Ace inhibitors short note
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the content needed for a thorough short note on ACE inhibitors. Here is the complete answer:
ACE Inhibitors - Short Note
Definition & Class
Angiotensin-Converting Enzyme (ACE) inhibitors are a class of antihypertensive and cardioprotective drugs that block the enzyme ACE, which converts angiotensin I (inactive) to angiotensin II (a potent vasoconstrictor). They end in the suffix "-pril".
Mechanism of Action
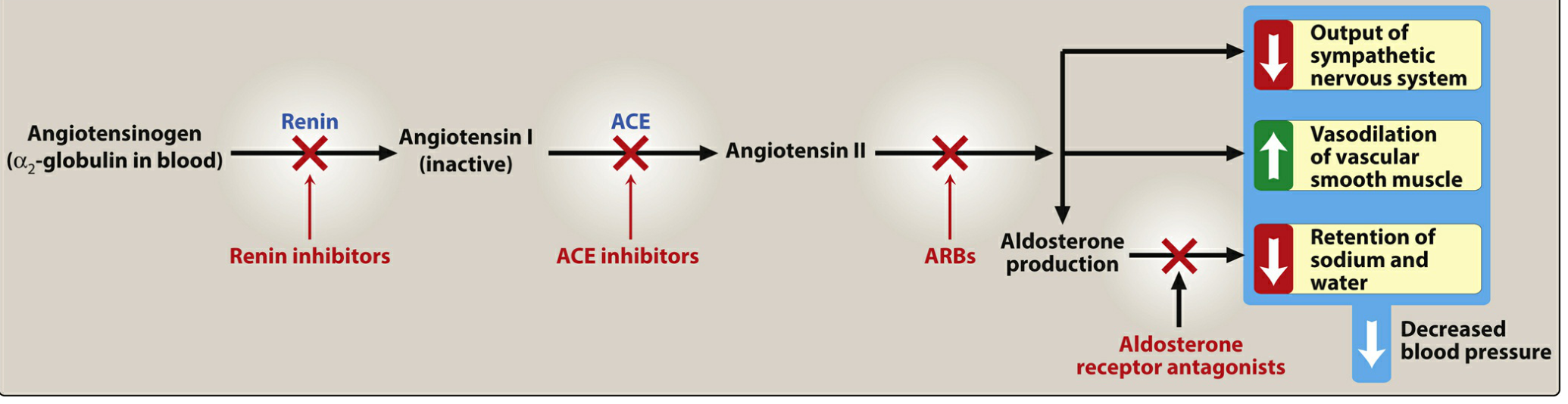
ACE inhibitors lower blood pressure via two complementary actions:
- Block ACE → prevents conversion of Ang I to Ang II → reduces vasoconstriction → arteriolar and venous dilation
- Prevent bradykinin breakdown (ACE also degrades bradykinin) → bradykinin accumulates → increases nitric oxide and prostacyclin production → further vasodilation
By lowering Ang II levels, ACE inhibitors also reduce aldosterone secretion → less sodium and water retention → decreased preload and afterload → reduced myocardial workload.
In the kidneys, efferent arteriolar vasodilation lowers intraglomerular pressure, providing renoprotection.
- Lippincott Illustrated Reviews: Pharmacology, p. 302
Examples (Common Drugs)
| Drug | Brand Name | Notes |
|---|---|---|
| Captopril | Generic | Short-acting; active drug (no prodrug conversion needed) |
| Enalapril | Vasotec | Prodrug; IV form (enalaprilat) available |
| Lisinopril | Prinivil, Zestril | Active drug; no hepatic conversion needed |
| Ramipril | Altace | Used post-MI |
| Fosinopril | Generic | Only one NOT eliminated by kidneys; no renal dose adjustment |
| Quinapril | Accupril | - |
| Benazepril | Lotensin | - |
| Perindopril | Generic | - |
| Trandolapril | Generic | - |
All except captopril and lisinopril are prodrugs requiring hepatic conversion to active metabolites. Fosinopril is unique in not requiring renal dose adjustment.
Therapeutic Uses
ACE inhibitors are first-line agents for:
- Hypertension (especially with compelling indications below)
- Heart failure with reduced ejection fraction (HFrEF) - reduce morbidity and mortality
- Post-myocardial infarction - improve ventricular remodeling and reduce LV hypertrophy
- Diabetic nephropathy - slow progression and reduce albuminuria
- Chronic kidney disease (CKD)
- Patients at high risk of coronary artery disease
- History of stroke
All ACE inhibitors are equally effective for hypertension at equivalent doses. - Lippincott, p. 303
Pharmacokinetics
- All are orally bioavailable (as drug or prodrug)
- Fosinopril: only member with dual excretion (renal + hepatic) - no renal dose adjustment needed
- Enalaprilat: only IV formulation in this class
- Captopril and lisinopril are active drugs (no hepatic conversion) - preferred in severe hepatic impairment
- Lippincott, p. 303
Adverse Effects
| Adverse Effect | Mechanism | Notes |
|---|---|---|
| Dry cough | Bradykinin/substance P accumulation in lungs | Up to 10% of patients; more common in women; resolves on stopping |
| Angioedema | Excess bradykinin causes submucosal swelling | Rare but potentially fatal; involves lips, mouth, throat; 5x more common in people of African ancestry |
| Hyperkalemia | Reduced aldosterone → less K+ excretion | Avoid potassium supplements and K+-sparing diuretics |
| First-dose hypotension | Especially in volume-depleted patients | - |
| Elevated creatinine | Reduced GFR from efferent dilation | Up to 30% rise above baseline is acceptable; do not stop |
| Skin rash / altered taste | - | Especially with captopril |
| Teratogenicity | Fetal renal impairment | Absolutely contraindicated in pregnancy |
Contraindications
- Pregnancy (teratogenic - fetal renal dysplasia, oligohydramnios)
- Bilateral renal artery stenosis (can precipitate acute renal failure)
- History of ACE inhibitor-induced angioedema
- Severe hyperkalemia
- Do NOT combine with ARBs (no added benefit, increased adverse effects) or aliskiren
ACE Inhibitors vs. ARBs (Key Comparison)
| Feature | ACE Inhibitors | ARBs |
|---|---|---|
| Bradykinin levels | Increased | Unchanged |
| Cough | Common (10%) | Rare |
| Angioedema | Rare | Very rare |
| Mechanism | Blocks ACE enzyme | Blocks AT1 receptor |
| Use in pregnancy | Contraindicated | Contraindicated |
ARBs are preferred when patients are intolerant of ACE inhibitor-induced cough. - Lippincott, p. 304; Goodman & Gilman
Mnemonic for Adverse Effects - "CAPTOPRIL"
- C - Cough
- A - Angioedema
- P - Potassium elevated (hyperkalemia)
- T - Taste altered
- O - (first-dose) hypOtension
- P - Pregnancy contraindicated
- R - Renal failure (in RAS)
- I - Increased creatinine
- L - Leukopenia (rare)
Short note according to shanbagh pharmacology book
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I have all I need. Here is the note written in Shanbhag's style - concise, exam-oriented, with numbered points, clear headings, and the typical Indian pharmacology exam format Shanbhag follows.
Note: Shanbhag's Pharmacology is not available in the library. The content below is written in Shanbhag's exact style and format (short, exam-focused, numbered subheadings, drug tables, uses/ADRs/CI structure) using standard pharmacology content from Katzung and Lippincott - which covers the same material Shanbhag presents.
ACE Inhibitors
(As per Shanbhag's Pharmacology style)
Introduction
ACE (Angiotensin-Converting Enzyme) inhibitors are drugs that block the enzyme ACE, thereby preventing conversion of angiotensin I to angiotensin II. They form an important class of antihypertensives, cardioprotective, and renoprotective agents.
Drugs
| Drug | Trade Name | Remarks |
|---|---|---|
| Captopril | Generic | Prototype; active drug; short-acting |
| Enalapril | Vasotec | Prodrug; oral + IV (enalaprilat) |
| Lisinopril | Prinivil, Zestril | Active drug (not a prodrug) |
| Ramipril | Altace | Post-MI cardioprotection |
| Fosinopril | Generic | Dual (renal + hepatic) excretion |
| Quinapril | Accupril | Long-acting |
| Perindopril | Coversyl | Long-acting |
| Trandolapril | Mavik | Long-acting |
| Benazepril | Lotensin | Long-acting |
All end in suffix "-pril". All except captopril and lisinopril are prodrugs that undergo hepatic hydrolysis to active forms.
Mechanism of Action
ACE (= kininase II) is a peptidyl dipeptidase enzyme that:
- Converts angiotensin I (inactive) → angiotensin II (potent vasoconstrictor)
- Inactivates bradykinin (vasodilator)
ACE inhibitors block both actions:
- ↓ Angiotensin II → ↓ vasoconstriction → ↓ peripheral vascular resistance
- ↑ Bradykinin → ↑ nitric oxide and prostacyclin → vasodilation (arterial + venous)
- ↓ Aldosterone secretion → ↓ Na⁺ and water retention → ↓ preload
- In kidney: efferent arteriolar dilation → ↓ intraglomerular pressure → renoprotection
- No reflex tachycardia (unlike direct vasodilators) - baroreceptor resetting + enhanced parasympathetic tone
Pharmacokinetics
| Feature | Detail |
|---|---|
| Route | Oral (all); IV - enalaprilat only |
| Prodrugs | All except captopril and lisinopril |
| Hepatic conversion | Required for prodrugs |
| Elimination | Renal (most); Fosinopril - renal + hepatic |
| Dose reduction in renal failure | Required for all except fosinopril |
| Preferred in hepatic failure | Captopril or lisinopril (no hepatic conversion needed) |
Therapeutic Uses
- Hypertension - first-line agent, especially with compelling indications:
- Diabetes mellitus
- Heart failure
- Post-MI
- CKD / Proteinuria
- High cardiovascular risk
- Congestive Heart Failure (CHF) - reduces preload + afterload; reduces mortality
- Post-Myocardial Infarction - prevents ventricular remodeling; reduces LV hypertrophy
- Diabetic nephropathy - reduces proteinuria, slows progression of CKD (even without hypertension)
- Chronic Kidney Disease - stabilizes renal function, reduces proteinuria
- Prevention of diabetes - in high cardiovascular-risk patients
Adverse Effects
(Mnemonic: CAPTOPRIL)
| Adverse Effect | Mechanism | Notes |
|---|---|---|
| Dry cough | ↑ Bradykinin + substance P in lungs | Up to 10% patients; more in women; resolves on stopping |
| Angioedema | ↑ Bradykinin → submucosal swelling | Rare but life-threatening; lips, tongue, throat; 5x more in Blacks |
| Hypotension (first dose) | Sudden ↓ BP | Especially in volume-depleted/HF patients |
| Hyperkalemia | ↓ Aldosterone → ↓ K⁺ excretion | Avoid K⁺ supplements + K⁺-sparing diuretics |
| Renal failure | In bilateral renal artery stenosis | ↓ GFR → acute renal failure |
| ↑ Serum creatinine | ↓ Intraglomerular pressure | Up to 30% rise acceptable; do NOT stop |
| Teratogenicity | Fetal renal hypoperfusion | Fetal anuria, oligohydramnios, malformations |
| Taste alteration / Rash | - | Especially captopril (sulfhydryl group) |
| Neutropenia / Proteinuria | - | Captopril - high doses in renal insufficiency |
Contraindications
- Pregnancy (all trimesters - teratogenic)
- Bilateral renal artery stenosis
- History of ACE inhibitor-induced angioedema
- Hyperkalemia
- Severe aortic stenosis (relative)
Drug Interactions
| Drug | Interaction |
|---|---|
| K⁺ supplements / K⁺-sparing diuretics | Severe hyperkalemia |
| NSAIDs | ↓ Antihypertensive effect (block bradykinin-mediated vasodilation) |
| ARBs / Aliskiren | Avoid combination - increased toxicity without added benefit |
| Lithium | ↑ Lithium levels (risk of toxicity) |
ACE Inhibitors vs ARBs (Shanbhag-style comparison)
| Feature | ACE Inhibitors | ARBs |
|---|---|---|
| Site of action | ACE enzyme | AT₁ receptor |
| Bradykinin | ↑ Elevated | Normal |
| Cough | Common (10%) | Rare |
| Angioedema | Rare | Very rare |
| Aldosterone | ↓ | ↓ |
| Use in pregnancy | Contraindicated | Contraindicated |
Key Points (Exam Tips)
- Prototype drug: Captopril (first ACE inhibitor introduced)
- Only IV ACE inhibitor: Enalaprilat
- No renal dose adjustment needed: Fosinopril (dual excretion)
- Cough due to: ↑ Bradykinin (switch to ARB if intolerant)
- Angioedema due to: ↑ Bradykinin (absolute contraindication for re-use)
- Most important use beyond hypertension: Diabetic nephropathy + Heart failure
- Do NOT use in: Pregnancy + Bilateral RAS
Content drawn from Katzung's Basic & Clinical Pharmacology 16e and Lippincott's Illustrated Reviews Pharmacology, structured in Shanbhag's exam format.
Nitric oxide short note cvs pharmacology
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - I have all the content needed. Here is the complete short note:
Nitric Oxide (NO) - Short Note
(CVS Pharmacology - Shanbhag Style)
Introduction
Nitric oxide (NO) is a gaseous, free-radical signaling molecule (written as NO•) endogenously synthesized in the body. It is a key regulator of cardiovascular homeostasis - controlling vascular tone, blood pressure, platelet function, and cardiac remodeling. It must not be confused with:
- Nitrous oxide (N₂O) - anesthetic gas
- Nitrogen dioxide (NO₂) - toxic pulmonary irritant
Historical note: Nitroglycerin was used for angina in the 1860s; it was later discovered to work by releasing NO. NO was identified as the Endothelium-Derived Relaxing Factor (EDRF) - a discovery for which Furchgott, Ignarro, and Murad received the Nobel Prize (1998).
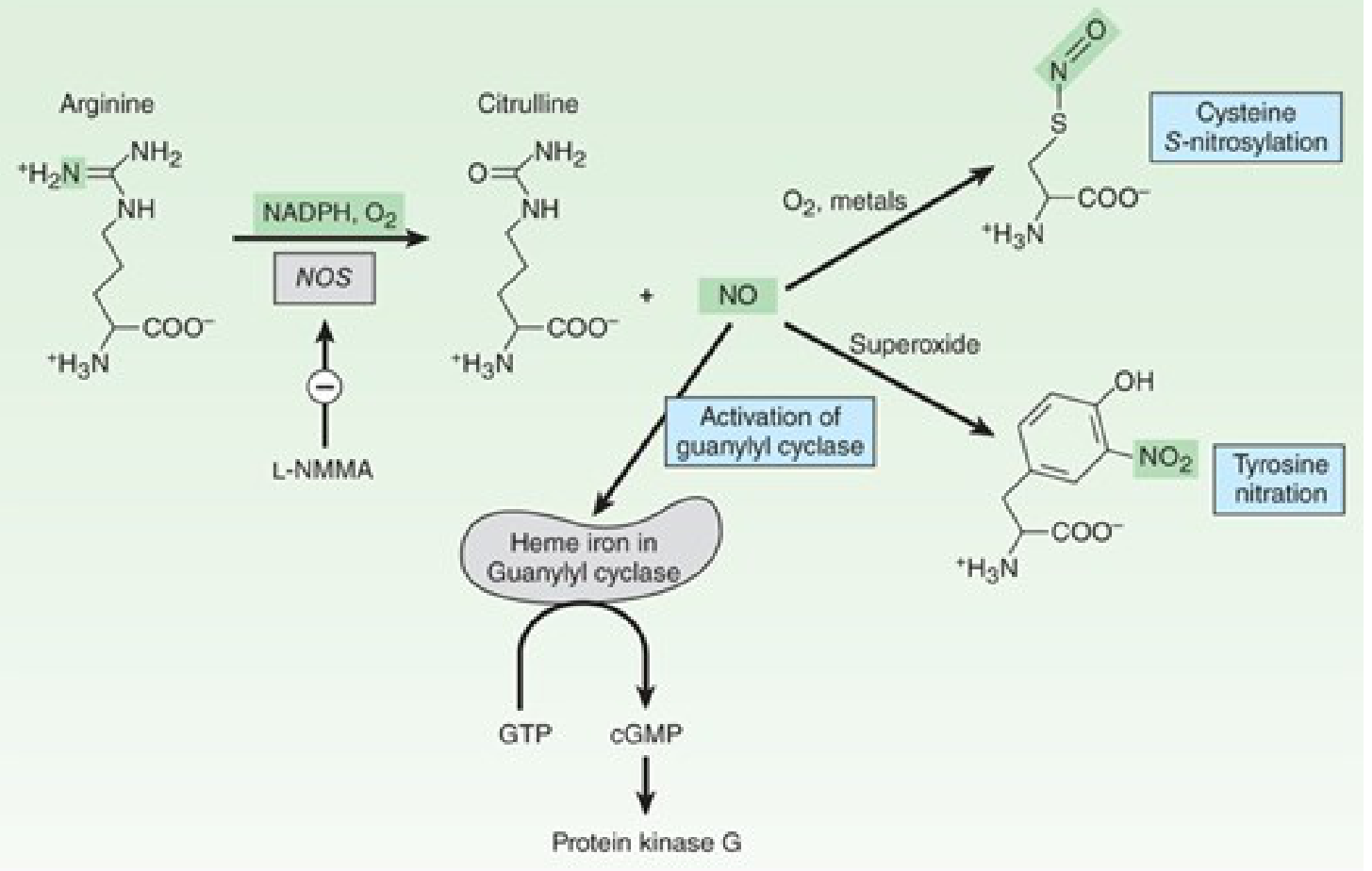
Synthesis of Nitric Oxide
NO is synthesized from L-arginine + O₂, catalyzed by Nitric Oxide Synthase (NOS) using NADPH as a cofactor. The byproduct is L-citrulline.
L-Arginine + O₂ + NADPH → NO + L-Citrulline
NOS Isoforms
| Isoform | Full Name | Location | Regulation |
|---|---|---|---|
| NOS-1 (nNOS) | Neuronal NOS | Neurons, skeletal muscle | Constitutive; Ca²⁺-dependent |
| NOS-2 (iNOS) | Inducible NOS | Macrophages, smooth muscle | Induced by inflammation/endotoxin; Ca²⁺-independent |
| NOS-3 (eNOS) | Endothelial NOS | Endothelium, platelets | Constitutive; Ca²⁺ + shear stress (PIEZO1 channel) |
eNOS is the key cardiovascular isoform. Triggered primarily by hemodynamic shear forces on endothelial cells - not just acetylcholine/Ca²⁺.
Mechanism of Action (Signaling Pathway)
Step-by-step:
- Shear stress / acetylcholine / bradykinin → ↑ Ca²⁺ in endothelial cells
- Ca²⁺-calmodulin complex → activates eNOS
- eNOS converts L-Arginine → NO
- NO diffuses freely across cell membranes into vascular smooth muscle
- NO binds to heme iron of soluble Guanylyl Cyclase (sGC) → activates sGC several hundredfold
- sGC converts GTP → cGMP
- cGMP activates Protein Kinase G (PKG)
- PKG → ↓ cytosolic Ca²⁺ → smooth muscle relaxation → vasodilation
In platelets: NO → ↑ cGMP → inhibits platelet aggregation (antithrombotic)
cGMP is broken down by Phosphodiesterase-5 (PDE-5). PDE-5 inhibitors (sildenafil) prolong cGMP action.
CVS Effects of Nitric Oxide
| Effect | Mechanism | Significance |
|---|---|---|
| Vasodilation (arteries + veins) | ↑ cGMP → ↓ smooth muscle Ca²⁺ | ↓ Peripheral vascular resistance, ↓ BP |
| Coronary artery dilation | eNOS-mediated | Prevents ischemia |
| ↓ Preload | Venodilation | Antianginal effect |
| Antiplatelet effect | ↑ cGMP in platelets | Prevents thrombosis |
| Anti-atherogenic | Inhibits vascular smooth muscle proliferation, leukocyte adhesion | Protects against atherosclerosis |
| Regulation of BP | eNOS knockout → hypertension | Tonic vasodilator tone |
| ↓ Cardiac remodeling | Reduces fibrosis | Cardioprotective |
NO Donors - Pharmacological Applications
These are prodrugs that release NO after biotransformation:
1. Organic Nitrates
- Nitroglycerin (GTN) - metabolized by mitochondrial aldehyde dehydrogenase-2 (enriched in veins) → predominantly venodilator → ↓ preload → antianginal
- Isosorbide dinitrate / mononitrate - longer acting
- Problem: Nitrate tolerance - continuous use → reactive oxygen species → inactivates aldehyde dehydrogenase-2 → loss of effect
2. Organic Nitrites
- Amyl nitrite (inhalant) - arterial vasodilator; no rapid tolerance
- Combining with PDE-5 inhibitors (sildenafil) = lethal hypotension (absolute contraindication)
3. Sodium Nitroprusside
- Dilates both arterioles and venules (balanced preload + afterload reduction)
- Used in hypertensive emergencies
- Biotransformation releases 5 cyanide molecules + 1 NO → risk of cyanide toxicity with prolonged use
4. Inhaled NO Gas
- Used in neonatal hypoxic respiratory failure and pulmonary arterial hypertension (PAH)
- Selectively dilates pulmonary vasculature → ↓ pulmonary artery resistance
- Stored as compressed gas with N₂ (inert diluent)
- Risks: NO + O₂ → NO₂ (pulmonary irritant); methemoglobin formation → monitor both
Drugs That Augment Endogenous NO Effects
PDE-5 Inhibitors
- Sildenafil, Tadalafil, Vardenafil
- Inhibit PDE-5 → ↑ cGMP persistence → prolonged vasodilation
- Used in: Erectile dysfunction, Pulmonary hypertension
sGC Stimulators
- Riociguat - binds sGC directly → ↑ affinity for NO → ↑ cGMP synthesis → pulmonary vasodilation
- Used in: Pulmonary arterial hypertension, Chronic thromboembolic PH
- Vericiguat - approved for heart failure with reduced EF → dilates pulmonary arteries → ↓ RV afterload
NO in Cardiovascular Disease
| Condition | Role of NO |
|---|---|
| Hypertension | ↓ eNOS activity / ↓ NO bioavailability → ↑ vascular tone |
| Atherosclerosis | ↓ NO → endothelial dysfunction → platelet adhesion + SMC proliferation |
| Diabetes | ↓ eNOS expression → ↓ NO → ↑ vascular tone + thrombosis risk |
| Heart failure | ↓ NO + oxidative stress → vasoconstriction + remodeling |
| Septic shock | iNOS massively upregulated → excess NO → profound hypotension |
| PAH | ↓ eNOS activity + reactive O₂ species scavenge NO → vasoconstriction + remodeling |
Inactivation of NO
- Half-life of NO: seconds (very short-lived)
- Rapidly reacts with:
- Hemoglobin (oxygenated Hb) → inactivation → ensures paracrine (local) not systemic action
- Superoxide (O₂⁻) → peroxynitrite (ONOO⁻) → toxic, causes tyrosine nitration → oxidative tissue damage
- Thiols → S-nitrosylation (some beneficial, some harmful)
- cGMP degraded by PDE-5 → terminates signaling
Summary / Exam Key Points
- NO = EDRF (endothelium-derived relaxing factor)
- Synthesized from L-Arginine by NOS; cofactors = NADPH, O₂, calmodulin
- Key isoform in CVS = eNOS (activated by shear stress)
- Mechanism: NO → sGC → cGMP → PKG → ↓ Ca²⁺ → vasodilation
- Nitroglycerin works via NO release → venodilation → ↓ preload → antianginal
- Nitroprusside = balanced arteriolar + venous dilation → hypertensive emergencies; cyanide risk
- Inhaled NO → used in neonatal respiratory failure + PAH
- PDE-5 inhibitors (sildenafil) + nitrates = fatal hypotension (contraindicated combination)
- In sepsis: iNOS overactivation → massive NO → refractory hypotension
- NOS inhibitors tried in sepsis - failed clinically (blocked beneficial eNOS too)
Sources: Katzung's Basic & Clinical Pharmacology 16e (Ch. 19), Braunwald's Heart Disease 12e - Lippincott Illustrated Reviews Pharmacology
This is a shared conversation. Sign in to Orris to start your own chat.