Explain me 20 common heart disease with ecg with treatment
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
20 common heart diseases ECG findings treatment summary cardiology
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have solid textbook-sourced content. Let me compile the comprehensive answer on all 20 heart diseases with ECG findings and treatments.
20 Common Heart Diseases: ECG Findings and Treatment
Below is a complete reference covering 20 major cardiac conditions, each with its characteristic ECG pattern and evidence-based treatment. Sources: Braunwald's Heart Disease (12th ed.), Guyton & Hall Medical Physiology, Goldman-Cecil Medicine, Harrison's Principles (22nd ed., 2025), and The Washington Manual of Medical Therapeutics.
1. ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery causing transmural ischemia and necrosis.
ECG Findings:
- ST-segment elevation ≥1 mm in ≥2 contiguous limb leads or ≥2 mm in precordial leads
- Hyperacute (tall, peaked) T waves in early phase
- Pathological Q waves (>40 ms wide, >25% of R wave) develop within hours to days
- Reciprocal ST depression in opposing leads
- Location: anterior (V1-V4 = LAD), inferior (II, III, aVF = RCA), lateral (I, aVL, V5-V6 = LCx)
Treatment:
- Primary PCI within 90 min of first medical contact (first-line)
- Fibrinolysis (alteplase, tenecteplase) if PCI not available within 120 min
- Antiplatelet: aspirin 325 mg loading + P2Y12 inhibitor (ticagrelor or clopidogrel)
- Anticoagulation: UFH or bivalirudin during PCI
- Beta-blockers, ACE inhibitors, high-intensity statins post-MI
- Morphine, oxygen (if SpO2 <90%), nitroglycerin for symptom relief
2. Non-ST-Elevation MI (NSTEMI) / Unstable Angina
Pathophysiology: Partial coronary occlusion or plaque rupture without transmural infarction.
ECG Findings:
- ST depression (≥0.5 mm, horizontal or downsloping) in ischemic leads
- T-wave inversion - often deep, symmetric ("Wellens' pattern" warns of proximal LAD disease)
- No pathological Q waves (differentiates from STEMI)
- ECG may be normal in ~30% of cases
Treatment:
- TIMI/GRACE risk scoring to guide urgency of catheterization
- Dual antiplatelet therapy (aspirin + ticagrelor or clopidogrel)
- Anticoagulation: enoxaparin or UFH
- Early invasive strategy (PCI within 24-48 h) for high-risk patients
- Beta-blockers, nitrates, ACE inhibitors, statins
- GPIIb/IIIa inhibitors (eptifibatide, tirofiban) in selected high-risk PCI patients
3. Atrial Fibrillation (AF)
Pathophysiology: Chaotic, rapid atrial depolarizations (350-600/min) from multiple re-entry circuits; irregular ventricular response.
ECG Findings:
- Absent P waves replaced by irregular fibrillatory (f) waves, best seen in V1 and II
- Irregularly irregular RR intervals (hallmark)
- Ventricular rate 100-180/min if uncontrolled
- No distinct isoelectric baseline
- Narrow QRS (unless aberrant conduction or pre-existing BBB)
Treatment:
- Rate control: Beta-blockers (metoprolol), diltiazem, or digoxin (heart failure)
- Rhythm control: Flecainide, propafenone (no structural disease); amiodarone, dofetilide, sotalol (structural disease); electrical cardioversion
- Anticoagulation (stroke prevention): DOACs (apixaban, rivaroxaban, dabigatran, edoxaban) preferred over warfarin; guided by CHA₂DS₂-VASc score (score ≥2 in men, ≥3 in women = anticoagulate)
- Catheter ablation: Pulmonary vein isolation for symptomatic paroxysmal AF refractory to drugs
- Left atrial appendage closure (Watchman device) for those intolerant to anticoagulation
- Braunwald's: AF occurs in ~12% of patients ≥75 years; all patients ≥75 have CHA₂DS₂-VASc ≥2 and warrant anticoagulation
4. Atrial Flutter
Pathophysiology: Macro-reentrant circuit in the right atrium (cavotricuspid isthmus), rate ~300/min.
ECG Findings:
- Classic "sawtooth" flutter (F) waves at 300/min, best seen in inferior leads (II, III, aVF) and V1
- Regular atrial rate ~300/min with 2:1 or 4:1 AV block (ventricular rate 150 or 75/min)
- 2:1 block producing rate of ~150 bpm should always raise suspicion for flutter
- No isoelectric baseline between flutter waves
Treatment:
- Rate control: Beta-blockers, diltiazem, or digoxin
- Rhythm control: Ibutilide (IV, acute conversion), electrical cardioversion (highly effective)
- Catheter ablation: Cavotricuspid isthmus ablation - curative in >95% of typical flutter
- Anticoagulation: Same as AF (CHA₂DS₂-VASc guided); cardioversion after 48 h requires anticoagulation or TEE to exclude LAA thrombus
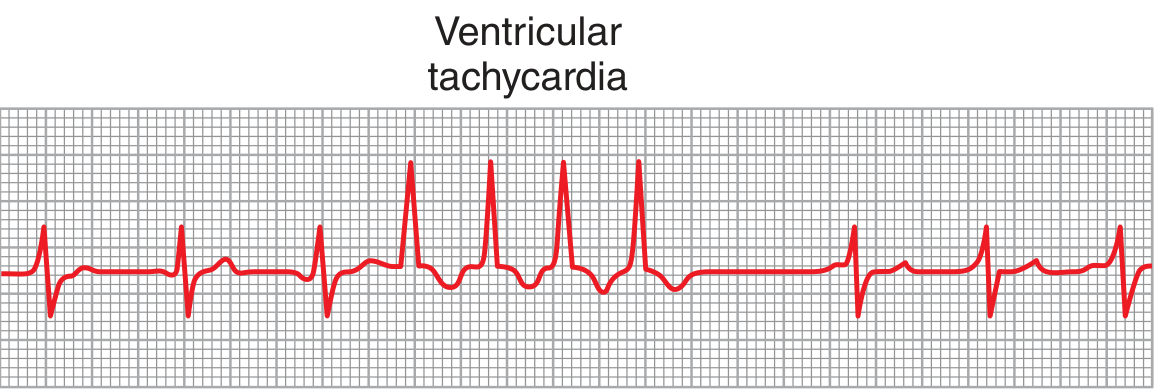
5. Ventricular Tachycardia (VT)
Pathophysiology: ≥3 consecutive ventricular beats at rate >100/min; usually from re-entry around scar tissue.
ECG Findings:
- Wide QRS complexes (>120 ms), bizarre morphology
- Rate 100-250/min, regular or slightly irregular
- AV dissociation (P waves marching independently of QRS) - pathognomonic when visible
- Capture beats (narrow QRS) and fusion beats
- Concordance of QRS in all precordial leads (all positive or all negative)
- LBBB or RBBB morphology depending on exit site
Treatment:
- Unstable VT: Immediate synchronized cardioversion (200 J biphasic)
- Stable VT: IV amiodarone (150 mg bolus, then 1 mg/min) or IV lidocaine
- Chronic/recurrent VT: ICD (implantable cardioverter-defibrillator) - primary prevention for EF ≤35%
- Catheter ablation for recurrent monomorphic VT or VT storm
- Treat underlying cause (ischemia, electrolyte disturbances, digitalis toxicity)
- Guyton: Amiodarone prolongs action potential and refractory period; lidocaine depresses sodium permeability
6. Ventricular Fibrillation (VF)
Pathophysiology: Completely chaotic ventricular activation with no effective cardiac output; invariably fatal without immediate treatment.
ECG Findings:
- Rapid, completely irregular, chaotic deflections of varying amplitude and morphology
- No identifiable QRS complexes, P waves, or T waves
- Rate unidentifiable (400-600 random activations/min)
- Coarse VF (larger amplitude) vs. fine VF (smaller amplitude, worse prognosis)
Treatment:
- Immediate unsynchronized defibrillation (200 J biphasic) - do not delay CPR
- High-quality CPR (30:2) until defibrillation available
- Epinephrine 1 mg IV every 3-5 min
- IV amiodarone (300 mg bolus) after 3rd shock
- Correct reversible causes (4 Hs and 4 Ts)
- ICD implantation in survivors (secondary prevention)
- Guyton: Death begins within 4-5 seconds of VF onset; irreversible tissue injury within minutes
7. Complete Heart Block (Third-Degree AV Block)
Pathophysiology: Complete dissociation between atrial and ventricular conduction; no impulse passes through the AV node.
ECG Findings:
- P waves and QRS complexes march independently (AV dissociation)
- Atrial rate normal (60-100/min); ventricular escape rate 20-40/min (junctional escape 40-60/min)
- QRS wide (>120 ms) if ventricular escape; narrow if junctional escape
- PP intervals regular; RR intervals regular but at different (slower) rate
- PP rate faster than RR rate
Treatment:
- Emergency: Atropine (may be ineffective in infranodal block); transcutaneous pacing
- Definitive: Permanent pacemaker implantation (Class I indication)
- Dual-chamber pacemaker (DDD) preferred to maintain AV synchrony
- Treat reversible causes (Lyme disease, drug toxicity, hyperkalemia, inferior MI)
8. Second-Degree AV Block, Type I (Wenckebach)
Pathophysiology: Progressive conduction delay in the AV node until a beat is dropped.
ECG Findings:
- Progressively lengthening PR interval with each beat
- RR interval progressively shortens
- A non-conducted P wave (dropped QRS) occurs cyclically
- Group beating pattern on the rhythm strip
- Usually narrow QRS (block is at AV node level)
Treatment:
- Often benign, especially in athletes or during inferior MI (vagal)
- Treat underlying cause (drug toxicity - digoxin, beta-blocker; inferior MI)
- Atropine if symptomatic
- Pacemaker rarely needed unless symptomatic or associated with wide complex
9. Second-Degree AV Block, Type II (Mobitz II)
Pathophysiology: Intermittent failure of conduction below the AV node (His bundle or bundle branches); more dangerous than Type I.
ECG Findings:
- Fixed PR interval (normal or prolonged) with sudden unexpected dropped QRS
- No progressive PR lengthening before the dropped beat
- Wide QRS complexes (infranodal block)
- May progress abruptly to complete heart block
Treatment:
- Permanent pacemaker (Class I indication regardless of symptoms)
- Higher risk than Wenckebach; may precipitate syncope or sudden death
- Transcutaneous/transvenous pacing as bridge
10. Left Bundle Branch Block (LBBB)
Pathophysiology: Block in the left bundle branch causing delayed left ventricular activation.
ECG Findings:
- QRS duration ≥120 ms
- Broad, notched ("M-shaped") R waves in lateral leads (I, aVL, V5-V6)
- rS pattern in V1 (deep S wave)
- No septal Q waves in lateral leads
- ST depression and T-wave inversion in lateral leads (secondary repolarization changes)
- New LBBB + chest pain = STEMI equivalent (Sgarbossa criteria)
Treatment:
- Treat underlying cause (CAD, hypertension, cardiomyopathy)
- LBBB with EF ≤35% and NYHA Class II-III HF: Cardiac Resynchronization Therapy (CRT/biventricular pacing) - significant mortality and symptom benefit
- New LBBB in context of ACS: treat as STEMI
11. Right Bundle Branch Block (RBBB)
Pathophysiology: Block in the right bundle branch; left ventricle activates first, then right ventricle.
ECG Findings:
- QRS ≥120 ms
- RSR' ("bunny ear") pattern in V1-V2
- Wide, slurred S wave in lateral leads (I, aVL, V5-V6)
- T-wave inversion in V1-V3 (secondary changes)
- Incomplete RBBB: QRS 100-119 ms with same pattern
Treatment:
- Isolated RBBB in asymptomatic patients: no treatment needed (often benign)
- New RBBB in pulmonary embolism context: suggests RV strain (treat PE)
- New RBBB with anterior MI: high risk, may need temporary pacing
- Bifascicular block (RBBB + left fascicular block) with syncope: permanent pacemaker
12. Supraventricular Tachycardia (SVT) / AVNRT
Pathophysiology: Re-entry circuit within or near the AV node (AVNRT most common, ~60% of SVTs); sudden onset and termination.
ECG Findings:
- Narrow QRS tachycardia, rate 150-250/min, regular
- P waves often hidden within or immediately after QRS (pseudo-R' in V1, pseudo-S in inferior leads)
- Retrograde P waves (inverted in II, III, aVF) if visible
- Abrupt onset and termination
- "Long RP" (AVRT) vs. "Short RP" (AVNRT) distinction
Treatment:
- Acute: Vagal maneuvers (Valsalva, carotid sinus massage) first
- IV adenosine 6 mg (then 12 mg) - drug of choice for acute termination
- IV diltiazem or beta-blocker if adenosine fails
- Synchronized cardioversion if hemodynamically unstable
- Long-term: Catheter ablation (curative >95%); drug prophylaxis (verapamil, beta-blockers) if ablation declined
13. Wolff-Parkinson-White (WPW) Syndrome
Pathophysiology: Accessory pathway (Bundle of Kent) bypasses the AV node causing pre-excitation; risk of rapid conduction in AF.
ECG Findings:
- Short PR interval (<120 ms)
- Delta wave (slurred upstroke of QRS)
- Wide QRS (>120 ms) due to pre-excitation
- Secondary ST-T changes
- AF with WPW: irregular, very rapid (>250/min), wide complex ("antidromic" - life-threatening)
Treatment:
- Symptomatic or AF with WPW: Catheter ablation of accessory pathway (curative, first-line)
- Avoid AV nodal blocking agents (digoxin, diltiazem, beta-blockers, adenosine) in AF+WPW - may accelerate conduction via accessory pathway causing VF
- Acute AF+WPW with hemodynamic instability: immediate DC cardioversion
- Acute AF+WPW stable: IV procainamide or IV ibutilide
14. Heart Failure with Reduced Ejection Fraction (HFrEF)
Pathophysiology: Reduced LV systolic function (EF <40%) causing inadequate cardiac output; neurohormonal activation accelerates progression.
ECG Findings:
- Often non-specific; may show:
- LVH (Sokolow-Lyon criteria: S in V1 + R in V5-V6 >35 mm)
- LBBB (as above)
- Signs of underlying ischemia (Q waves, ST changes)
- Low voltage in pericardial effusion
- Atrial fibrillation (common comorbidity)
- Sinus tachycardia (compensatory)
Treatment (4 pillars of HFrEF):
- ACE inhibitor or ARB/sacubitril (ARNi - sacubitril/valsartan) - RAAS blockade
- Beta-blocker (carvedilol, metoprolol succinate, bisoprolol)
- Mineralocorticoid receptor antagonist (spironolactone, eplerenone)
- SGLT2 inhibitor (dapagliflozin, empagliflozin) - added as 4th pillar per 2022 guidelines
- Loop diuretics (furosemide) for fluid overload
- CRT if LBBB + EF ≤35%
- ICD for EF ≤35% and NYHA Class II-III
- LVAD or heart transplant for refractory Stage D HF
15. Hypertrophic Cardiomyopathy (HCM)
Pathophysiology: Autosomal dominant mutation in sarcomere proteins (usually beta-myosin heavy chain) causing asymmetric LV hypertrophy, diastolic dysfunction, and dynamic LVOT obstruction.
ECG Findings:
- LVH criteria (high voltage: deep S in V1 + tall R in V5-V6)
- Deep, narrow "dagger-like" Q waves in lateral and inferior leads (septal depolarization)
- T-wave inversion in lateral leads (especially in apical variant)
- ST depression, left axis deviation
- AF (late complication)
- Giant T-wave inversions (Yamaguchi/apical HCM variant)
Treatment:
- Symptomatic obstruction: Beta-blockers (first-line); verapamil, disopyramide
- Mavacamten (cardiac myosin inhibitor) - FDA-approved 2022 for symptomatic obstructive HCM
- Alcohol septal ablation or surgical myectomy for drug-refractory LVOT obstruction
- ICD for high-risk patients (prior VF, VT, unexplained syncope, family history of SCD, massive LVH ≥30 mm)
- Anticoagulation if AF develops
- Avoid strenuous competitive athletics
16. Dilated Cardiomyopathy (DCM)
Pathophysiology: LV or biventricular dilation with reduced systolic function; causes include viral myocarditis, alcohol, genetic, idiopathic.
ECG Findings:
- Sinus tachycardia
- LVH or low voltage
- LBBB (common)
- Left axis deviation
- Non-specific ST-T changes
- Atrial fibrillation (common)
- Frequent PVCs or NSVT
Treatment:
- Same 4-pillar HFrEF treatment (ACEi/ARNi, beta-blocker, MRA, SGLT2i)
- ICD for EF ≤35% (primary prevention of SCD)
- CRT for LBBB + EF ≤35%
- Abstain from alcohol (alcoholic DCM may reverse with abstinence)
- Anticoagulation if AF or LV thrombus
- Treat underlying cause (immunosuppression for giant cell myocarditis, etc.)
17. Pericarditis (Acute)
Pathophysiology: Inflammation of the pericardium; causes include viral, idiopathic, post-MI (Dressler's), autoimmune, uremic.
ECG Findings - Classic 4 Stages:
- Stage 1 (early): Diffuse saddle-shaped (concave up) ST elevation in almost all leads except aVR and V1 (where there is ST depression); PR depression (pathognomonic)
- Stage 2: ST returns to baseline; PR depression persists
- Stage 3: T-wave inversions (diffuse)
- Stage 4: ECG normalizes
- Key distinction from STEMI: ST elevation is diffuse (not regional), concave up, PR depression present, no reciprocal ST depression (except aVR/V1)
Treatment:
- Aspirin 750-1000 mg every 8h for 1-2 weeks (first-line for idiopathic/viral)
- Colchicine 0.5 mg twice daily for 3 months - reduces recurrence by ~50%
- NSAIDs (ibuprofen) as alternative to aspirin
- Restrict physical activity until resolution
- Corticosteroids only if aspirin/NSAID contraindicated (higher recurrence rate)
- Treat pericardial effusion/tamponade with pericardiocentesis if hemodynamically significant
18. Pulmonary Embolism (PE)
Pathophysiology: Thromboembolism obstructing pulmonary vasculature causing acute RV pressure overload and strain.
ECG Findings:
- Sinus tachycardia (most common finding, ~44%)
- S1Q3T3 pattern: S wave in lead I, Q wave and T-wave inversion in lead III (classic but only in ~20%)
- Right axis deviation
- New incomplete or complete RBBB (RV strain)
- T-wave inversions in right precordial leads (V1-V4)
- P pulmonale (peaked P waves in II)
- AF or atrial flutter
- ECG may be normal in small PE
Treatment:
- Anticoagulation: DOACs (rivaroxaban, apixaban preferred) or UFH/LMWH bridge to warfarin
- Massive PE (hemodynamic instability): Systemic thrombolysis (alteplase 100 mg over 2h) or catheter-directed therapy
- Submassive PE (RV dysfunction): Anticoagulation + consider thrombolysis in deteriorating patients
- Oxygen, hemodynamic support
- IVC filter only if anticoagulation absolutely contraindicated
- Extended anticoagulation for unprovoked PE (3-6 months minimum, often indefinite)
19. Sick Sinus Syndrome (SSS)
Pathophysiology: Dysfunction of the SA node causing bradyarrhythmias, often alternating with tachyarrhythmias (tachycardia-bradycardia syndrome).
ECG Findings:
- Sinus bradycardia (<50/min)
- Sinus pauses/arrest (prolonged PP intervals, no P wave)
- Sinoatrial exit block (PP interval doubles)
- Alternating with episodes of AF, atrial flutter, or SVT (tachycardia-bradycardia pattern)
- Chronotropic incompetence (failure to increase HR with exertion)
Treatment:
- Symptomatic SSS: Permanent pacemaker (Class I; AAI or DDD pacing)
- Pacemaker implantation allows safe use of antiarrhythmic drugs for the tachycardia component
- Anticoagulation if AF episodes occur (CHA₂DS₂-VASc guided)
- Avoid drugs that worsen bradycardia (beta-blockers, calcium channel blockers) without pacemaker protection
20. Long QT Syndrome (LQTS)
Pathophysiology: Genetic (congenital) or acquired prolongation of ventricular repolarization; predisposes to torsades de pointes (TdP) - polymorphic VT - and sudden cardiac death.
ECG Findings:
- Prolonged QTc interval: >450 ms in men, >460 ms in women (corrected using Bazett formula: QTc = QT/√RR)
- QTc >500 ms: high risk for TdP
- Abnormal T-wave morphology: notched, bifid, or broad T waves depending on LQTS subtype
- U waves (prominent in hypokalemia-associated QT prolongation)
- Torsades de pointes: polymorphic VT with QRS complexes rotating around the isoelectric axis ("twisting of points")
Treatment:
- Beta-blockers (nadolol, propranolol) - mainstay for congenital LQTS (LQT1 and LQT2)
- ICD for prior cardiac arrest, recurrent syncope on beta-blockers, or QTc >550 ms with symptoms
- Avoid QT-prolonging drugs (check CredibleMeds/azlist.org)
- Correct electrolytes (hypokalemia, hypomagnesemia worsen QT)
- Acute TdP: IV magnesium sulfate 2g bolus; correct K+ to 4.5-5 mEq/L; overdrive pacing (isoproterenol or temporary pacing at 100/min)
- Left cardiac sympathetic denervation (LCSD) as adjunct therapy
Quick Reference Summary Table
| # | Condition | Key ECG Finding | 1st-Line Treatment |
|---|---|---|---|
| 1 | STEMI | ST elevation + Q waves | Primary PCI within 90 min |
| 2 | NSTEMI/UA | ST depression, T inversion | Antiplatelet + anticoagulation, early PCI |
| 3 | Atrial Fibrillation | Absent P waves, irregularly irregular | Rate/rhythm control + anticoagulation (DOAC) |
| 4 | Atrial Flutter | Sawtooth F waves at 300/min | Catheter ablation (cavotricuspid isthmus) |
| 5 | Ventricular Tachycardia | Wide QRS, AV dissociation | Cardioversion if unstable; amiodarone/ICD |
| 6 | Ventricular Fibrillation | Chaotic, no QRS | Immediate defibrillation + CPR |
| 7 | Complete Heart Block | AV dissociation, slow escape | Permanent pacemaker |
| 8 | Wenckebach | Progressive PR lengthening, dropped beat | Observation/treat cause |
| 9 | Mobitz II | Fixed PR, sudden dropped QRS | Permanent pacemaker |
| 10 | LBBB | Wide QRS, M-shaped R in lateral | Treat cause; CRT if HF |
| 11 | RBBB | RSR' in V1, wide S in lateral | Usually no treatment; treat cause |
| 12 | SVT/AVNRT | Narrow QRS tachycardia, P in QRS | Adenosine; catheter ablation |
| 13 | WPW | Short PR, delta wave | Catheter ablation; avoid AV nodal blockers in AF |
| 14 | HFrEF | LVH, LBBB, non-specific changes | ACEi/ARNi + beta-blocker + MRA + SGLT2i |
| 15 | HCM | Deep Q waves lateral, LVH | Beta-blockers; mavacamten; ICD if high-risk |
| 16 | DCM | LBBB, low voltage, AF | HFrEF regimen; ICD/CRT |
| 17 | Acute Pericarditis | Diffuse saddle ST elevation, PR depression | Aspirin + colchicine 3 months |
| 18 | Pulmonary Embolism | Tachycardia, S1Q3T3, RBBB | Anticoagulation; thrombolysis if massive |
| 19 | Sick Sinus Syndrome | Sinus pauses, bradycardia-tachycardia | Permanent pacemaker |
| 20 | Long QT Syndrome | QTc >450-460 ms, torsades | Beta-blockers; ICD; avoid QT-prolonging drugs |
Sources:
- Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 12th Edition
- Guyton & Hall Textbook of Medical Physiology, 14th Edition
- Goldman-Cecil Medicine, International Edition
- Harrison's Principles of Internal Medicine, 22nd Edition (2025)
- The Washington Manual of Medical Therapeutics
Clinical Note: ECG interpretation must always be integrated with clinical context, patient history, and other investigations. Drug dosages and guideline recommendations should be verified against current institutional protocols. This content is for educational purposes.
This is a shared conversation. Sign in to Orris to start your own chat.