Metal reaction explain in detail with causes of it signs and symptoms and prevention and treatment for it with appropriate images and illustration
Reading File
Finding Sources
Finding Sources
Searching the Web
metal hypersensitivity reaction causes signs symptoms treatment prevention
Reading File
Reading File
Finding Sources
Loading Image
Searching the Web
metal allergy nickel cobalt chromium type IV hypersensitivity mechanism pathophysiology diagram
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have everything needed to write a comprehensive, well-illustrated answer. Let me compile it all.
Metal Reaction (Metal Hypersensitivity) - A Complete Guide
What Is a Metal Reaction?
A metal reaction (also called metal hypersensitivity or metal allergy) is an immune-mediated adverse response triggered when the body's immune system recognizes certain metal ions as foreign. It is classified as a Type IV (delayed-type) hypersensitivity reaction - cell-mediated rather than antibody-driven - which explains why it does not cause the immediate sneezing, watery eyes, or anaphylaxis seen with typical allergies.
"Allergic contact dermatitis (ACD) is a cell-mediated (type IV), delayed type, hypersensitivity reaction caused by skin contact with an environmental allergen. Prior sensitization is required for allergy to develop." - Fitzpatrick's Dermatology, 5e
Metal reactions affect approximately 21.2% of the general population for at least one metal allergen, with nickel being the single most prevalent contact allergen worldwide (sensitization rates of 18-30%).
Causative Metals
The most common metal offenders include:
| Metal | Common Sources |
|---|---|
| Nickel | Jewelry, belt buckles, zippers, coins, cell phones, eyeglass frames, orthopedic implants |
| Cobalt | Jewelry alloys, paints, tattoo inks, vitamin B12, prosthetic joints |
| Chromium (hexavalent) | Cement, leather (tanned), tools, chrome plating |
| Copper | Coins, IUDs, plumbing fixtures |
| Gold | Jewelry, dental fillings |
| Palladium | Dental alloys, jewelry |
| Beryllium | Industrial/occupational exposure (aerospace, electronics) |
| Arsenic | Contaminated water, pesticides, industrial exposure |
| Mercury | Dental amalgams, certain vaccines, industrial exposure |
| Titanium | Implants, surgical devices (less common but reported) |
From Dermatology 2-Volume Set, 5e (Table 88.12), additional metals with cutaneous hazards include aluminum (vaccine hypersensitivity), barium, bismuth, cadmium, cesium, thallium, tin, and zirconium.
Pathophysiology (Mechanism)
Metal hypersensitivity follows the Type IV (delayed-type) hypersensitivity pathway. There are two distinct phases:
Phase 1 - Sensitization (10-25 days, asymptomatic)
Metal ions (haptens) are too small to be immunogenic alone. They penetrate the skin and bind to endogenous carrier proteins, forming a complete hapten-protein antigen complex. This triggers the following cascade:
- Keratinocytes release pro-inflammatory cytokines: IL-1, IL-8, IL-18, TNF-α, and GM-CSF
- Langerhans cells (epidermal dendritic cells) and dermal dendritic cells take up the hapten-protein complex
- These antigen-presenting cells migrate via lymphatics to regional lymph nodes
- In lymph nodes, they present the antigen on MHC class II molecules to naïve CD4+ T cells (and MHC class I to CD8+ T cells)
- Naïve T cells are primed, differentiate into memory effector T cells (Th1/Tc1), clonally expand, acquire skin-homing antigens, and enter circulation
"The sensitization phase generally lasts 10 to 25 days and often is asymptomatic." - Fitzpatrick's Dermatology, 5e
Phase 2 - Elicitation (Re-exposure: symptoms in 12-72 hours)
On re-exposure to the metal:
- Low-grade non-specific inflammation activates toll-like receptors
- Neutrophils are recruited first, then antigen-specific effector T cells are recruited to the skin
- Effector T cells recognize the hapten-antigen complex presented by local Langerhans/dendritic cells
- T cells release IFN-γ and TNF-α, stimulating macrophages and keratinocytes to release more cytokines
- Monocytes migrate in, mature into activated macrophages, attracting more T cells
- Visible inflammatory response (eczema, vesicles, edema) develops, typically peaking at 48-72 hours

Type IV cell-mediated hypersensitivity cascade - the immunological basis of metal allergy
DTH Response Mechanism Diagrams
The following textbook diagrams illustrate the delayed-type hypersensitivity response underlying metal allergy:
Step 1 - TH1 cell activation by macrophage antigen presentation, releasing chemokines, cytokines (IFN-γ, TNF-α), and cytotoxins:
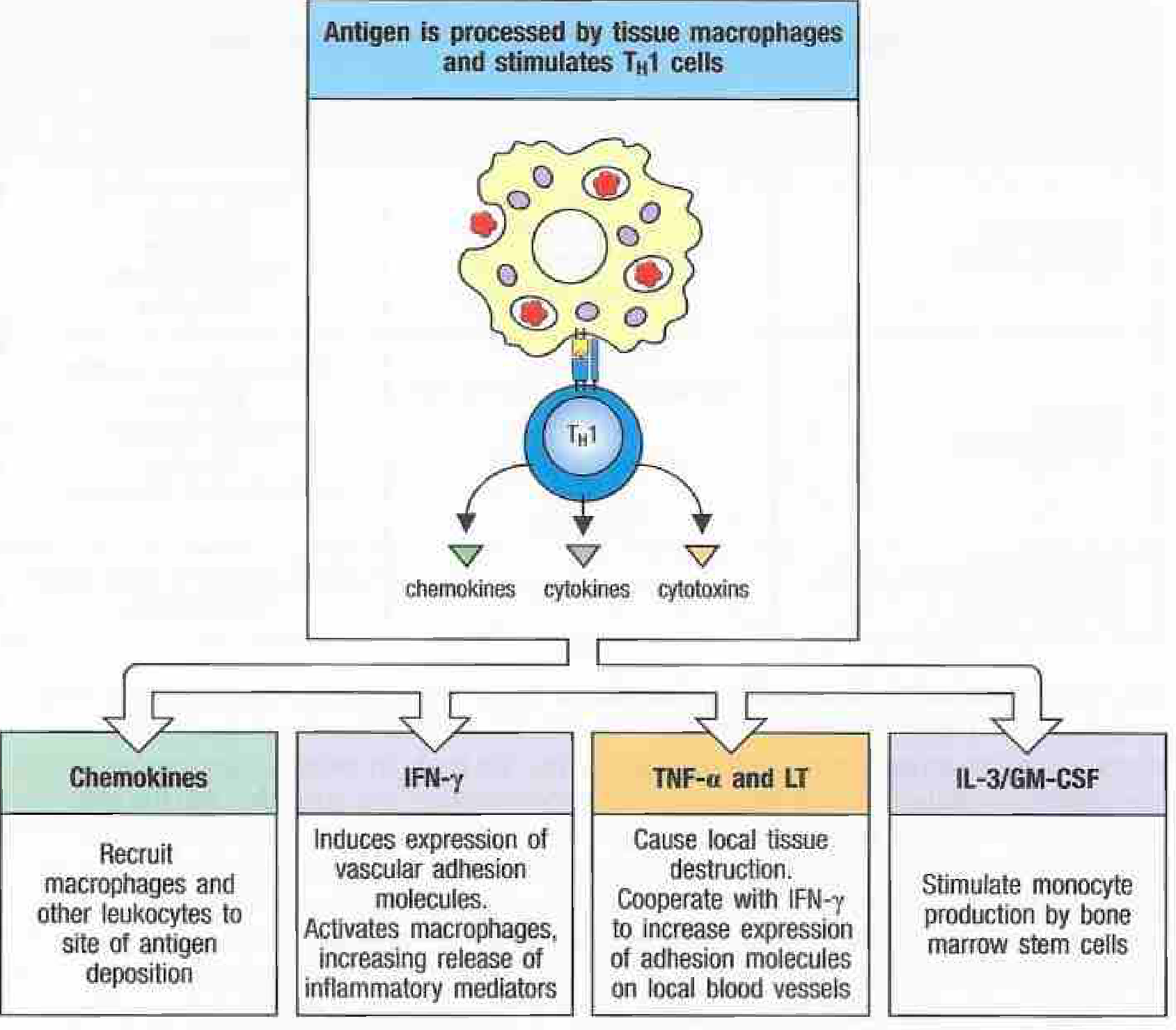
Antigen processed by tissue macrophages stimulates TH1 cells, which release chemokines (recruiting macrophages), IFN-γ (activating macrophages), TNF-α (causing local tissue destruction), and IL-3/GM-CSF (stimulating monocyte production). - Janeway's Immunobiology 10e
Step 2 - Elicitation of contact hypersensitivity - the 4-step process in skin:
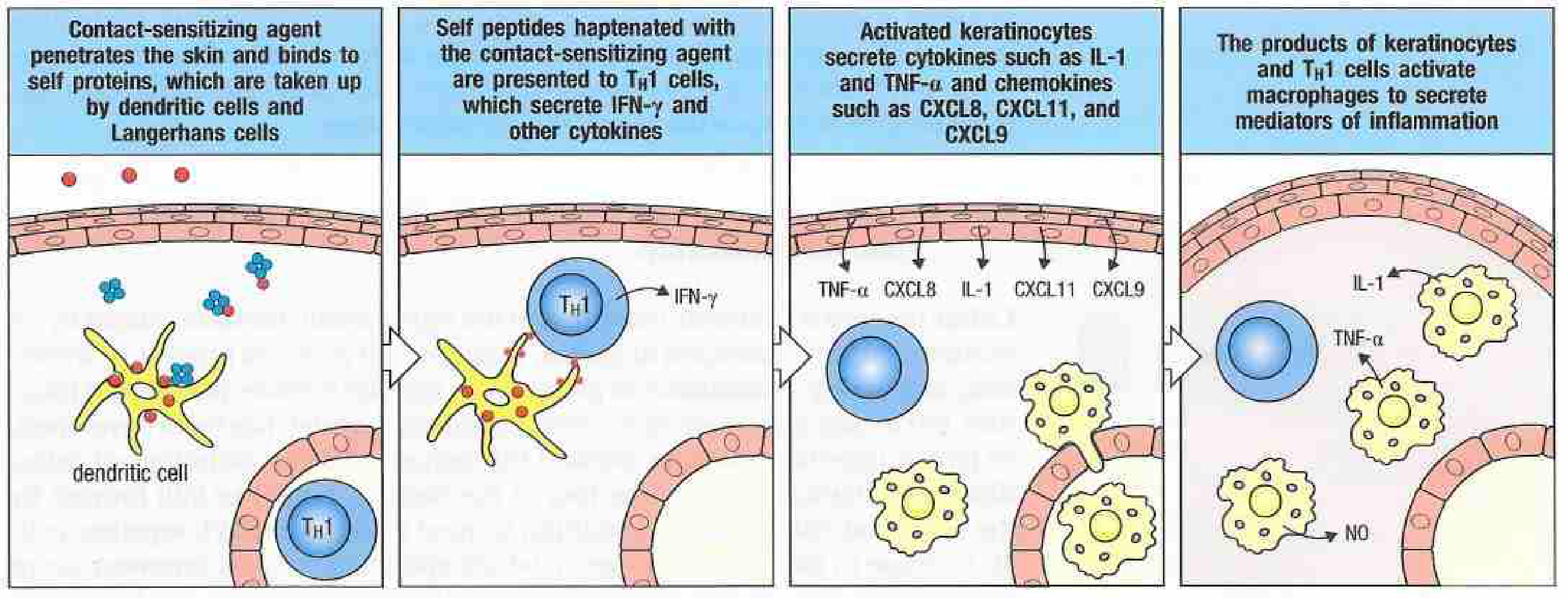
Elicitation of delayed-type hypersensitivity to a contact-sensitizing agent. (1) Metal ion penetrates skin, binds to self-protein as hapten, taken up by dendritic cells/Langerhans cells. (2) Haptenated peptides presented to TH1 cells → IFN-γ release. (3) Activated keratinocytes secrete TNF-α, IL-1, CXCL8, CXCL11, CXCL9. (4) Macrophages secrete IL-1, TNF-α, NO causing inflammation. - Janeway's Immunobiology 10e
Step 3 - Timeline of visible lesion formation (24-72 hours):
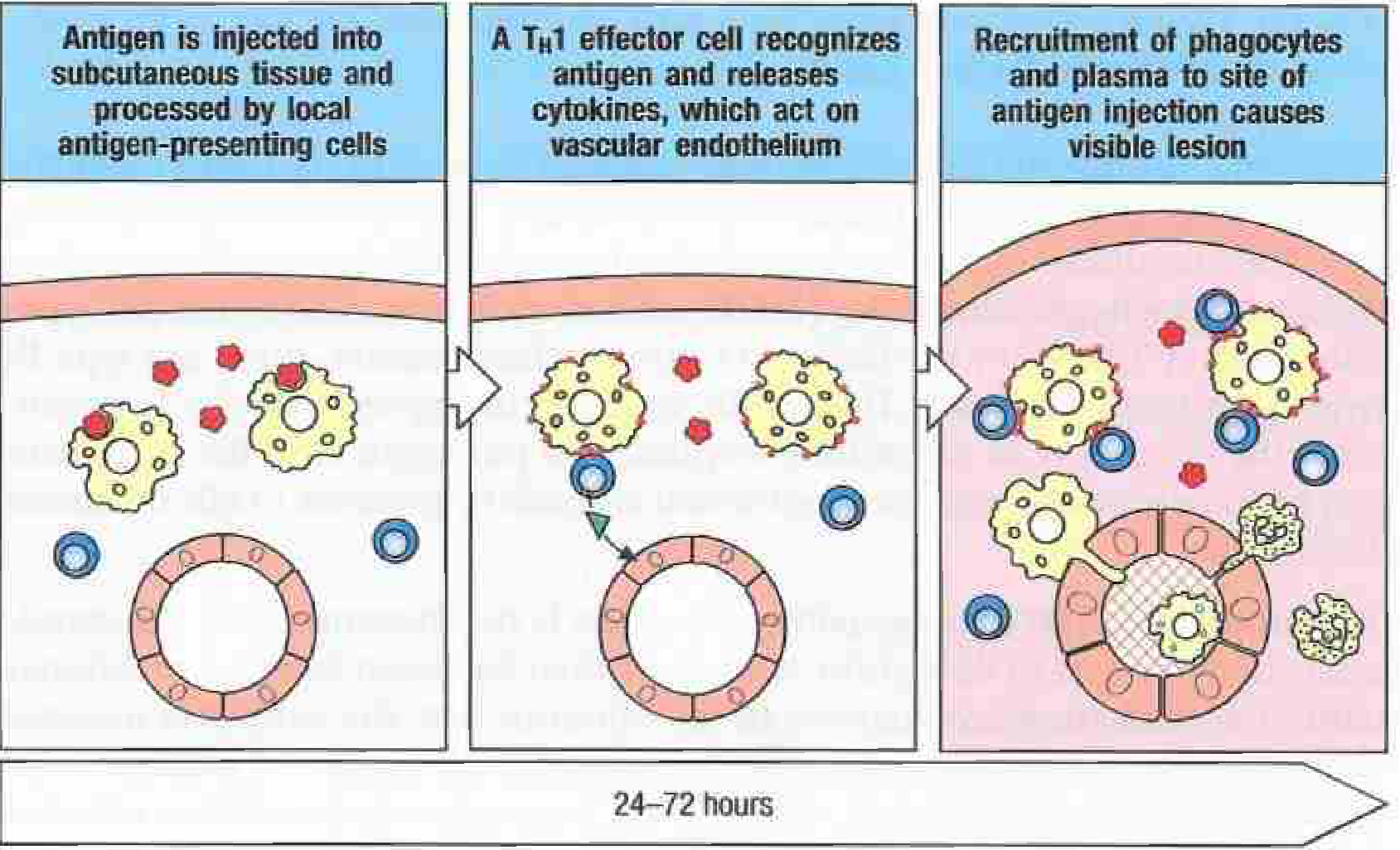
The visible DTH lesion takes 24-72 hours to develop: antigen injected → TH1 effector cell recognizes it and releases cytokines acting on vascular endothelium → recruitment of phagocytes and plasma to site causes the visible lesion. - Janeway's Immunobiology 10e
Metal Implant-Specific Mechanism
For implanted devices (prosthetic joints, stents, pacemakers), a unique mechanism operates:

Implant tribocorrosion releases metal wear particles → ingested by local macrophages, dendritic cells, osteoblasts, osteoclasts → metalloproteins form and transport metal ions systemically via the circulatory system to lymph nodes, liver, and spleen - triggering systemic sensitization. (Bone & Joint Research)
Signs and Symptoms
Cutaneous (Skin Contact - Most Common)
These appear 12-48 hours after contact (sometimes up to several days):
- Pruritus (itching) - the cardinal symptom, often the first complaint
- Erythema (redness) at the contact site
- Edema (swelling) of affected skin
- Vesicles - small fluid-filled blisters
- Eczematous dermatitis - weeping, crusting plaques
- Scaling and fissuring in chronic cases
- Lichenification - thickened, leathery skin with prolonged exposure
- Hyperpigmentation or hypopigmentation (post-inflammatory)
Characteristic distributions by metal source:
- Earlobes, neckline, wrist, periumbilical area - nickel from jewelry, belt buckles
- Hands - occupational chromium/nickel (cement workers, hairdressers)
- Neck - necklaces, perfume atomizers in sensitized patients ("atomizer sign")
- Oral mucosa - dental metal alloys (contact stomatitis)
Systemic Symptoms (Implant/Systemic Exposure)
When metal ions disseminate systemically (e.g., from failing implants or via ingestion):
- Joint pain, swelling, stiffness around prosthetic implants
- Effusions (excess fluid in joint)
- Impaired wound healing at surgical site
- Aseptic loosening of implant (bone resorption via osteoclast activation)
- Pseudotumor / Metallosis - solid or cystic masses near prosthesis (ALVAL: aseptic lymphocyte-dominated vasculitis-associated lesion)
- Systemic contact dermatitis - distant skin rash from systemically absorbed metal (e.g., from metal-on-metal hip)
- Generalized weakness and fatigue (rare, severe cases)
Metal-Specific Cutaneous Signs (from Dermatology 5e, Table 88.12):
| Metal | Specific Signs |
|---|---|
| Chromium (hexavalent) | Allergic & irritant contact dermatitis, ulceration ("chrome holes"), burns; systemic: renal failure, hepatic failure, anemia, coagulopathy |
| Nickel | Eczematous ACD at contact sites; oral stomatitis from dental fillings |
| Cobalt | ACD similar to nickel; found with nickel co-sensitization |
| Arsenic | Keratoses, hyperpigmentation, Mees' lines, Bowen's disease, skin cancer |
| Beryllium | Granulomatous dermatitis, lung granulomas |
| Thallium | Alopecia, acneiform papules, keratotic plaques, Mees' lines |
| Mercury | Allergic contact dermatitis, acrodynia (pink disease) |
| Gold | ACD, oral lichen planus from dental gold |
| Zinc chloride | Burns, oral lichen planus |
| Zirconium | Granulomas, blue-gray skin discoloration |
Causes and Risk Factors
Direct Causes
- Costume and cheap jewelry (earrings, rings, necklaces, belt buckles) - especially low-quality alloys high in nickel
- Occupational metal exposure - cement workers (chromium), hairdressers (nickel in dyes), metalworkers, welders, electronics workers
- Body piercing - early-age ear piercing dramatically increases nickel sensitization risk
- Orthopedic and dental implants - prosthetic hips/knees, cardiac stents, pacemaker leads, dental fillings
- Medical devices - IUDs (copper), orthodontic braces
Risk Factors
- Female sex - higher rates of nickel allergy linked to ear piercing practices
- Atopic history (asthma, atopic dermatitis, seasonal allergies)
- Previous sensitization - once sensitized, re-exposure causes reaction
- Occupation - construction, dentistry, hairdressing, manufacturing
- Genetic factors - polymorphisms in TNF, CLDN1, FLG genes increase susceptibility (as shown below)
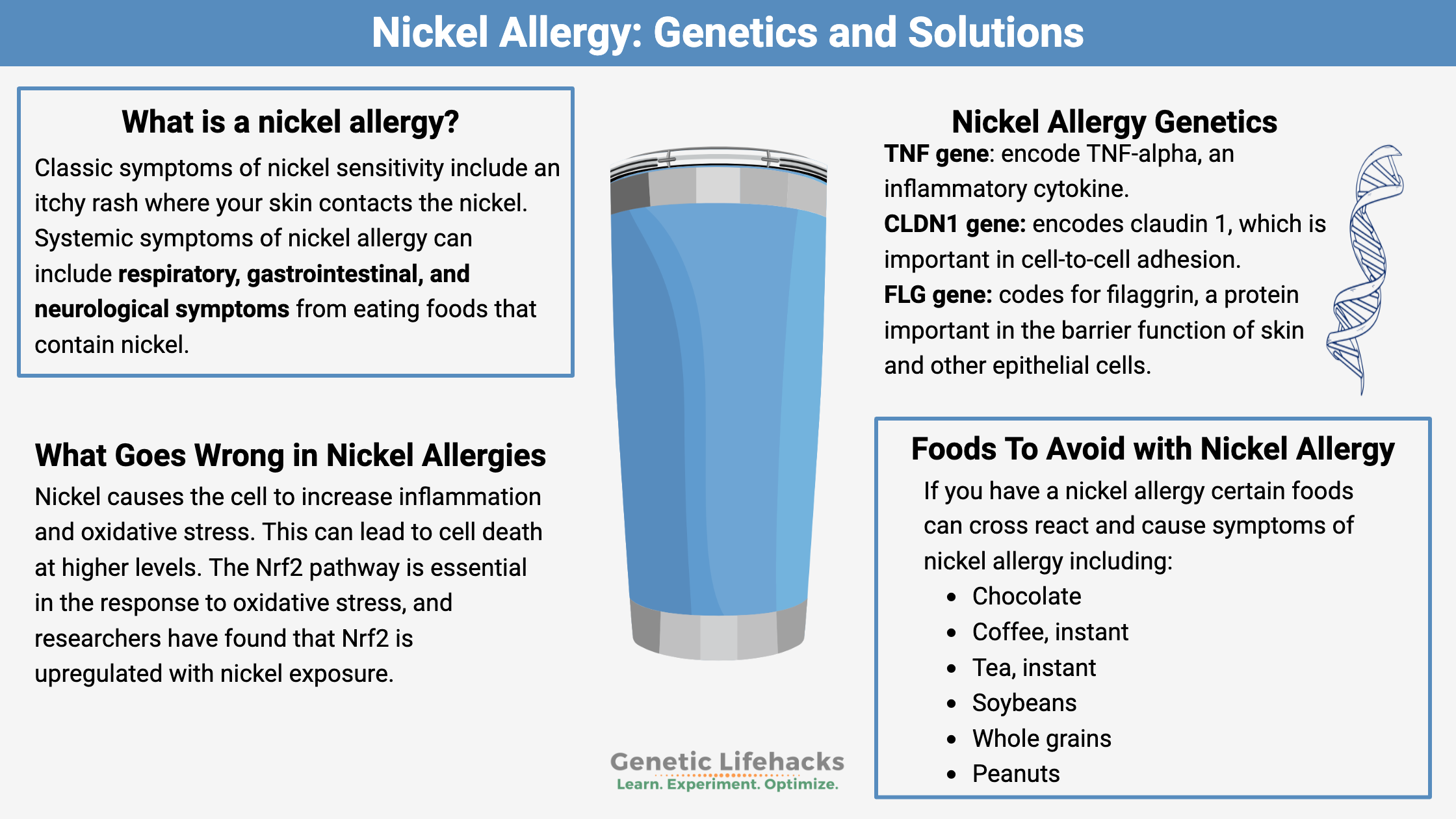
Genetic factors in nickel allergy: TNF gene encodes inflammatory TNF-α; CLDN1 encodes claudin-1 (cell-to-cell adhesion); FLG encodes filaggrin (skin barrier function). Nickel in foods can trigger systemic reactions in sensitized individuals.
Diagnosis
1. Clinical History
- Pattern and location of rash corresponding to metal contact sites
- Jewelry/piercing history, occupation, recent implant surgery
- Timing: delayed onset (12-72 hours after contact)
2. Epicutaneous Patch Testing (Gold Standard)
- Patch test panels (e.g., TRUE Test, North American Contact Dermatitis Group series) applied to the back for 48 hours, read at 48 and 72-96 hours
- Positive reaction = erythema + induration at the test site
- Identifies the specific metal(s) responsible
- Essential for patients with persistent/recurrent dermatitis
"Patch testing is the diagnostic test of choice to identify causal allergens and is indicated for patients with persistent or recurrent dermatitis in whom ACD is suspected." - Fitzpatrick's Dermatology, 5e
3. Spot Chemical Tests
- Dimethylglyoxime (DMG) test for nickel: detects nickel release from objects (pink precipitate = positive)
- 2-nitroso-1-naphthol-4-sulfonic acid spot test for cobalt
4. Blood Tests
- Lymphocyte transformation test (LTT) - useful for implant-related sensitivity
- Serum cobalt/chromium ion levels (for metal-on-metal implant assessment)
Prevention
Primary Prevention (Avoiding Sensitization)
- Avoid nickel-releasing jewelry - choose surgical steel, titanium, 14-karat gold, platinum, or sterling silver
- Legislation and regulation - the EU limits nickel release from skin-contact items to ≤0.5 μg/cm²/week (≤0.2 μg/cm²/week for piercing jewelry); similar policies should be adopted globally
- Delay ear piercing in children to reduce sensitization risk
- Pre-operative patch testing before joint replacement surgery if metal allergy is suspected - guides selection of hypoallergenic implant materials
- Occupational protection - wear protective gloves, barrier creams (e.g., zinc oxide), and protective clothing when handling metals; adequate ventilation for metal fumes
- Use nickel-free tools and equipment in sensitization-prone occupations
Secondary Prevention (Avoiding Elicitation Once Sensitized)
- Strict allergen avoidance - coat metal items with clear nail polish or protective tape
- Dietary nickel restriction in patients with systemic nickel allergy syndrome (avoid chocolate, coffee, instant tea, soybeans, whole grains, peanuts, legumes)
- Hypoallergenic implant selection - titanium, zirconia, or coated alloys for patients with known metal sensitivity
- Barrier emollients before occupational exposure
"To prevent development of nickel sensitivity, the European Union, in 1994, regulated the amount of nickel that may be released from objects with direct and prolonged skin contact to ≤0.5 μg nickel/cm²/week... Among Danish women, the prevalence of nickel allergy decreased from 28% in 1985 to 17% in 2007." - Fitzpatrick's Dermatology, 5e
Treatment
1. Allergen Avoidance (Mainstay)
The single most effective treatment. Complete avoidance of the offending metal allows the skin to heal and prevents recurrence.
"Allergen avoidance is the mainstay of ACD treatment. Educating patients about avoiding the allergen and related substances, and providing suitable alternatives, are crucial to a good outcome." - Fitzpatrick's Dermatology, 5e
2. Topical Corticosteroids
- First-line pharmacological treatment for mild-moderate ACD
- Potency selected based on body site (lower potency for face/flexures, higher for palms/soles)
- A 21-day course of topical corticosteroids at the cutaneous reaction site is effective in many implant-related cases
- Reduce inflammation, pruritus, and vesiculation
3. Systemic Corticosteroids
- For severe, widespread, or refractory ACD
- Oral prednisone (typically 0.5-1 mg/kg/day tapered over 2-3 weeks)
- Used when topical therapy is insufficient
4. Antihistamines
- Oral antihistamines for symptom relief, primarily for pruritus
- Note: antihistamines treat symptoms but do NOT address the underlying Type IV mechanism (unlike Type I allergy)
- Non-sedating antihistamines (cetirizine, loratadine) for daytime use
- Sedating antihistamines (hydroxyzine) for nighttime itch/sleep disruption
5. Calcineurin Inhibitors (Topical Immunomodulators)
- Tacrolimus ointment and pimecrolimus cream as steroid-sparing alternatives
- Particularly useful for facial/eyelid involvement or prolonged treatment to avoid steroid side effects
6. Emollients and Barrier Repair
- Moisturizers restore the skin barrier, reduce transepidermal water loss, and minimize allergen penetration
- Essential adjunct in all stages of ACD treatment
7. Wet Dressings / Compresses
- Cool, moist compresses for acute weeping vesicular reactions
- Reduce inflammation and provide symptomatic relief
8. Treatment for Implant-Related Reactions
- Topical/systemic corticosteroids as first step for peri-implant cutaneous reactions
- Implant removal if the implant has served its purpose and reaction is persistent
- Implant revision to non-allergenic materials (titanium alloy, ceramic, polytetrafluoroethylene-coated) - reserved for confirmed, refractory cases
- Revision surgery carries significant risks and unpredictable outcomes and is considered a last resort
9. Phototherapy
- Narrowband UVB or PUVA for chronic, widespread refractory cases
- Induces tolerance by promoting regulatory T cells
10. Systemic Immunosuppressants
- For severe chronic refractory ACD: azathioprine, methotrexate, cyclosporine, or mycophenolate mofetil
- Reserved for cases unresponsive to corticosteroids
Summary Table
| Feature | Details |
|---|---|
| Type | Type IV (delayed-type) hypersensitivity - cell mediated |
| Mechanism | Hapten + carrier protein → Th1/Tc1 sensitization → re-exposure → IFN-γ, TNF-α release → macrophage activation → inflammation |
| Onset | 12-72 hours after re-exposure; sensitization takes 10-25 days initially |
| Most common metal | Nickel (18-30% sensitization rate worldwide) |
| Key symptoms | Itching, erythema, vesicles, eczema at contact sites; joint pain/loosening for implants |
| Diagnosis | Patch testing (gold standard) |
| Mainstay treatment | Allergen avoidance |
| Medications | Topical/systemic corticosteroids, calcineurin inhibitors, antihistamines |
| Prevention | Nickel-free jewelry, regulatory limits on nickel release, pre-op patch testing, occupational protection |
Sources:
- Fitzpatrick's Dermatology, 5e - Chapters on Allergic Contact Dermatitis and Mucocutaneous Findings with Heavy Metals
- Janeway's Immunobiology, 10e - Chapter 14: Hypersensitivity Reactions (Type IV)
- Dermatology 2-Volume Set, 5e - Table 88.12: Mucocutaneous Findings Associated with Toxic Elements and Heavy Metals
- PMC: Hypersensitivity to Orthopedic Implants
This is a shared conversation. Sign in to Orris to start your own chat.