune complex-mediated disease
Kidney Biopsy
- Required in adults with nephrotic syndrome unless diabetes is a clear underlying cause
- Guides specific diagnosis, prognosis, and therapy
- Not routinely needed in children (<12 years) presenting with pure nephrotic syndrome (presumed MCD; treat empirically with steroids)
- Processing: light microscopy (H&E, PAS, Masson trichrome, silver stain), immunofluorescence, and electron microscopy are all needed for complete evaluation
Management
General (Non-Disease-Specific) Measures
| Intervention | Rationale |
|---|---|
| Low-salt diet | Reduce edema |
| Protein restriction (0.8-1 g/kg/day) | Reduce proteinuria, slow progression |
| ACE inhibitor or ARB | Reduce intraglomerular pressure and proteinuria; also combat coagulopathy, dyslipidemia, and slow progression |
| Loop diuretics (furosemide) | Treat edema; note: hypoalbuminemia reduces furosemide binding and enlarge its volume of distribution; may need combination with thiazide for resistant edema |
| Statins | Treat hyperlipidemia, reduce cardiovascular risk |
| Anticoagulation | For high-risk patients (membranous nephropathy with severe hypoalbuminemia; documented thrombus) |
Important notes on diuretic resistance:
- Furosemide is highly protein-bound; in hypoalbuminemia, delivery to the tubular lumen is impaired
- Albumin infusion to "pre-mix" with furosemide has NOT been confirmed to reliably enhance diuresis and is not generally recommended
- Adding ACE inhibitor/ARB to reduce proteinuria is a more rational approach to diuretic resistance
Disease-Specific Treatment
| Disease | First-line | Second-line / Steroid-Resistant |
|---|---|---|
| MCD (children) | Corticosteroids | Cyclosporine A, tacrolimus, rituximab, mycophenolate |
| MCD (adults) | Corticosteroids | Rituximab, cyclosporine |
| Primary FSGS | Corticosteroids | Calcineurin inhibitors, rituximab |
| Primary membranous nephropathy | Observation (partial remission) or Cyclophosphamide + steroid | Rituximab (now preferred) |
| Diabetic nephropathy | RAAS blockade, SGLT2 inhibitors | - |
Nephrotic vs. Nephritic Syndrome: Key Distinction
| Feature | Nephrotic | Nephritic |
|---|---|---|
| Proteinuria | >3.5 g/day (heavy) | <3.5 g/day (mild-moderate) |
| Hematuria | Absent or minimal | Present (dysmorphic RBCs, RBC casts) |
| Edema | Severe (anasarca) | Mild-moderate |
| Hypertension | Variable | Common |
| GFR | Usually preserved (early) | Often reduced |
| Mechanism | Permeability defect (podocyte) | Inflammatory injury |
Some diseases can present with overlap (nephrotic-nephritic syndrome): MPGN, lupus nephritis, and advanced FSGS.
Recent Evidence
A 2025 Cochrane review [PMID: 40337980] evaluated interventions for idiopathic steroid-resistant nephrotic syndrome in children, and a 2025 meta-analysis [PMID: 40849613] assessed urinary NGAL as a biomarker to distinguish steroid-resistant from steroid-sensitive NS. A 2024 systematic review [PMID: 38965515] described NS associated with solid malignancies. These recent studies reinforce that steroid resistance identification and targeted therapy remain active areas of research but do not substantially alter the foundational management framework described above.
Sources:
- Frameworks for Internal Medicine, pp. 463-466
- National Kidney Foundation Primer on Kidney Diseases, 8e, pp. 190-196
- Goldman-Cecil Medicine, Tables 107-2 and 107-3
- Brenner and Rector's The Kidney, p. 2277
- Robbins & Kumar Basic Pathology, pp. 452-458
This is a shared conversation. Sign in to Orris to start your own chat.