Hepatolithiasis
Reading File
Finding Sources
Finding Sources
Searching PubMed
hepatolithiasis management treatment
Reading File
Reading File
Reading File
Reading File
Searching PubMed
hepatolithiasis intrahepatic stones
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
I now have thorough coverage from multiple authoritative textbooks. Here is a comprehensive answer.
Hepatolithiasis
Hepatolithiasis refers to stones located in the intrahepatic bile ducts - specifically above the confluence of the left and right hepatic ducts. Once called "recurrent pyogenic cholangitis" or "Oriental cholangiopathy," it is a distinct and often challenging biliary disease.
Epidemiology
- Highly prevalent in East Asia (China, Taiwan, Japan, Korea, Southeast Asia) and their emigrant populations worldwide; rare in the West.
- In Western populations, most ductal stones are extrahepatic; intrahepatic stones, when they do occur, are usually secondary to other biliary pathology.
- Affects both sexes equally.
- Approximately 20% of patients remain asymptomatic (Japanese survey data).
- 70% of patients with hepatolithiasis do NOT have gallstones.
Etiology & Pathogenesis
The exact cause is uncertain in most cases. Contributing factors include:
- Chronic biliary stasis - the central mechanism, leading to stone nucleation
- Biliary strictures (benign, postoperative, or associated with PSC)
- Recurrent pyogenic cholangitis (RPC) - bile duct strictures cause proximal stasis → recurrent cholangitis → pyogenic inflammation → de novo pigment stone formation. Transient portal bacteremia transfers organisms to the bile ducts, facilitating stone growth. Causative organisms: E. coli, Klebsiella, Proteus, Pseudomonas, anaerobes.
- Choledochal cysts / Caroli disease
- Biliary parasites (Clonorchis sinensis, Opisthorchis viverini)
- Congenital duct abnormalities
- Defects in hepatic phospholipid transporters (proposed)
- Diet has also been implicated
Stone Composition
- Predominantly pigmented calcium bilirubinate stones (brown pigment stones) - distinct from the cholesterol stones typical of Western gallstone disease.
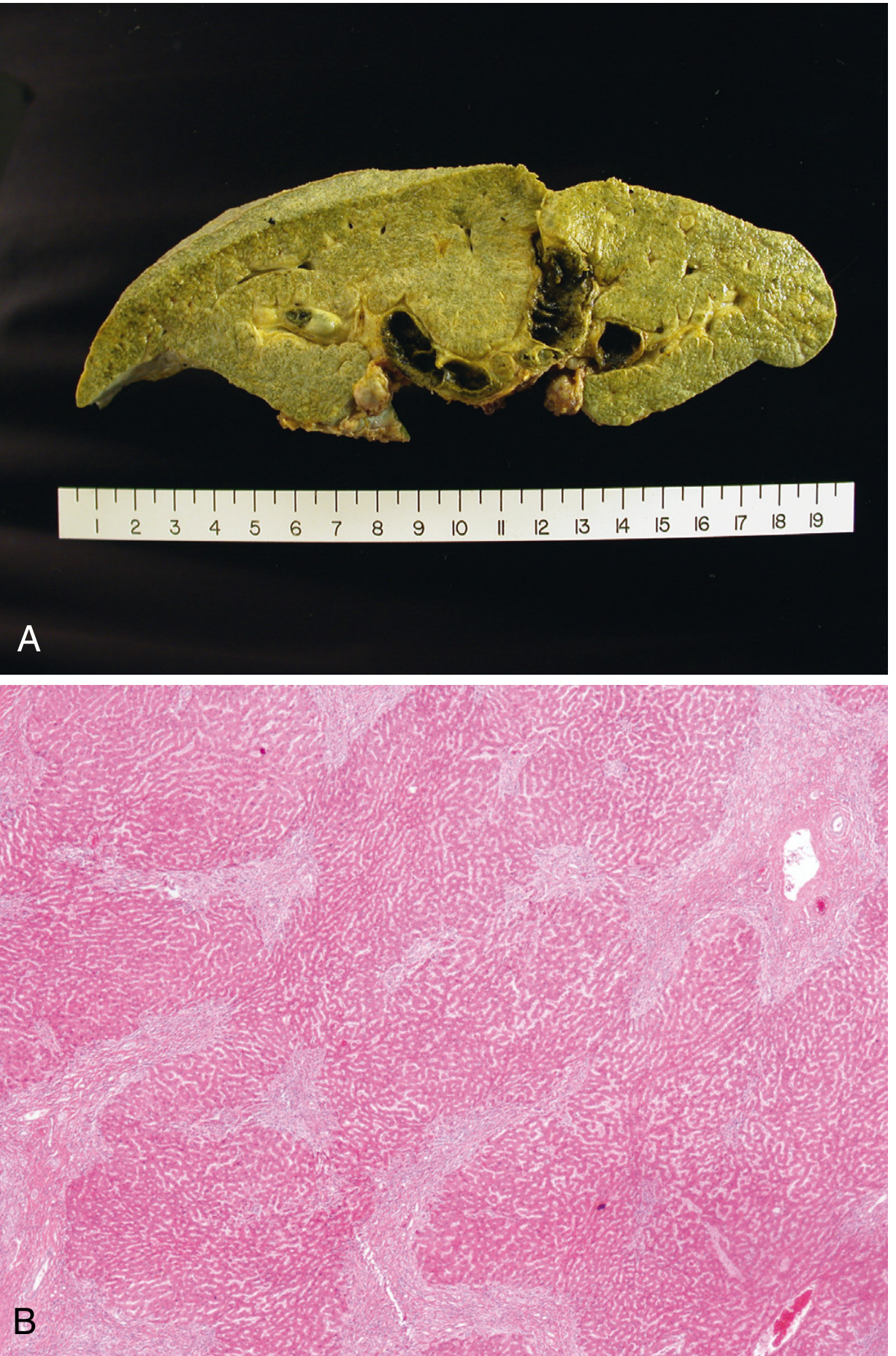
Pathology (Morphology)
- Distended intrahepatic bile ducts containing pigmented calcium bilirubinate stones
- Duct wall: chronic inflammation, mural fibrosis, peribiliary gland hyperplasia
- No obstruction of the extrahepatic ducts (primary disease)
- Repeated bouts of inflammation → parenchymal collapse and fibrosis → can produce a mass-like lesion mimicking tumor on imaging
Clinical Presentation
- Recurrent ascending cholangitis - the hallmark: fever, right upper quadrant pain, jaundice (Charcot's triad)
- Severity ranges from mild to life-threatening sepsis
- Hepatic abscess formation
- Progressive hepatic parenchymal destruction, biliary cirrhosis
- Liver failure (late)
- 20% can remain asymptomatic
Classification
Two widely used systems:
Japanese Classification (by location)
| Type | Description |
|---|---|
| Type I | Intrahepatic stones alone |
| Type IE | Intra- and extrahepatic ductal stones |
| Type L | Left-sided intrahepatic ductal stones |
| Type R | Right-sided intrahepatic ductal stones |
| Type C | Caudate lobe stones |
Takada Classification (by stricture pattern)
| Type | Description |
|---|---|
| Type I | No stricture, mild biliary dilatation |
| Type II | Distal CBD/ampullary stricture |
| Type III | Hilar stricture |
| Type IV | Unilateral hepatic duct stricture |
| Type V | Multiple bilateral strictures |
| Type VI | Multiple strictures |
- Mulholland and Greenfield's Surgery, p. 3081
Diagnosis
Multiple modalities are available:
| Modality | Role |
|---|---|
| Ultrasound (US) | First-line; detects stones, duct dilatation |
| CT | Defines distribution, strictures, atrophy, cholangiocarcinoma |
| MRCP | Non-invasive biliary mapping; preferred for defining anatomy |
| ERCP | Invasive; therapeutic as well as diagnostic |
| Percutaneous transhepatic cholangiography (PTC) | Used when ERCP fails or anatomy is altered |
- Imaging features are similar to extrahepatic stones (filling defects, upstream dilatation)
- CT/MRI may show lobar atrophy in long-standing cases
- A mass-like lesion must raise suspicion for cholangiocarcinoma
Complications
- Recurrent ascending cholangitis - the most common complication
- Liver abscess
- Biliary cirrhosis and portal hypertension
- Cholangiocarcinoma - incidence 5-10% in patients with hepatolithiasis; particularly high risk in Taiwan, also Japan. Hepatolithiasis is a known risk factor alongside PSC, choledochal cysts, and Opisthorchis infection. Stone removal may reduce this risk.
- Liver failure
- Lobar atrophy from chronic obstruction
Management
Acute Phase
- Resuscitation and treatment of cholangitis (IV antibiotics, fluid support)
- Biliary drainage - percutaneous or endoscopic, depending on stone location and stricture distribution
Definitive Treatment
1. Endoscopic (ERCP)
- For accessible stones, especially those near the hilum
- Cholangioscopy (SpyGlass or similar) with electrohydraulic lithotripsy (EHL) or laser lithotripsy often required given the proximal location
- ESWL may be used as adjunct to fragment stones for ERCP retrieval
- Limitations: high recurrence; may not be feasible in complex bilateral or stricture-associated disease
2. Percutaneous Transhepatic Choledochoscopy (PTCS)
- Particularly valuable when ERCP access is limited
- Direct cholangioscopic stone removal via a transhepatic tract
- Recent evidence supports this as an effective approach for difficult hepatolithiasis
3. Surgery - the preferred definitive option in many cases
- Hepatectomy (partial/segmental): indicated when
- Stones are limited to one lobe/segment with atrophy or irreversible parenchymal damage
- Concern for cholangiocarcinoma
- Failed endoscopic/percutaneous approaches
- Recurrent pyogenic cholangitis confined to a segment
- Hepaticojejunostomy (Roux-en-Y) ± anchoring the jejunal limb to the abdominal wall (creates a "hepaticojejunostomy access loop") for future percutaneous stone retrieval
- Transduodenal sphincteroplasty for impacted stones at the ampulla, primary duct stones, or benign distal strictures
Key Decision Points for ERCP vs Surgery
- Is segmental hepatectomy the better option (e.g., RPC, lobar atrophy, cholangiocarcinoma risk)?
- Is there underlying cholangiopathy or malignancy?
- What is the distribution and number of strictures (Takada classification guides this)?
- Clinical Gastrointestinal Endoscopy, p. 1571
Recurrence
- Recurrence rates are high even after complete stone clearance
- Rates vary widely in the literature (0% to >50%)
- This drives the preference for surgery with biliary enteric bypass in appropriate patients, allowing future percutaneous access
Key Associations - Risk Factors for Cholangiocarcinoma
| Condition |
|---|
| Primary sclerosing cholangitis (PSC) |
| Choledochal cyst disease |
| Hepatolithiasis |
| Recurrent pyogenic cholangitis |
| Opisthorchis viverini infection |
| Thorotrast exposure |
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
Summary
Hepatolithiasis is a predominantly East Asian disease of intrahepatic pigment stone formation, driven by biliary stasis, strictures, and chronic infection/inflammation. Its natural history includes recurrent cholangitis, progressive hepatic destruction, and a significant risk of cholangiocarcinoma (5-10%). Management is stepwise - acute cholangitis first, then definitive therapy which is often surgical (segmental hepatectomy ± biliary-enteric bypass) given high endoscopic recurrence rates. Classification by the Japanese or Takada systems guides treatment planning.
Recent literature (2024): A comprehensive review (Motta et al., PMID 38659478, World J Gastroenterol 2024) covers the full epidemiology, classification, and management of hepatolithiasis. A surgical evolution review (Ye et al., PMID 39734463, World J Gastrointest Surg 2024) and a narrative review on percutaneous transhepatic choledochoscopy (Wang & Wu, PMID 39022230, Quant Imaging Med Surg 2024) reflect current practice trends.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Mulholland and Greenfield's Surgery (7e); Clinical Gastrointestinal Endoscopy (3e); Yamada's Textbook of Gastroenterology (7e); Grainger & Allison's Diagnostic Radiology; Sleisenger and Fordtran's GI and Liver Disease; Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.