Principal of administrative safe general anaesthesia ?
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from the textbooks. Let me compile the complete answer on the principles of safe general anaesthesia.
Principles of Safe General Anaesthesia
General anaesthesia (GA) is a reversible state of unconsciousness achieved through a combination of drugs that produce: amnesia, analgesia, inhibition of noxious reflexes, and skeletal muscle relaxation — the four classic components of the anaesthetic state.
— Sabiston Textbook of Surgery, p. 345
1. The Four Components of General Anaesthesia
| Component | Goal | Agents Used |
|---|---|---|
| Amnesia (unconsciousness) | No recall of events | IV agents (propofol, thiopental, etomidate), volatile agents |
| Analgesia | Pain-free state | Opioids (fentanyl, morphine, remifentanil), ketamine |
| Suppression of noxious reflexes | Blunt autonomic/somatic stress responses | Opioids, volatile agents, β-blockers |
| Muscle relaxation | Facilitate intubation & surgical access | Depolarizing (succinylcholine) or non-depolarizing (rocuronium, vecuronium) NMBAs |
Because the drugs producing these effects also cause respiratory depression, cardiovascular depression, and loss of airway protection, the pharmacologic effects must be carefully matched to each patient's pathophysiology.
— Sabiston, p. 345
2. Preoperative Assessment & Preparation
Safe anaesthesia begins before the patient enters the operating room:
- History & physical: Identify comorbidities (cardiovascular, respiratory, renal, hepatic disease), prior anaesthetic problems, allergies, current medications
- Airway assessment: Predict difficult airway (Mallampati scoring, thyromental distance, mouth opening, neck mobility) — anticipation is the cornerstone of airway safety
- Fasting (NPO) status: Reduce aspiration risk — typically 6 h for solids, 2 h for clear fluids
- Premedication: Anxiolytics, antacids, antiemetics, continuation or cessation of medications as appropriate
- Informed consent: Including explicit discussion of risks — awareness, aspiration, cardiovascular events, postoperative nausea/vomiting
3. Standard Monitoring (ASA Standards)
The ASA minimum standards must be applied before induction:
| Monitor | Purpose |
|---|---|
| Pulse oximetry (SpO₂) | Detect hypoxaemia in real time |
| ECG | Detect arrhythmias and ischaemia (V5 lead for ischaemia) |
| Non-invasive blood pressure (NIBP) | Haemodynamic surveillance |
| Capnography (EtCO₂) | Confirm tracheal intubation; monitor ventilation |
| Temperature | Prevent hypothermia (especially in paediatrics) |
| Volatile agent concentration | Assess anaesthetic depth |
Additional monitoring (arterial line, CVP, TOE, BIS, NIRS) is added based on patient and surgical risk.
4. Airway Management
Airway loss is the single most dangerous event in anaesthesia. The ASA Difficult Airway Algorithm mandates:
- Assess likelihood of difficult ventilation, difficult intubation, difficulty with patient cooperation, and difficult tracheostomy
- Actively deliver supplemental oxygen throughout airway management
- Plan primary AND backup strategies before induction
- If the airway is anticipated to be difficult → preserve spontaneous ventilation (awake fibreoptic intubation, high-flow nasal oxygen, topical anaesthesia)
- If unexpected difficulty arises after induction → call for help, use video laryngoscope, LMA, bougie, or surgical airway if needed
"Cannot intubate, cannot oxygenate" (CICO) is a life-threatening emergency — front-of-neck access (emergency cricothyroidotomy) must not be delayed.

5. Phases of General Anaesthesia
A. Induction
- Goals: Smooth, rapid loss of consciousness while maintaining cardiovascular stability and protecting the airway
- Agents: Propofol (most common), etomidate (haemodynamically unstable patients), ketamine (trauma, bronchospasm), thiopental (historical)
- Intubation: Facilitated by non-depolarising NMBAs (rocuronium 1.2 mg/kg, vecuronium 0.1 mg/kg) or succinylcholine for rapid sequence intubation (RSI)
- Preoxygenation: 3 minutes tidal breathing or 8 vital capacity breaths of 100% O₂ to denitrogenate (maximise safe apnoea time)
- RSI is mandatory for full-stomach/aspiration-risk patients: rapid induction + cricoid pressure + intubation without bag-mask ventilation
B. Maintenance
- Aims: Adequate depth (prevent awareness and autonomic responses), haemodynamic stability, optimal ventilation
- Inhalational maintenance: Sevoflurane, isoflurane, desflurane ± nitrous oxide
- Total intravenous anaesthesia (TIVA): Propofol infusion ± remifentanil — preferred when inhalational agents are contraindicated (malignant hyperthermia risk, PONV-prone patients, neuromonitoring)
- Ventilation: Lung-protective strategy (tidal volume 6–8 mL/kg IBW, PEEP 5 cmH₂O, FiO₂ titrated to maintain SpO₂ >95%), EtCO₂ maintained in normal range (35–45 mmHg)
- Fluid management: Balanced crystalloids; goal-directed therapy in major surgery; avoid hyperglycaemia
- Temperature: Active warming (forced-air blanket, fluid warmers)
C. Emergence & Extubation
- Criteria for extubation: Awake, following commands, adequate spontaneous ventilation (RR >8, tidal volume >5 mL/kg), SpO₂ >95% on FiO₂ 0.4, reversal of neuromuscular blockade confirmed (train-of-four ratio ≥0.9), normothermic, haemodynamically stable
- Reversal of NMB: Neostigmine + glycopyrrolate (acetylcholinesterase inhibitors), or sugammadex (for rocuronium/vecuronium — preferred for deep block)
- Smooth emergence: Avoid bucking/hypertension — use lidocaine IV, remifentanil, or dexmedetomidine
- Post-extubation: Supplemental O₂, lateral recovery position, monitor for laryngospasm and re-obstruction
6. Prevention of Critical Complications
| Complication | Prevention Principle |
|---|---|
| Hypoxaemia | Preoxygenation, pulse oximetry, lung-protective ventilation, SpO₂ monitoring |
| Aspiration | NPO fasting, RSI for full stomach, avoid premature extubation |
| Awareness under anaesthesia | Adequate volatile agent concentration (≥0.7 MAC), BIS monitoring, avoid NMBAs without confirmed anaesthetic depth, benzodiazepines for high-risk cases (cardiac, obstetric, trauma surgery) |
| Hypotension | Volume loading, vasopressors (phenylephrine, noradrenaline), judicious induction agents |
| Cardiac arrest | Continuous ECG, IV access confirmed before induction, emergency drugs drawn up (adrenaline, atropine) |
| Malignant hyperthermia | Know susceptible patients (personal/family history, myopathies), avoid volatile agents and succinylcholine, dantrolene immediately available |
| Hypothermia | Warm OR, forced-air warming, warm IV fluids |
| Postoperative nausea & vomiting (PONV) | Multimodal prophylaxis (ondansetron, dexamethasone, TIVA) for high-risk patients |
7. Drug Safety Principles
- Never administer NMBAs without confirmed IV access and ability to ventilate — awake paralysis is a medico-legal emergency
- Label all syringes at the time of drawing and before administration
- Verify drug and dose — medication errors are a leading cause of awareness and cardiac arrest
- Maintain anaesthetic continuity — do not allow vaporiser to empty or TIVA infusion to run dry
8. WHO Surgical Safety Checklist
The WHO Surgical Safety Checklist is a cornerstone of safe anaesthesia:
- Sign In (before induction): patient identity, procedure, site marked, anaesthetic machine and medication check, pulse oximetry, allergy/difficult airway/aspiration risk, blood loss risk
- Time Out (before skin incision): team introductions, procedure confirmation, antibiotic prophylaxis, anticipated critical events
- Sign Out (before leaving OR): instrument/sponge counts, specimen labelling, equipment concerns, recovery plan
Summary
Safe general anaesthesia is built on the principle that preparation, vigilance, and systematic safety protocols prevent harm. The four-component model (amnesia, analgesia, reflex suppression, muscle relaxation) guides drug selection; standardized monitoring and airway algorithms prevent the most common life-threatening crises; and structured checklists and team-based communication ensure every step is performed correctly.
"The four components of general anesthesia are usually achieved in modern anesthesia by a combination of IV anesthetics and analgesics, inhalational anesthetics, and, frequently, muscle relaxants. Because the drugs that produce these components cause both desirable and undesirable physiologic changes, the pharmacologic effects of the agents must be matched to the pathophysiology of the patient's comorbidities." — Sabiston Textbook of Surgery, p. 345
Sources:
- Morgan and Mikhail's Clinical Anesthesiology, 7e
- Sabiston Textbook of Surgery, p. 344–346
- Miller's Anesthesia, 10e
Osteomyelitis
Reading File
Finding Sources
Finding Sources
Searching PubMed
osteomyelitis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material from 6 authoritative textbooks. Let me compile the full answer:
Osteomyelitis
Osteomyelitis is inflammation of bone and marrow, virtually always secondary to infection. It may complicate any systemic infection or present as a solitary primary focus.
— Robbins Pathologic Basis of Disease, p. 989
1. Pathogenesis & Routes of Infection
Three mechanisms underlie osteomyelitis:
- Haematogenous spread — bacteria seed bone during bacteraemia; the most common route in children and for vertebral osteomyelitis in adults
- Contiguous spread — from adjacent infected soft tissue, or after surgery/trauma (open fractures, joint replacement, sternal surgery)
- Vascular insufficiency / neuropathy — chronic progressive deep soft tissue infection, most commonly diabetic foot
— Harrison's Principles of Internal Medicine 22e, p. 1105
Why the Metaphysis?
In haematogenous osteomyelitis, the metaphysis of long bones is preferentially infected because slow blood flow through looped sinusoidal vessels combined with microtrauma encourages bacterial seeding during bacteraemia. In neonates, metaphyseal vessels penetrate the growth plate, allowing spread to the epiphysis and adjacent joint. After growth plate closure in adults, anastomoses between metaphyseal and epiphyseal vessels facilitate bacterial spread to subchondral regions.
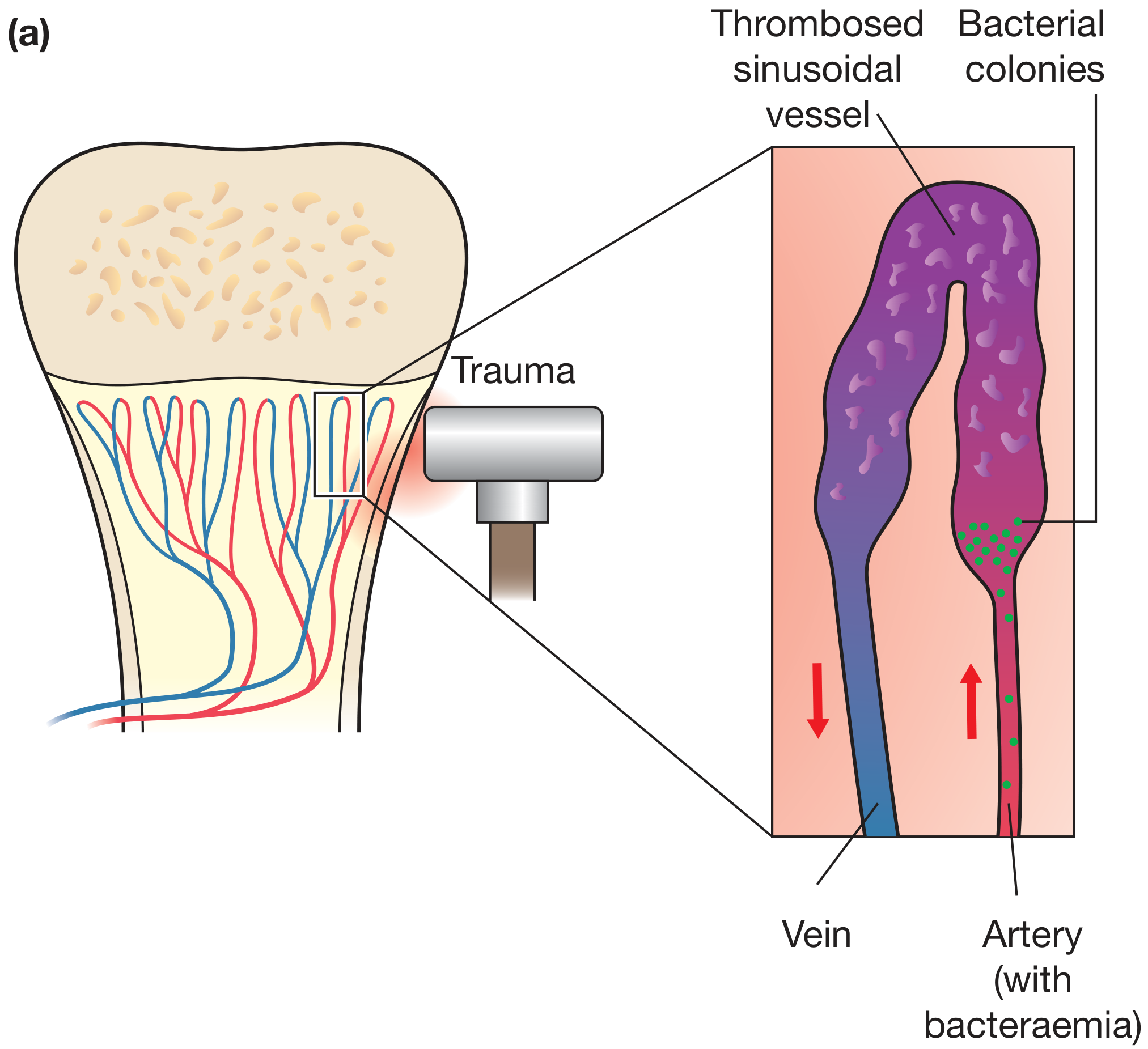
Figure: Pathogenesis of haematogenous osteomyelitis — bacteraemia seeds the artery supplying the metaphysis; microtrauma causes thrombosis of the sinusoidal vessel, and bacterial colonies establish. (Bailey & Love, p. 656)
2. Microbiology
| Setting | Common Organism(s) |
|---|---|
| All ages (most common) | Staphylococcus aureus (80–90% of culture-positive cases) |
| Neonates | Group B Streptococcus, E. coli |
| Children | S. aureus, Streptococcus pyogenes, H. influenzae |
| Sickle cell disease | Salmonella spp. (+ S. aureus) |
| Vertebral (acute) | S. aureus (40–50%), Gram-negative bacilli (E. coli, Pseudomonas), Streptococci |
| IV drug users / Candida | Candida spp., Pseudomonas aeruginosa |
| Subacute/chronic (endemic regions) | Mycobacterium tuberculosis, Brucella spp. |
| Implant-associated | Coagulase-negative staphylococci, Cutibacterium acnes |
S. aureus cell wall proteins bind bone matrix collagen, facilitating bacterial adherence.
— Robbins, p. 991; Harrison's, p. 1106
3. Classification
By Duration
| Type | Characteristics |
|---|---|
| Acute | Days to weeks; predominantly neutrophilic; no bone necrosis → antibiotics alone may suffice |
| Subacute | Weeks to months; includes Brodie's abscess; may present insidiously |
| Chronic | Bone necrosis (sequestrum) present; requires combined antibiotics + surgery |
The presence or absence of bone necrosis (sequestrum), not a specific duration, is the critical determinant guiding management. — Harrison's, p. 1106
Cierny-Mader Classification (Long Bone Osteomyelitis)
The most widely used surgical staging system, classifying by anatomic type and host physiology:
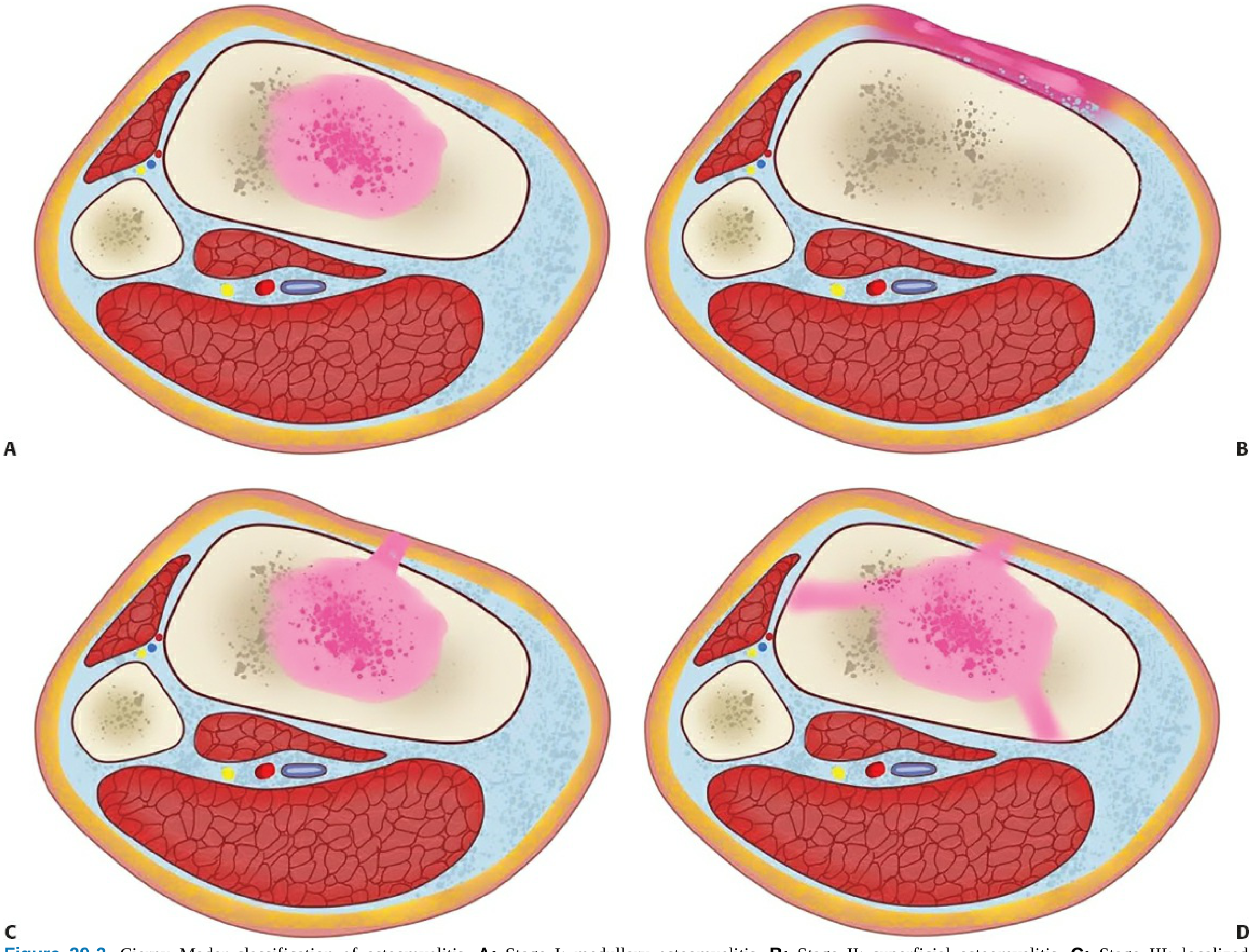
Anatomic Stage:
- Type I — Medullary (endosteal) infection
- Type II — Superficial (cortical surface only)
- Type III — Localized (full-thickness cortex, stable bone)
- Type IV — Diffuse (segmental instability, worst prognosis)
Host Class:
- Class A — Normal immune system and vascularity
- Class B — Locally (BL) or systemically (BS) compromised
- Class C — Treatment worse than disease; suppressive therapy only
Systemic factors: malnutrition, diabetes, renal/hepatic failure, immunosuppression, tobacco/alcohol, extremes of age
Local factors: lymphoedema, venous stasis, major vessel compromise, neuropathy, radiation fibrosis
— Rockwood & Green's Fractures in Adults, 10e
4. Pathological Stages & Morphology
Acute Phase
- Bacteria proliferate → neutrophilic infiltration
- Necrosis of bone cells and marrow within 48 hours
- Infection spreads via Haversian canals to periosteum
- Subperiosteal abscess formation (especially in children)
- Periosteal elevation → impairs blood supply → amplifies necrosis
- Pus formation → pus passes through cortical bone; if periosteum is breached → soft tissue abscess → sinus tract to skin
Chronic Phase
- Sequestrum — devascularised dead bone (hallmark of chronic osteomyelitis)
- Involucrum — periosteal new bone formed around the sequestrum; may encase it → "bone-within-a-bone" appearance
- Brodie's abscess — a subacute form; well-defined lytic lesion with sclerotic rim on imaging; typically in young males
- Sinus tracts — pus tracks through gaps in involucrum to the skin surface
— Robbins, p. 991–992; Bailey & Love, p. 656; Grainger & Allison, p. 1637
5. Clinical Features
Acute Haematogenous Osteomyelitis (Children)
- Fever, malaise, toxaemia
- Localised bone pain, tenderness, erythema, warmth, swelling over the affected metaphysis
- Pseudoparalysis / refusal to bear weight / move limb
- May coexist with sympathetic joint effusion or frank septic arthritis
Vertebral Osteomyelitis (Adults)
- Back pain (most common presenting symptom, >85%)
- Lumbar spine 60%, thoracic 30%, cervical 10%
- Fever in only ~50% of patients (analgesic use blunts this)
- Neurological deficit if epidural abscess complicates
- Primary foci: urinary tract, skin/soft tissue, intravascular catheter, endocarditis
Chronic Osteomyelitis
- Persistent or recurrent pain, discharging sinus tracts, systemic malaise
- Intermittent flares after years of quiescence
6. Investigations
| Investigation | Findings |
|---|---|
| WBC, CRP, ESR | Elevated in acute; CRP is the best marker for treatment response |
| Blood cultures | Positive in ~50% of haematogenous cases — must be obtained before antibiotics |
| Bone biopsy / aspiration | Gold standard for organism identification; always attempt before antibiotics in non-septic patients |
| Plain X-ray | Changes lag 10–14 days behind disease onset; shows soft tissue swelling, cortical irregularity, periosteal reaction, lytic lesions |
| Ultrasound | Best first-line in children; shows subperiosteal fluid, guides aspiration |
| CT | Best for defining cortical destruction and detecting sequestra |
| MRI | Highest sensitivity and specificity; shows bone marrow oedema (T2 hyperintensity), abscess (penumbra sign in subacute), soft tissue involvement, epidural extension; investigation of choice for vertebral osteomyelitis |
| Bone scintigraphy / PET-CT | Useful for multifocal disease; PET-CT increasingly used for implant-associated infection |
Radiographic signs of improvement lag behind clinical recovery even on appropriate therapy. — Grainger & Allison's Diagnostic Radiology, p. 1638
7. Treatment
General Principles
- Obtain microbiological diagnosis before starting antibiotics (blood cultures + bone biopsy) — unless sepsis mandates immediate treatment
- Drain pus whenever present
- Rest and splintage of the affected limb
- Treat underlying conditions (diabetes, malnutrition, sickle cell disease)
Antibiotic Therapy
Empirical therapy targets S. aureus as the most likely pathogen:
- Flucloxacillin (or nafcillin) IV for MSSA
- Vancomycin IV for MRSA or unknown organism in high-risk settings
- Adjust based on culture and sensitivity results
Duration:
- Acute without necrosis: 4–6 weeks total (IV then oral step-down)
- Chronic / with sequestrum: 6+ weeks combined with surgery
- Vertebral osteomyelitis: 6 weeks (RCT evidence — 6 weeks = 12 weeks, cure rate ~91% both groups)
- Implant-associated, early (<30 days): debridement + implant retention + 3 months antibiotics
- Implant-associated, late (>30 days): implant removal + 6 weeks antibiotics
IV vs. Oral:
Evidence from a landmark RCT shows oral antibiotics are non-inferior to IV when: correct spectrum, excellent oral bioavailability, normal GI function, no vomiting. High-bioavailability agents (fluoroquinolones, linezolid, co-trimoxazole) are suitable for oral step-down. A short initial IV course may reduce fluoroquinolone resistance emergence.
— Harrison's, p. 1107; PubMed PMID 40280255
Surgical Treatment
| Indication | Procedure |
|---|---|
| Abscess / subperiosteal collection | Incision and drainage |
| Chronic osteomyelitis with sequestrum | Sequestrectomy + debridement of dead bone (saucerisation) |
| Large bone defect after debridement | Bone grafting, Masquelet technique, distraction osteogenesis |
| Implant-associated infection (late) | Implant removal |
| Vertebral osteomyelitis (most acute haematogenous) | Usually does NOT require surgery |
| Vertebral with neurological deficit, spinal instability, undrained abscess | Surgical decompression / stabilisation |
8. Special Forms
Brodie's Abscess
- Subacute haematogenous osteomyelitis, mainly in young males
- Well-defined lytic cavity with sclerotic rim, most common in tibial metaphysis
- Penumbra sign on MRI (peripheral high-signal granulation tissue surrounding low-signal abscess)
Vertebral / Spinal Osteomyelitis (Spondylodiscitis)
- Most common form of haematogenous osteomyelitis in adults
- MRI shows T2 hyperintensity in disc and adjacent vertebrae + gadolinium enhancement
- Complications: epidural abscess, spinal cord compression, vertebral collapse, psoas abscess
Diabetic Foot Osteomyelitis
- Arises from progressive deep soft tissue infection
- Diagnosis: "probe-to-bone" test (positive = bone felt through ulcer), MRI
- Treatment: prolonged antibiotics ± surgical debridement ± amputation
Tuberculous Osteomyelitis (Pott's Disease)
- Haematogenous spread from primary pulmonary focus
- Predilection for thoracolumbar vertebrae; insidious onset
- Gibbus deformity, psoas abscess, cord compression
- Tuberculosis dactylitis — "spina ventosa" (cyst-like cavities with diaphyseal expansion)
9. Complications
| Complication | Mechanism |
|---|---|
| Septic arthritis | Direct spread from adjacent metaphysis into joint |
| Growth plate damage | Epiphyseal vessel involvement in neonates/infants → limb length discrepancy, angular deformity |
| Pathological fracture | Cortical destruction weakens bone |
| Sinus tracts | Chronic suppuration tracking to skin |
| Squamous cell carcinoma | Rare malignant transformation in long-standing sinus tracts (Marjolin's ulcer) |
| Amyloidosis | Secondary (AA) amyloidosis in chronic infection |
| Epidural abscess / cord compression | Vertebral osteomyelitis |
10. Summary
"Not the duration of infection, but the presence or absence of bone necrosis is crucial. Acute osteomyelitis without bone necrosis can generally be treated with antibiotics alone. In contrast, for chronic osteomyelitis antibiotic treatment should be combined with debridement surgery." — Harrison's Principles of Internal Medicine 22e, p. 1106
Key clinical pearls:
- Always obtain blood cultures and bone biopsy before antibiotics (unless septic)
- MRI is the imaging gold standard
- S. aureus is the cause in ~80–90% of culture-positive cases
- Oral antibiotics are non-inferior to IV when bioavailability is adequate (2025 meta-analysis, PMID 40280255)
- Surgery is required for chronic osteomyelitis with sequestrum, implant-associated infection, and vertebral disease with neurological compromise
Sources:
- Robbins Pathologic Basis of Disease, p. 989–993
- Harrison's Principles of Internal Medicine 22e, pp. 1104–1109
- Bailey & Love's Short Practice of Surgery, 28e, pp. 655–657
- Grainger & Allison's Diagnostic Radiology, p. 1620–1644
- Rockwood & Green's Fractures in Adults, 10e (Cierny-Mader Classification)
- Schwartz's Principles of Surgery, 11e
This is a shared conversation. Sign in to Orris to start your own chat.