Abg from basics to clinicals
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content. Let me compose the full ABG guide.
Arterial Blood Gas (ABG) - Basics to Clinicals
1. Why pH Matters
The body maintains blood pH between 7.35-7.45 (normal = 7.40). This narrow range is critical because H⁺ ions alter the charge and conformation of proteins - enzymes, receptors, ion channels, and structural proteins all change behavior with pH shifts. Even a shift of 0.3 pH units represents a 2-fold change in [H⁺], and a shift of 1.0 unit = a 10-fold change.
- pH < 7.35 = acidemia
- pH > 7.45 = alkalemia
The -emia suffix describes the blood state; the -osis suffix describes the process causing it.
2. The Henderson-Hasselbalch Framework
The central equation governing ABG interpretation:
CO₂ + H₂O ⇌ H₂CO₃ ⇌ HCO₃⁻ + H⁺
Two variables are under physiological control:
- PaCO₂ - controlled by the lungs (respiratory)
- HCO₃⁻ - controlled by the kidneys (metabolic)
| Parameter | Normal Value |
|---|---|
| pH | 7.35-7.45 (ideal 7.40) |
| PaCO₂ | 35-45 mm Hg (ideal 40) |
| HCO₃⁻ | 22-26 mEq/L (ideal 24) |
| PaO₂ | 80-100 mm Hg |
| Base Excess (BE) | -2 to +2 mEq/L |
| SpO₂ | 95-100% |
3. The Three Buffer Systems
The body uses three overlapping systems to resist pH change:
- Bicarbonate buffer (extracellular, dominant) - responds within minutes via respiratory adjustment
- Protein buffers (hemoglobin, albumin, intracellular proteins) - immediate buffering
- Phosphate buffer (intracellular and renal) - key for urinary acid excretion
Medical Physiology, Boron
4. Normal Compensatory Responses
When a primary disorder occurs, the body compensates to push pH back toward normal (never fully corrects it). The rule: compensation brings pH toward normal, but never past 7.40.
| Primary Disorder | Compensation | Mechanism |
|---|---|---|
| Metabolic acidosis | ↑ ventilation → ↓ PaCO₂ | Respiratory (minutes-hours) |
| Metabolic alkalosis | ↓ ventilation → ↑ PaCO₂ | Respiratory (minutes-hours) |
| Respiratory acidosis | ↑ renal HCO₃⁻ reabsorption | Renal (3-5 days) |
| Respiratory alkalosis | ↓ renal HCO₃⁻ reabsorption | Renal (3-5 days) |
Roberts and Hedges' Clinical Procedures in Emergency Medicine
5. Stepwise ABG Interpretation
Step 1 - Assess the pH
- pH < 7.35 → Acidosis
- pH > 7.45 → Alkalosis
- pH = 7.35-7.45 → May still have a mixed disorder
Step 2 - Identify the Primary Disorder
Look at PaCO₂ and HCO₃⁻ together:
| Finding | Primary Disorder |
|---|---|
| pH ↓, HCO₃⁻ < 24 | Metabolic acidosis |
| pH ↓, PaCO₂ > 40 | Respiratory acidosis |
| pH ↑, HCO₃⁻ > 24 | Metabolic alkalosis |
| pH ↑, PaCO₂ < 40 | Respiratory alkalosis |
The parameter that "matches" the pH direction is the primary driver. For example: acidosis (pH ↓) with high PaCO₂ = respiratory acidosis.
Symptom to Diagnosis, 4th Ed
Step 3 - Calculate the Anion Gap (for metabolic acidosis)
Anion Gap (AG) = Na⁺ - (HCO₃⁻ + Cl⁻) Normal = 12 ± 4 mEq/L (some labs: 7-9 mEq/L)
An elevated AG indicates accumulation of unmeasured anions.
Albumin correction (critical in hypoalbuminemia):
- Corrected AG = Measured AG + 2.5 × (4.4 - serum albumin in g/dL)
- Failure to correct will miss high-AG acidosis in critically ill patients with low albumin.
High AG metabolic acidosis - mnemonic MUDPILES (or GOLD MARK):
| MUDPILES | GOLD MARK (modern) |
|---|---|
| Methanol | Glycols (ethylene, propylene) |
| Uremia | Oxoproline (pyroglutamic acid) |
| DKA | Lactic acidosis |
| Propylene glycol | D-lactic acidosis |
| Isoniazid / Iron | Methanol |
| Lactic acidosis | Aspirin (salicylates) |
| Ethylene glycol | Renal failure (uremia) |
| Salicylates | Ketoacidosis |
Normal AG (hyperchloremic) metabolic acidosis - mnemonic HARDUP:
- Hyperalimentation
- Acetazolamide / carbonic anhydrase inhibitors
- Renal tubular acidosis (RTA)
- Diarrhea (GI HCO₃⁻ loss - most common)
- Ureteral diversion
- Pancreatic fistula
Symptom to Diagnosis, 4th Ed
Step 4 - Check Compensation (is it adequate?)
Use these formulas to determine if the compensation is appropriate. If actual compensation differs from predicted, a second disorder is present.
| Primary Disorder | Expected Compensation Formula |
|---|---|
| Metabolic acidosis | PaCO₂ = 1.5 × HCO₃⁻ + 8 ± 2 (Winter's formula) OR ↓PaCO₂ = 1.2 × ↓HCO₃⁻ |
| Metabolic alkalosis | ↑PaCO₂ = 0.7 × ↑HCO₃⁻ (or ↑0.6 per 1 mEq/L ↑HCO₃⁻) |
| Respiratory acidosis (acute) | ↑HCO₃⁻ = 1 mEq/L per 10 mm Hg ↑PaCO₂ |
| Respiratory acidosis (chronic) | ↑HCO₃⁻ = 4 mEq/L per 10 mm Hg ↑PaCO₂ |
| Respiratory alkalosis (acute) | ↓HCO₃⁻ = 2 mEq/L per 10 mm Hg ↓PaCO₂ |
| Respiratory alkalosis (chronic) | ↓HCO₃⁻ = 4 mEq/L per 10 mm Hg ↓PaCO₂ |
Winter's formula trick: Expected PaCO₂ ≈ last two digits of expected pH.
- If measured PaCO₂ > expected → additional respiratory acidosis
- If measured PaCO₂ < expected → additional respiratory alkalosis (e.g., salicylate poisoning)
Roberts and Hedges' Clinical Procedures in Emergency Medicine
Step 5 - Delta-Delta Ratio (for high AG metabolic acidosis)
Delta ratio = ΔAG / ΔHCO₃⁻ = (Measured AG - 12) / (24 - Measured HCO₃⁻)
| Delta Ratio | Interpretation |
|---|---|
| < 0.4 | Pure normal-AG (hyperchloremic) acidosis |
| 0.4-1.0 | Mixed: high AG + normal AG acidosis (e.g., DKA + diarrhea) |
| 1-2 | Pure high AG metabolic acidosis (expected) |
| > 2 | Mixed: high AG acidosis + concurrent metabolic alkalosis (e.g., DKA + vomiting) |
Miller's Anesthesia, 10th Ed
Step 6 - Assess Oxygenation
- PaO₂ normal: 80-100 mm Hg on room air
- A-a gradient = PAO₂ - PaO₂
- PAO₂ = (FiO₂ × 713) - (PaCO₂ / 0.8)
- Normal A-a gradient ≈ age/4 mm Hg (or < 10-15 on room air)
- Elevated A-a gradient → intrinsic lung disease (V/Q mismatch, shunt, diffusion defect)
- Normal A-a gradient + hypoxemia → hypoventilation (pure PaCO₂ problem)
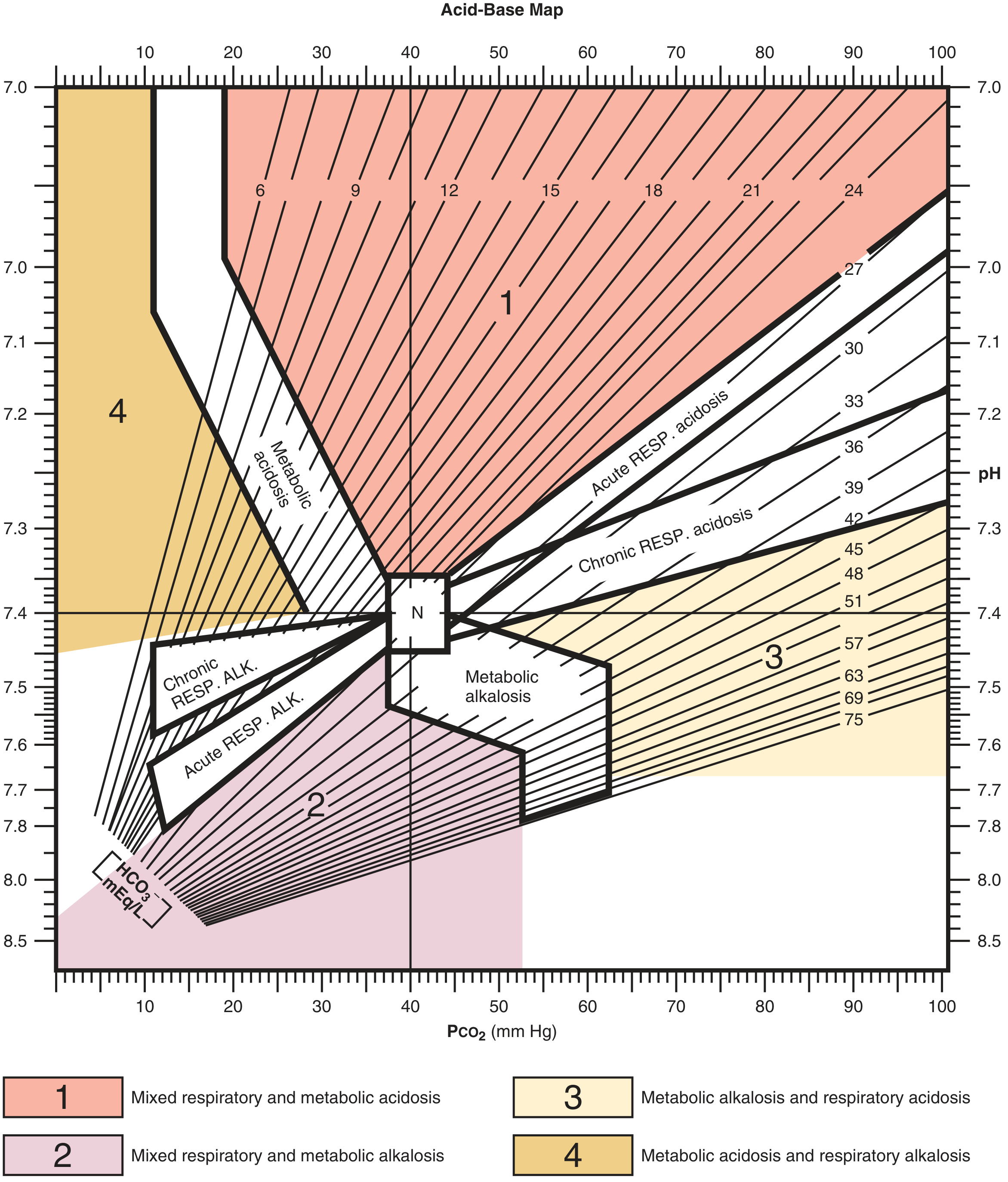
6. The Acid-Base Map
This map plots pH vs PaCO₂ with confidence bands for each pure disorder. Points falling inside the bands = simple disorder; points in the colored zones between bands = mixed disorders.
Roberts and Hedges' Clinical Procedures in Emergency Medicine
7. The Four Primary Disorders - Clinical Details
A. Metabolic Acidosis
Mechanism: Gain of H⁺ (consuming HCO₃⁻) or direct loss of HCO₃⁻
ABG pattern: ↓pH, ↓HCO₃⁻, ↓PaCO₂ (compensation)
Kussmaul breathing - deep, labored, rapid respirations - is the clinical sign of severe metabolic acidosis compensation.
Clinical causes by AG:
| High AG | Normal AG |
|---|---|
| DKA (fruity breath, glucosuria, ketonemia) | Diarrhea (most common) |
| Lactic acidosis (shock, sepsis, hypoxia) | RTA |
| Uremia (chronic kidney disease) | Acetazolamide |
| Salicylate OD (mixed high AG + respiratory alkalosis) | Post-hypocapnia |
| Methanol / ethylene glycol (elevated osmol gap) |
B. Metabolic Alkalosis
Mechanism: Loss of H⁺ or gain of HCO₃⁻
ABG pattern: ↑pH, ↑HCO₃⁻, ↑PaCO₂ (compensation - hypoventilation)
Classification by urine chloride (clinically useful):
| Saline-responsive (UCl < 20 mEq/L) | Saline-resistant (UCl > 20 mEq/L) |
|---|---|
| Vomiting / NG suction | Primary hyperaldosteronism |
| Loop / thiazide diuretics | Cushing's syndrome |
| Post-hypercapnia | Severe hypokalemia |
| Contraction alkalosis | Excess licorice ingestion |
C. Respiratory Acidosis
Mechanism: ↓ alveolar ventilation → CO₂ retention → ↑H⁺
ABG pattern: ↓pH, ↑PaCO₂, ↑HCO₃⁻ (renal compensation - delayed 3-5 days)
Acute vs Chronic:
- Acute: HCO₃⁻ rises only ~1 mEq/L per 10 mm Hg PaCO₂ rise (buffering only)
- Chronic: HCO₃⁻ rises ~4 mEq/L per 10 mm Hg (full renal compensation)
Causes by location:
| CNS (drive) | Airway/Lung | Neuromuscular |
|---|---|---|
| Opiates, sedatives | COPD | Guillain-Barré |
| Brainstem stroke | Severe asthma | Myasthenia gravis |
| Sleep apnea | Pulmonary edema | ALS, polio |
| Pneumothorax | Flail chest |
D. Respiratory Alkalosis
Mechanism: Hyperventilation → ↓CO₂ → ↓H⁺
ABG pattern: ↑pH, ↓PaCO₂, ↓HCO₃⁻ (renal compensation)
Causes:
- Anxiety / pain / fever
- Pulmonary embolism (common, reflex hyperventilation)
- Pregnancy (progesterone stimulates breathing)
- Hepatic failure / cirrhosis
- Salicylate toxicity (early - before acidosis dominates)
- Mechanical ventilation (iatrogenic)
- CNS insult (meningitis, stroke)
8. Mixed Disorders - Clinical Scenarios
| Clinical Scenario | ABG Pattern |
|---|---|
| Septic shock | Met acidosis (lactic) + Resp alkalosis (reflex hyperventilation) |
| DKA + vomiting | High AG met acidosis + Met alkalosis (delta ratio > 2) |
| COPD exacerbation + diuretics | Resp acidosis + Met alkalosis |
| Salicylate OD | High AG met acidosis + Resp alkalosis |
| Cardiac arrest | Resp acidosis + Met acidosis (zone 1 on map) |
| Cirrhosis on diuretics | Resp alkalosis + Met alkalosis |
The "N" (normal point) on the acid-base map is where pH = 7.4, PaCO₂ = 40. Points falling in the numbered colored zones outside confidence bands indicate mixed disorders.
9. A Worked Clinical Example
Patient: 28-year-old with Type 1 DM, 2 days of vomiting, orthostatic hypotension.
Labs: Na⁺ 138, K⁺ 6.2, Cl⁻ 100, HCO₃⁻ 6, glucose 389, pH 7.10, PaCO₂ 15
Step 1: pH 7.10 → Acidosis
Step 2: HCO₃⁻ 6 (< 24) with pH down → Metabolic acidosis as primary
Step 3: AG = 138 - (6 + 100) = 32 → High AG metabolic acidosis → DKA
Step 4 (Winter's): Expected PaCO₂ = 1.5(6) + 8 = 17 ± 2 → Actual PaCO₂ = 15 → within expected range, pure compensation, no second respiratory disorder
Step 5 (Delta-delta): (32-12)/(24-6) = 20/18 = 1.1 → Pure high-AG acidosis; however, history of vomiting raises concern for a concurrent metabolic alkalosis masking an even lower HCO₃⁻.
Diagnosis: DKA (primary high AG metabolic acidosis with appropriate respiratory compensation)
Symptom to Diagnosis, 4th Ed
10. Quick Reference Card
ABG Normal Values
─────────────────────────────────────
pH 7.35 – 7.45
PaCO₂ 35 – 45 mm Hg
HCO₃⁻ 22 – 26 mEq/L
PaO₂ 80 – 100 mm Hg
BE -2 to +2 mEq/L
STEP-BY-STEP
1. pH → acidemia / alkalemia?
2. Match PaCO₂ or HCO₃⁻ to direction → primary disorder
3. If met acidosis: AG = Na - (Cl + HCO₃)
Correct for albumin: +2.5 per g/dL below 4.4
4. Check compensation (Winter's, tables above)
Mismatch = second disorder
5. If high AG: Delta ratio = ΔAG / ΔHCO₃
<0.4 = NAGMA; 1-2 = pure HAGMA; >2 = HAGMA + met alk
6. A-a gradient for oxygenation assessment
Sources:
- Medical Physiology (Boron & Boulpaep) - acid-base physiology
- Symptom to Diagnosis: An Evidence-Based Guide, 4th Ed - stepwise approach
- Roberts and Hedges' Clinical Procedures in Emergency Medicine - compensation tables and worked examples
- Miller's Anesthesia, 10th Ed - delta ratio and base excess
- Comprehensive Clinical Nephrology, 7th Ed - mixed disorders
This is a shared conversation. Sign in to Orris to start your own chat.