Fundamental principles of ventricular assist devices
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ventricular assist device" AND "mechanical circulatory support"
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Excellent! I now have all the content I need. Let me compile a comprehensive, well-structured answer.
Fundamental Principles of Ventricular Assist Devices (VADs)
1. Definition and Concept
Mechanical circulatory support (MCS) devices are mechanical pumps designed to assist or replace the function of the left and/or right ventricle(s). A ventricular assist device specifically augments cardiac output by drawing blood from a failing ventricle and returning it to the systemic or pulmonary circulation. Important characterizing features include: (1) location of the pumping chamber; (2) ventricle(s) supported; (3) pumping mechanism; and (4) intended duration of support.
- Braunwald's Heart Disease, p. 328
2. Indications and Treatment Strategies
VADs are indicated when hemodynamic compromise is refractory to guideline-directed medical therapy. Three therapeutic strategies define clinical use:
| Strategy | Abbreviation | Description |
|---|---|---|
| Bridge to Recovery | BTR | Temporary support until native myocardial function recovers (e.g., acute MI, myocarditis, Takotsubo) |
| Bridge to Transplantation | BTT | Longer support allowing time for donor heart allocation |
| Destination Therapy | DT | Permanent support in transplant-ineligible patients |
Hemodynamic thresholds that generally trigger MCS initiation:
- Cardiac index < 1.8-2.2 L/min/m²
- Systolic BP < 90 mm Hg
- PCWP > 20 mm Hg
- Evidence of end-organ hypoperfusion: oliguria, rising creatinine, elevated lactate, altered mentation, cool extremities
Patients can and often do transition between strategies as their clinical circumstances evolve. Candid discussion of the intended strategy is both legally and morally essential.
- Braunwald's Heart Disease, pp. 328-330
3. Basic Components
All left-sided VAD systems share a common anatomical circuit:
LV apex (inflow cannula) → Pump → Ascending aorta (outflow cannula)
For right ventricular support, cannulas drain from the right atrium or RV and return blood to the pulmonary artery. Temporary devices have long external cannulas that traverse the skin to connect to an extracorporeal pump. Durable devices are fully implantable.
- Braunwald's Heart Disease, p. 330
4. Pump Types and Mechanisms
4a. Pulsatile-Flow, Volume-Displacement Pumps (Historical)
- Mimicked the phasic contractions of the native heart
- Provided flexibility for biventricular support
- No longer commercially available for adults; restricted to pediatric temporary use
- Disadvantages: large size, many moving parts, higher energy requirement, limited durability
4b. Continuous-Flow Rotary Pumps (Current Standard)
These have almost entirely replaced pulsatile pumps for both short- and long-term support, offering:
- Smaller size
- Fewer moving parts - greater durability and reliability
- Limited blood-contacting surfaces
- Reduced energy requirements
How they work: A spinning internal impeller is suspended within a tube and propels blood forward by imparting kinetic energy. The impeller is actuated by an electrical current and magnetic field interacting with internal magnets in the impeller.
Although called "continuous flow," these pumps are not truly non-pulsatile when the native heart is contracting. Flow is greater during systole (lower pressure gradient across the pump) than diastole. This phasic variation imparts a reduced but real pulse pressure to the circulation. Only in ventricular fibrillation or arrest is flow truly non-pulsatile.
- Braunwald's Heart Disease, p. 330
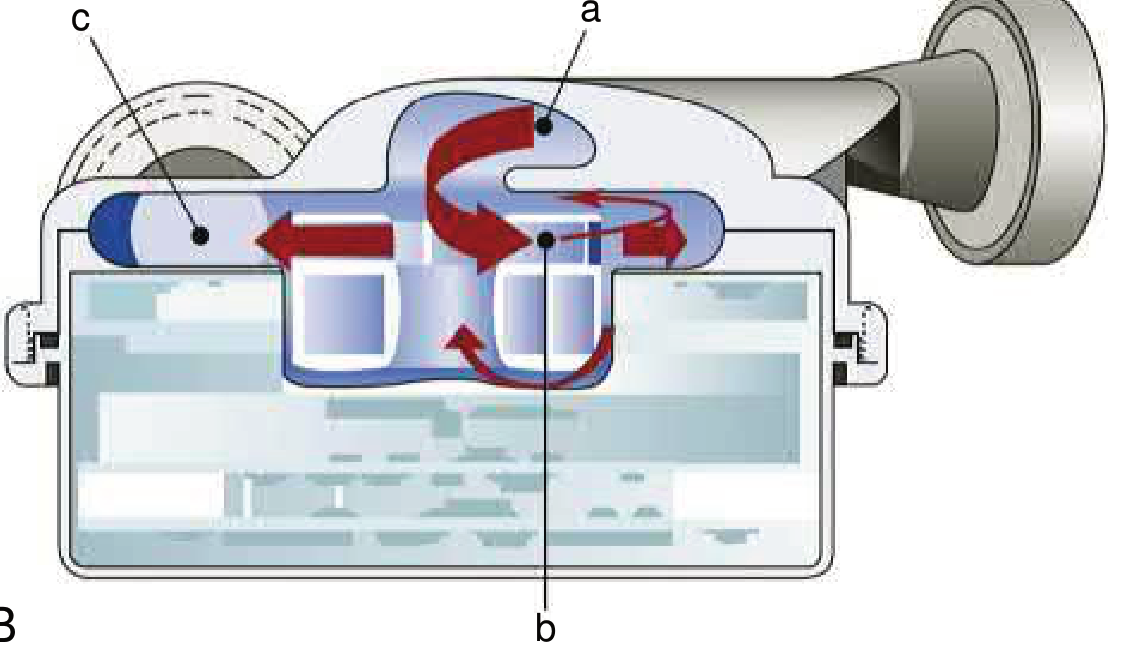
EFIGURE 59.1 - Axial (A) and centrifugal (B) rotary pump designs. From Braunwald's Heart Disease.
5. Axial vs. Centrifugal Flow Design
| Feature | Axial Flow | Centrifugal Flow |
|---|---|---|
| Blood path | Along the axis of rotation | Radially outward from center |
| Impeller support | Mechanical bearings or pivot | Magnetic or hydrodynamic levitation |
| Speed (RPM) | Higher (~8,000-12,000) | Lower (~2,000-3,500) |
| Examples | HeartMate II (HMII) | HeartMate 3 (HM3), TandemHeart |
| Shear stress | Higher | Lower |
Impeller suspension methods:
-
Mechanical bearings: Pivot contact design - potential frictional wear and heat generation over time, may lead to device failure
-
Hydrodynamic levitation: Fluid forces alone suspend the impeller; simpler electronics, smaller pump, but impeller may contact housing at very low speeds
-
Magnetic levitation (passive or active): Permanent magnets (passive, no power) or electromagnets (active, position sensing); fully contactless design eliminates bearing wear
-
Hybrid systems: Combination of hydrodynamic + magnetic levitation (e.g., HM3 uses passive magnetic + hydrodynamic)
-
Braunwald's Heart Disease, pp. 330-331
6. Hydrodynamic Properties
The fundamental operating principle of a continuous-flow rotary pump:
Flow = f(pump speed, pressure gradient)
- Flow is directly proportional to pump speed (RPM)
- Flow is inversely proportional to the pressure gradient across the pump (aortic pressure minus LV pressure)
This means:
- If aortic afterload rises, flow decreases at a fixed RPM
- If the native heart contracts weakly (high LV pressure), less gradient exists and pump can generate more flow
- Clinicians can titrate RPM to balance ventricular unloading and cardiac output
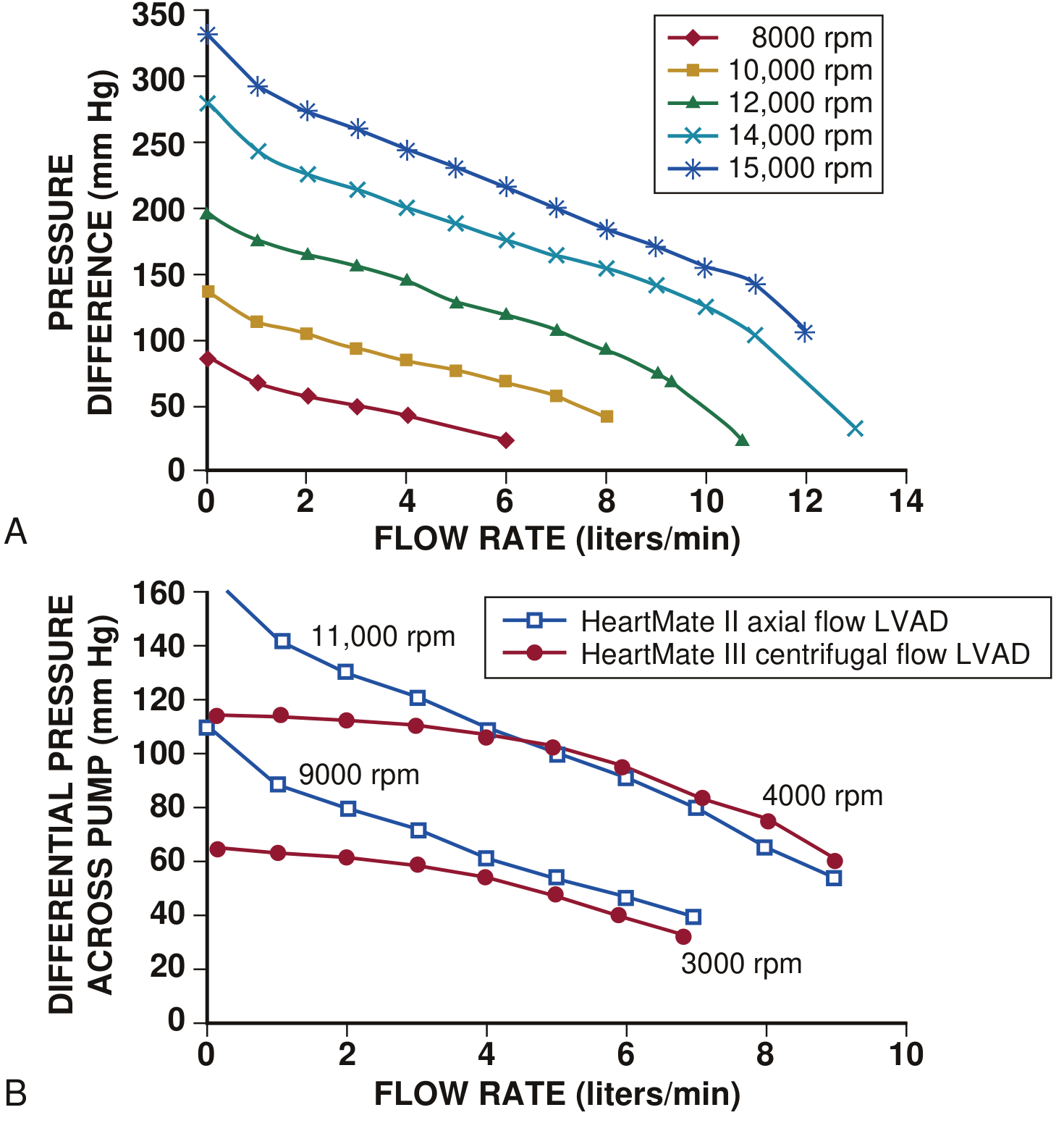
EFigure 59.3 - Hydrodynamic properties: flow is inversely related to pressure gradient and directly related to pump speed (RPM). From Braunwald's Heart Disease.
7. Specific Devices
Temporary/Short-term Devices
| Device | Type | Mechanism | Support |
|---|---|---|---|
| IABP (Intra-Aortic Balloon Pump) | Counterpulsation | Inflates in diastole, deflates in systole | LV (passive, ~0.5 L/min augmentation) |
| Impella | Microaxial rotary | Transvalvular catheter; aspirates from LV, ejects into aorta | LV (up to 5.5 L/min) |
| TandemHeart | Centrifugal | Transseptal LA drainage, returns to femoral artery | LV bypass (~4 L/min) |
| VA-ECMO | Centrifugal + membrane oxygenator | Drains venous blood, oxygenates, returns to artery | Biventricular + pulmonary |
The IABP-SHOCK II trial demonstrated that IABP does not reduce 30-day, 12-month, or 6-year mortality in cardiogenic shock with LV failure, and it is no longer recommended for this indication. Active percutaneous devices (Impella, TandemHeart) provide better hemodynamic support but have not yet demonstrated a clear mortality benefit in randomized trials. - Harrison's Principles of Internal Medicine 22E
Durable/Long-term Devices
- HeartMate II (HMII): First-generation axial-flow LVAD; most studied with >20,000 implantations worldwide
- HeartMate 3 (HM3): Centrifugal, fully magnetically levitated impeller; superior survival and lower stroke/GI bleeding vs. HMII in the MOMENTUM 3 trial
- HeartWare HVAD: Now discontinued (June 2021) after showing a 3.49x higher hazard ratio for mortality vs. HM3
8. Patient Selection Considerations
Before implantation, the following must be carefully assessed:
Renal function: Most common risk for morbidity/mortality. Cardiogenic shock elevates CVP, worsening renal congestion independent of low-flow injury.
Coagulation: Abnormal INR (without warfarin) reflects hepatic congestion/fibrosis. Combined coagulopathy + anticoagulation increases perioperative bleeding, RV failure, and multi-organ failure. Heparin-induced thrombocytopenia (HIT) must be screened.
Valvular disease:
- Mild-moderate AS: Not a contraindication
- Severe AS: Must be corrected (bioprosthesis) before LVAD to allow future weaning
- Moderate AI: Causes LV distension with LA-aorta cannulation; with LV apex-aorta devices, AI worsens as LV pressure drops (creates circular flow loop)
Right ventricular function: RV failure is a major post-implant complication; preoperative RV assessment is essential. A temporary right ventricular assist device (RVAD) may be needed post-LVAD.
Pulmonary hypertension, hepatic function, intracardiac shunts, and arrhythmias all require evaluation.
- Braunwald's Heart Disease, pp. 329-334
9. Adverse Events and Complications
The major complications common to all VADs:
| Complication | Mechanism |
|---|---|
| Driveline infection | Percutaneous driveline provides a conduit for bacteria; most common infection site |
| Gastrointestinal bleeding | Loss of high-molecular-weight von Willebrand factor multimers (shear-induced degradation), acquired vWD; arteriovenous malformations (AVMs) related to reduced pulse pressure |
| Stroke (ischemic/hemorrhagic) | Pump thrombosis causing emboli; inadequate anticoagulation; hypertension; hemorrhage from over-anticoagulation |
| Pump thrombosis | Thrombus in the pump itself - presents with power spikes, hemolysis, and worsening hemodynamics |
| Right heart failure | Increased preload to RV after LVAD decompresses LV; interventricular septal shift |
| Aortic insufficiency (acquired) | Reduced LV pressure from LVAD creates pressure gradient promoting AI development |
| Device failure | Bearing wear, lead fracture, driveline damage |
Anticoagulation (warfarin, target INR 2-3) plus antiplatelet therapy (aspirin) is standard for durable LVADs. The HM3's fully magnetically levitated design essentially eliminated pump thrombosis in MOMENTUM 3.
- Braunwald's Heart Disease; Miller's Anesthesia 10e; Mulholland and Greenfield's Surgery 7e
10. Monitoring and Management
- INTERMACS (Interagency Registry for Mechanically Assisted Circulatory Support): The primary registry tracking outcomes of all durable MCS devices in the United States. Provides risk stratification profiles (INTERMACS profiles 1-7, with 1 = critical cardiogenic shock, 7 = advanced NYHA III).
- Pump speed is titrated to optimize cardiac output while preventing ventricular suction (over-decompression of the LV)
- Echocardiography guides cannula position, RV function assessment, aortic valve opening frequency, and detection of complications
- Mean arterial pressure (not standard cuff systolic/diastolic) is the relevant blood pressure measurement in continuous-flow VAD patients
Summary
VADs work by mechanically unloading a failing ventricle and generating forward flow. The field has shifted from bulky pulsatile pumps to compact continuous-flow rotary pumps, with the centrifugal magnetically levitated design (HM3) now representing the gold standard for durable support. The three strategic goals - bridge to recovery, bridge to transplant, and destination therapy - frame all clinical decision-making. Complication management, particularly GI bleeding, stroke, driveline infection, and right heart failure, remains the central challenge of long-term VAD support.
Recent literature to note:
- Durable Mechanical Circulatory Support: JACC Scientific Statement (2023) - PMID 37758441: Comprehensive 2023 JACC statement covering current evidence and management
- Right Heart Failure with LVAD - ESC HFA Consensus Statement (2024) - PMID 38853659: Pre/peri/post-operative strategies for RV failure management
This is a shared conversation. Sign in to Orris to start your own chat.