60 yr old female known SHTN came with dyspnea for 1 day and pedal edema for 1 week
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Searching PubMed
"heart failure" AND "hypertension" AND "HFpEF"
Loading Image
Reading File
Finding Sources
I now have excellent content from Harrison's, Robbins, Clinical Echocardiography, and Comprehensive Clinical Nephrology. Let me compile a thorough clinical response.
Clinical Case Analysis: 60F with Known Hypertension, Dyspnea (1 day) + Pedal Edema (1 week)
Most Likely Diagnosis
Acute Decompensated Heart Failure (ADHF) secondary to Hypertensive Heart Disease
This is the classic presentation. Long-standing systemic hypertension leads to left ventricular pressure overload, which drives LV hypertrophy and ultimately diastolic and/or systolic dysfunction.
Pathophysiology (Why This Happens)
Hypertension imposes chronic pressure overload on the left ventricle. The LV responds with concentric hypertrophy - an adaptive mechanism that has limits. Per Robbins Pathology:
"Persistent hypertension can eventually culminate in dysfunction, cardiac dilation, CHF, and sudden death... the hypertrophic myocytes fail to contract efficiently, possibly due to structural abnormalities in newly assembled sarcomeres and because the vascular supply is inadequate to meet the demands of the increased muscle mass."
There are two pathways to HF in hypertension, important to distinguish:
| Feature | HFpEF (Diastolic Dysfunction) | HFrEF (Systolic Dysfunction) |
|---|---|---|
| EF | ≥50% (preserved) | ≤40% (reduced) |
| LV size | Concentric hypertrophy, small cavity | Dilated |
| Mechanism | Impaired early diastolic filling → elevated LA pressure → pulmonary venous HTN | Loss of contractility |
| Common in | Early/mid-stage hypertensive disease, older women | Late-stage or coexistent CAD |
This patient - older female with hypertension - has a very high probability of HFpEF. As the echocardiography textbook notes:
"Early in the disease course, pathologic hypertrophy is associated with impaired early diastolic filling. Impaired ventricular filling leads to elevated LA pressures and pulmonary venous hypertension, resulting in dyspnea."
The pedal edema (1 week) reflects chronic venous congestion (right-sided/systemic); the acute dyspnea (1 day) reflects a new trigger causing rapid pulmonary decompensation.
Precipitants to Search For
Per Harrison's, the first principle of ADHF management is identifying the precipitating factor:
- Non-adherence to antihypertensive medications or sodium restriction (most common)
- Uncontrolled hypertension - a "hypertensive ADHF" phenotype (usually NOT volume-overloaded; responds to vasodilators)
- Dietary salt excess
- New arrhythmia (especially atrial fibrillation - common with LA enlargement from chronic HTN)
- Coronary ischemia / ACS - must rule out
- Infection / sepsis (increased cardiac demand)
- NSAIDs or other nephrotoxic/fluid-retaining drugs
- Pulmonary embolism
- New valvular disease
Initial Evaluation
History:
- Symptom progression, orthopnea, PND, weight gain
- Medication compliance (antihypertensives, diuretics)
- Dietary habits (salt intake)
- Palpitations (arrhythmia?)
- Chest pain (ACS?)
Examination:
- BP (likely elevated - hypertensive ADHF), HR, SpO2, RR
- JVP elevation
- Bibasilar crackles
- S3 gallop (volume-overloaded HFrEF) vs S4 (stiff/hypertrophic ventricle, HFpEF)
- Pedal/pitting edema grade
- Hepatomegaly, ascites (right heart congestion)
- Signs of low output: cold extremities, narrow pulse pressure
Investigations:
| Test | Purpose |
|---|---|
| ECG | LVH pattern (voltage criteria), arrhythmia, ischemia |
| Chest X-ray | Cardiomegaly, pulmonary vascular congestion, pleural effusions, Kerley B lines |
| Echocardiogram | Key test - EF (HFpEF vs HFrEF), LV wall thickness, diastolic function grading, valvular disease |
| BNP / NT-proBNP | Confirms HF diagnosis; elevated in both HFpEF and HFrEF; guides prognosis |
| CBC | Anemia as precipitant |
| Renal function + electrolytes | Baseline before diuretics; cardiorenal syndrome |
| Serum troponin | Rule out ACS as trigger |
| Blood glucose / HbA1c | Comorbidities |
| Thyroid function | Hypothyroid can precipitate decompensation |
| Urinalysis | Proteinuria (hypertensive nephropathy) |
ADHF Phenotypes and Management (Harrison's Fig. 265-2)
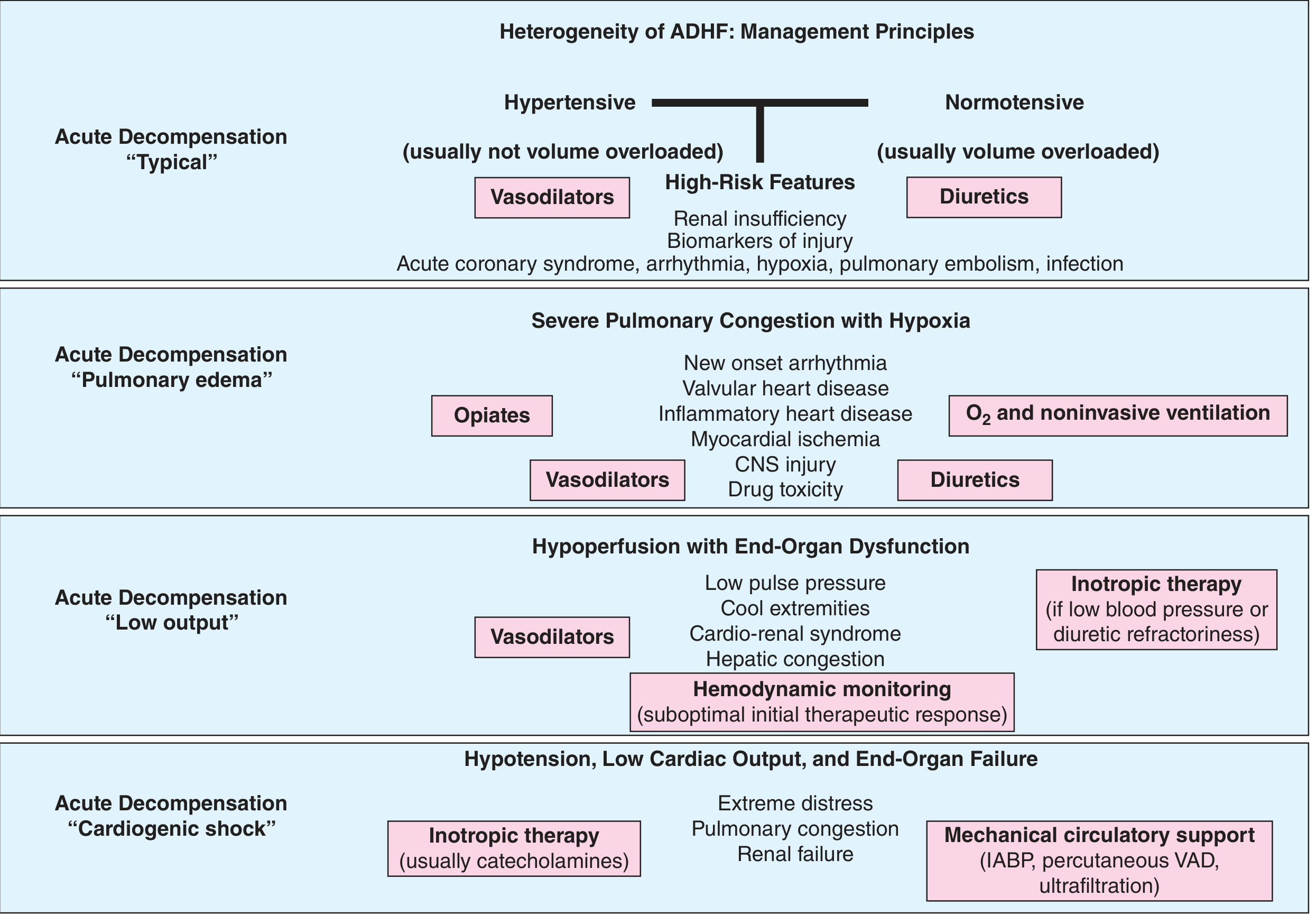
This patient most likely fits the "Hypertensive ADHF" phenotype (top-left of figure):
- Acute dyspnea, elevated BP, redistribution pulmonary edema (often NOT truly volume-overloaded)
- Primary treatment: Vasodilators (reduce afterload rapidly) + supplemental O2
- If volume-overloaded: IV diuretics
Acute Management
1. Oxygen / Ventilatory Support
- Target SpO2 >94%
- High-flow O2, consider non-invasive ventilation (CPAP/BiPAP) if severe hypoxia or respiratory distress - reduces preload and work of breathing
2. Vasodilators (Hypertensive ADHF - priority)
- IV Nitroglycerine (sublingual first, then infusion) - reduces preload and afterload, relieves pulmonary congestion rapidly
- IV Nitroprusside - more potent afterload reduction if BP very high
3. IV Loop Diuretics (if volume-overloaded)
- Furosemide IV - rapid onset, natriuresis and venodilatation
- Monitor urine output, daily weights, electrolytes
- If refractory: add metolazone (sequential nephron blockade) - watch for hypokalemia
4. Monitor for Cardiorenal Syndrome
Per Harrison's: ~30% of ADHF patients have renal impairment at baseline. Worsening creatinine during diuresis requires hemodynamic reassessment.
Longer-Term Management (Post-Stabilization)
For HFpEF (likely in this patient)
Per Comprehensive Clinical Nephrology:
"BP lowering is commonly required in patients with HFpEF. If volume overload is present, diuretics will be required."
Guideline-directed therapy for HFpEF + HTN:
- BP control to target (<130/80 mmHg)
- Loop/thiazide diuretics for congestion control
- SGLT2 inhibitors (empagliflozin/dapagliflozin) - now shown to reduce HF hospitalizations in HFpEF regardless of diabetes status (Harrison's 2025)
- Mineralocorticoid receptor antagonists (spironolactone) - variable evidence, may reduce HF hospitalizations
- Sacubitril/valsartan (ARNI) - emerging data in HFpEF, better evidence in HFrEF
- GLP-1 agonists - newer data in obese HFpEF patients
For HFrEF (if EF is reduced)
Per Comprehensive Clinical Nephrology - the "4 pillars":
- ACEi/ARB or ARNI (sacubitril/valsartan preferred)
- Beta-blocker (carvedilol, bisoprolol, metoprolol succinate)
- Mineralocorticoid receptor antagonist (spironolactone/eplerenone)
- SGLT2 inhibitor
- Avoid: Non-DHP calcium channel blockers (diltiazem, verapamil), alpha-blockers, moxonidine in HF
Red Flags Requiring Urgent Action
- SpO2 <90% despite O2 → BiPAP / intubation
- SBP <90 mmHg → cardiogenic shock protocol (inotropes, mechanical support)
- ACS on ECG/troponin → urgent cardiology consult
- New AF with fast ventricular rate → rate control / cardioversion
- BUN >43 mg/dL + Cr >2.75 mg/dL + SBP <115 mmHg → worse prognosis, escalate monitoring
Summary
| Aspect | Key Point |
|---|---|
| Likely diagnosis | Acute decompensated HF (hypertensive - probable HFpEF) |
| Mechanism | HTN → LVH → diastolic dysfunction → elevated LVEDP → pulmonary venous HTN |
| Priority investigations | ECG, CXR, Echo, BNP, troponin, renal function |
| Acute treatment | O2, IV nitroglycerin (vasodilator), IV furosemide |
| Disease-modifying (HFpEF) | BP control, SGLT2 inhibitor, diuretics, possibly spironolactone |
| Disease-modifying (HFrEF) | ARNI + BB + MRA + SGLT2i ("4 pillars") |
Sources:
- Harrison's Principles of Internal Medicine, 22e (2025) - ADHF chapter
- Comprehensive Clinical Nephrology, 7th ed. - Hypertension in HF
- Textbook of Clinical Echocardiography - Hypertensive heart disease & diastolic dysfunction
- Robbins & Kumar Basic Pathology - Hypertensive heart disease pathology
- Recent PubMed: Systematic review on HFpEF phenotyping in device trials (PMID 40857067, 2025) and meta-analysis on BP and pulse pressure in HF (PMID 39745404, 2025 JACC)
This is a shared conversation. Sign in to Orris to start your own chat.