Function of parietal lobe and anatomy,brain stem syndrome with stroke localisation with how to differentiate between cortical stroke and dense hemiplegia
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the essential content to compose a comprehensive, well-structured answer.
Parietal Lobe: Anatomy, Functions, and Stroke Syndromes
PART 1: PARIETAL LOBE - ANATOMY
Gross Anatomy
The parietal lobe lies posterior to the central sulcus (Rolandic fissure), anterior to the parieto-occipital sulcus, and superior to the Sylvian fissure. It is divided into:
| Gyrus/Area | Brodmann Area | Function |
|---|---|---|
| Postcentral gyrus (primary somatosensory cortex) | 3, 1, 2 | Primary tactile and proprioceptive reception |
| Superior parietal lobule | 5, 7 | Somatosensory integration, spatial orientation |
| Inferior parietal lobule | 39, 40 | Higher integrative functions |
| Supramarginal gyrus | 40 | Phonological processing, ideomotor praxis |
| Angular gyrus | 39 | Reading, writing, calculation (dominant hemisphere) |
The postcentral gyrus is the primary sensory cortex - its somatotopic map mirrors the motor homunculus (hand and face areas are disproportionately large). Deeper parietal structures include the superior longitudinal fasciculus (connecting parietal to frontal and occipital lobes) and the arcuate fasciculus passing through the inferior parietal region.
Blood Supply
The parietal lobe is supplied predominantly by branches of the middle cerebral artery (MCA) - superior division supplies the postcentral and superior parietal cortex, while the inferior division branches supply the supramarginal and angular gyri. The superior sagittal region receives contributions from anterior cerebral artery (ACA) pericallosal branches.
PART 2: FUNCTIONS OF THE PARIETAL LOBE
A. Primary Somatosensory Functions (Postcentral Gyrus)
The parietal postcentral cortical defect is fundamentally one of sensory discrimination - the inability to integrate and localize stimuli. This results in:
- Astereognosis - inability to distinguish objects by size, shape, weight, and texture
- Agraphesthesia - failure to recognize figures written on the skin
- Impaired two-point discrimination
- Loss of tactile direction sense - inability to detect movement direction of a tactile stimulus
Primary perception (pain, touch, pressure, vibration, temperature) is relatively intact when the postcentral gyrus itself is spared; it is the discriminative component that fails.
B. Higher Cortical (Parietal Association) Functions
The parietal lobes encode a body schema (internal map of the body), a map of external topographic space, and are essential for calculation, left-right differentiation, and writing. Key functions and their lesion syndromes:
Dominant (Left) Parietal Lobe
| Syndrome | Deficit | Anatomical Basis |
|---|---|---|
| Gerstmann syndrome | Finger agnosia + acalculia + agraphia + left-right disorientation | Angular gyrus (BA 39) |
| Ideomotor apraxia | Cannot perform skilled movements on command despite intact motor and sensory function | Supramarginal gyrus (BA 40) |
| Conduction aphasia | Fluent speech with impaired repetition, paraphasic errors | Arcuate fasciculus / supramarginal gyrus |
| Tactile agnosia (astereognosis) | Cannot identify objects by touch | Postcentral gyrus |
| Alexia with/without agraphia | Reading/writing disturbance | Angular gyrus (BA 39) |
Non-dominant (Right) Parietal Lobe
| Syndrome | Deficit |
|---|---|
| Hemineglect (hemispatial neglect) | Ignores entire left hemispace - does not respond to stimuli from the left |
| Anosognosia | Unawareness or denial of own hemiplegia |
| Constructional apraxia | Cannot copy geometric figures or clock drawing |
| Dressing apraxia | Cannot dress correctly |
| Topographic disorientation | Gets lost in familiar places |
| Visuospatial deficits | Impaired depth perception, spatial relations |
Bilateral Parietal Lobe (Balint Syndrome - rare)
- Optic ataxia - reaching errors under visual guidance
- Oculomotor apraxia - inability to voluntarily move gaze
- Simultanagnosia - cannot perceive more than one object at a time
PART 3: BRAINSTEM SYNDROMES AND STROKE LOCALIZATION
Key Anatomical Principle: The "Crossed Sign"
The most important localizing clue for brainstem stroke is the crossed neurological sign: ipsilateral cranial nerve deficit + contralateral hemiplegia/hemisensory loss. This occurs because cranial nerve nuclei are at the level of the lesion (ipsilateral) while long tracts (corticospinal, spinothalamic) that have not yet crossed are also affected at that level.
Features strongly suggestive of brainstem involvement vs. hemispheric stroke:
- Crossed signs (one-sided face deficit + opposite body deficit)
- Bilateral motor or sensory signs
- Prominent cranial nerve abnormalities (diplopia, dysarthria, dysphagia, facial palsy)
- Cerebellar ataxia combined with hemiparesis
- Vertigo + vomiting as prominent features
Brainstem Blood Supply
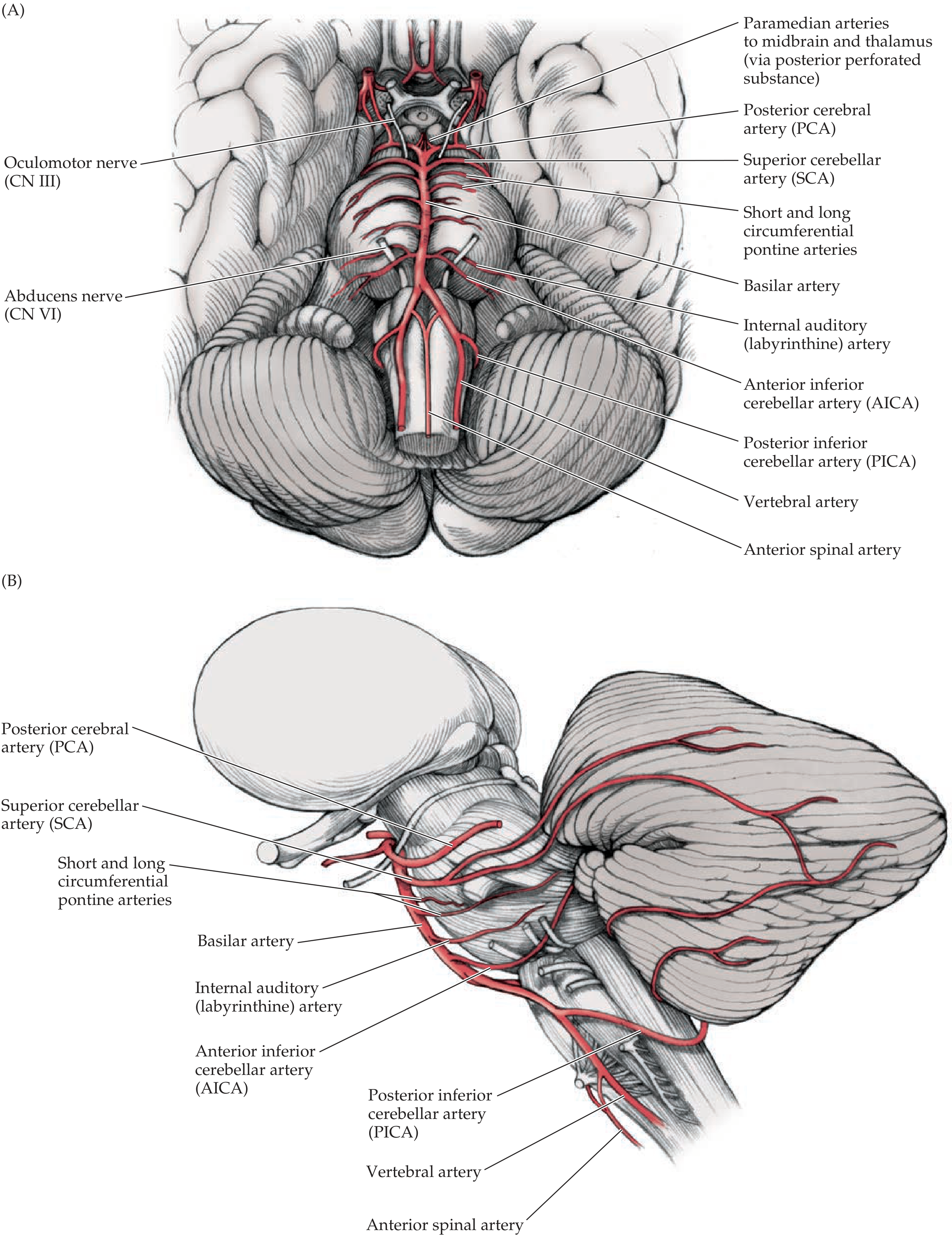
The vertebrobasilar system gives rise to:
- Paramedian branches - supply medial brainstem (corticospinal tract, MLF, cranial nerve nuclei)
- Short circumferential branches - supply lateral brainstem tegmentum
- Long circumferential branches (PICA, AICA, SCA) - supply dorsolateral brainstem + cerebellum
A. MEDULLARY SYNDROMES
| Feature | Medial Medullary Syndrome | Lateral Medullary Syndrome (Wallenberg) |
|---|---|---|
| Artery | Anterior spinal artery / vertebral branches | PICA or vertebral artery |
| Ipsilateral | Tongue weakness (CN XII) | Facial pain & temperature loss (CN V); Horner syndrome; dysarthria, dysphagia (IX, X); limb ataxia |
| Contralateral | Hemiplegia (arm + leg; face spared) + loss of vibration/proprioception | Body pain & temperature loss (spinothalamic) |
| Key feature | Face is SPARED (corticobulbar fibers have already decussated above) | No hemiplegia - classic "pure sensory crossed syndrome" |
Wallenberg (Lateral Medullary) Syndrome - mnemonic "PICA":
- Palate palsy + dysphagia
- Ipsilateral face (pain/temp loss), Ipsilateral Horner
- Contralateral body pain/temp loss
- Ataxia (ipsilateral cerebellar)
B. PONTINE SYNDROMES
| Syndrome | Artery | Ipsilateral Signs | Contralateral Signs |
|---|---|---|---|
| Medial pontine (Millard-Gubler) | Paramedian basilar branches | CN VI palsy (lateral rectus) + CN VII palsy (LMN facial) | Hemiplegia (arm, leg, face) |
| Foville syndrome | Paramedian branches (ventral + dorsal) | Horizontal gaze palsy toward lesion + facial palsy | Hemiplegia |
| AICA syndrome (lateral caudal pons) | AICA | Facial pain/temp loss (CN V), ataxia, INO (MLF), Horner, hearing loss, vertigo | Body pain/temp loss (spinothalamic) |
| SCA syndrome (dorsolateral rostral pons) | SCA | Cerebellar ataxia | Variable lateral tegmental features |
| Pure motor hemiparesis / Dysarthria-clumsy hand | Paramedian (lacunar) | - | Contralateral face + arm + leg weakness; dysarthria |
Signs of pontine dysfunction to recognize:
- Bilateral Babinski signs
- Bilateral small but reactive pupils (disruption of descending sympathetic fibers)
- Ocular bobbing (eyes dip rapidly downward then slowly return)
- Perioral + "salt-and-pepper" facial tingling
- Horizontal gaze palsy or abducens palsy
C. MIDBRAIN SYNDROMES
| Syndrome | Artery | Ipsilateral Signs | Contralateral Signs |
|---|---|---|---|
| Weber syndrome (medial midbrain - cerebral peduncle) | PCA / paramedian branches | CN III palsy (ptosis, mydriasis, "down-and-out" eye) | Hemiplegia (arm, leg, face) |
| Claude syndrome (midbrain tegmentum) | PCA | CN III palsy | Contralateral ataxia and tremor (red nucleus) |
| Benedikt syndrome (combined) | PCA | CN III palsy | Contralateral hemitremor + hemiplegia |
| Parinaud syndrome (dorsal midbrain) | Top of basilar / PCA | Upgaze palsy, convergence-retraction nystagmus, light-near dissociation | No hemiplegia (tectum only) |
Signs of midbrain dysfunction:
- CN III palsy with fixed dilated pupil
- Decerebrate (extensor) posturing
- Impaired consciousness (ARAS involvement)
PART 4: CORTICAL STROKE vs. DENSE HEMIPLEGIA - How to Differentiate
This is one of the most clinically important distinctions. The key question: is the hemiplegia from a cortical (MCA territory) infarct or from a subcortical/capsular infarct (internal capsule - "dense/pure motor hemiplegia")?
Mechanism
| Feature | Cortical Stroke | Dense (Pure Motor) Hemiplegia - Capsular/Lacunar |
|---|---|---|
| Lesion location | MCA cortex (frontal + parietal cortex) | Internal capsule (posterior limb), basis pontis, corona radiata |
| Pathology | Usually large artery thromboembolism | Small vessel disease (lacunar); less often small cardioembolic |
| Artery | Middle cerebral artery (MCA) - superior or inferior division | Lenticulostriate arteries (branches of MCA) |
Clinical Features - The Differentiating Signs
| Feature | Cortical MCA Stroke | Dense (Capsular) Hemiplegia |
|---|---|---|
| Motor deficit | Hemiplegia often PARTIAL - face and arm > leg (superior division); or arm = leg | COMPLETE and equal face + arm + leg weakness ("dense" pure motor) |
| Sensory loss | Cortical-type (astereognosis, agraphesthesia, 2-point discrimination loss) | May be absent (pure motor lacune) or proportional loss of all modalities |
| Aphasia | Present if dominant hemisphere (Broca's or Wernicke's depending on division) | ABSENT (subcortical; Broca and Wernicke areas are cortical) |
| Neglect/hemineglect | Present with right hemisphere (non-dominant) cortical lesion | ABSENT |
| Gaze deviation | Eyes deviate TOWARD the side of lesion ("frontal eye field" destruction) | May also occur but less marked |
| Visual field defect | Homonymous hemianopia common (optic radiation involvement) | ABSENT in pure capsular lacune |
| Apraxia | Present (dominant parietal) | ABSENT |
| Anosognosia | Present (non-dominant parietal) | ABSENT |
| Cortical sensory signs | Astereognosis, extinction, agraphesthesia | ABSENT |
| Level of consciousness | Often reduced initially (large cortical infarcts) | Usually PRESERVED (small lacune) |
| Convulsions | More common (cortical irritation) | Rare |
The "Cortical Signs" - Key Positive Findings for Cortical Stroke
If any of the following are present alongside hemiplegia, the lesion is cortical not capsular:
- Aphasia (expressive/receptive) - localizes to dominant hemisphere cortex
- Hemispatial neglect - right parietal cortex
- Anosognosia - non-dominant parietal
- Visual field defect (hemianopia) - optic radiation in parieto-occipital region
- Gaze preference toward the side of the lesion
- Cortical sensory loss - astereognosis, agraphesthesia, extinction to double simultaneous stimulation
- Apraxia
- Seizures at onset
Arm vs. Leg Ratio
This is a simple bedside clue:
- Arm >> Leg weakness = MCA (superior division) cortical stroke (face-arm homunculus on lateral cortex)
- Leg >> Arm weakness = ACA territory (parasagittal cortex - leg representation is medial)
- Face + Arm + Leg EQUAL and dense = Internal capsule (all fibers tightly packed in posterior limb) or basis pontis
Summary Comparison Table
| Clinical Sign | Cortical Stroke | Capsular/Brainstem | Brainstem |
|---|---|---|---|
| Hemiplegia | Yes (often partial, arm > leg) | Yes (complete, equal) | Yes + CN sign |
| Aphasia | Yes (dominant) | No | No |
| Neglect | Yes (non-dominant) | No | No |
| Cortical sensory loss | Yes | No | No |
| Hemianopia | Yes | No (usually) | Variable |
| Crossed signs (CN + body) | No | No | YES - pathognomonic |
| Consciousness impaired | Possibly (large stroke) | No (small lacune) | Yes (if pontomesencephalic) |
| Cerebellar signs | No | No | Yes (posterior fossa) |
Sources:
- Adams and Victor's Principles of Neurology, 12th Edition - "Clinical Effects of Parietal Lobe Lesions," "Cortical Sensory Syndromes," "Parietal Lobe Disorders"
- Neuroanatomy through Clinical Cases, 3rd Edition - "Brainstem Vascular Supply," "Vertebrobasilar Vascular Disease," "Focal Vascular Syndromes of the Pons and Medulla" (Tables 14.7, 14.8, 14.9)
- Harrison's Principles of Internal Medicine, 22E (2025) - "Signs and Symptoms: Structures Involved"
Blood supply of brain stem simplified
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a clear, simplified breakdown of brainstem blood supply, using the textbook diagrams directly.
Blood Supply of the Brainstem - Simplified
The One Golden Rule
Everything in the brainstem comes from the vertebrobasilar system. There is no anterior circulation contribution.
Step 1: The Main Vessels (Top-Down Logic)
Think of it as a Y-shape flipped upside down:
Two VERTEBRAL arteries (from subclavian, via foramen transversaria C6-C2)
|
↓ (join at pontomedullary junction)
BASILAR artery (runs along ventral pons)
|
↓ (splits at pontomesencephalic junction)
Two POSTERIOR CEREBRAL arteries (PCA)
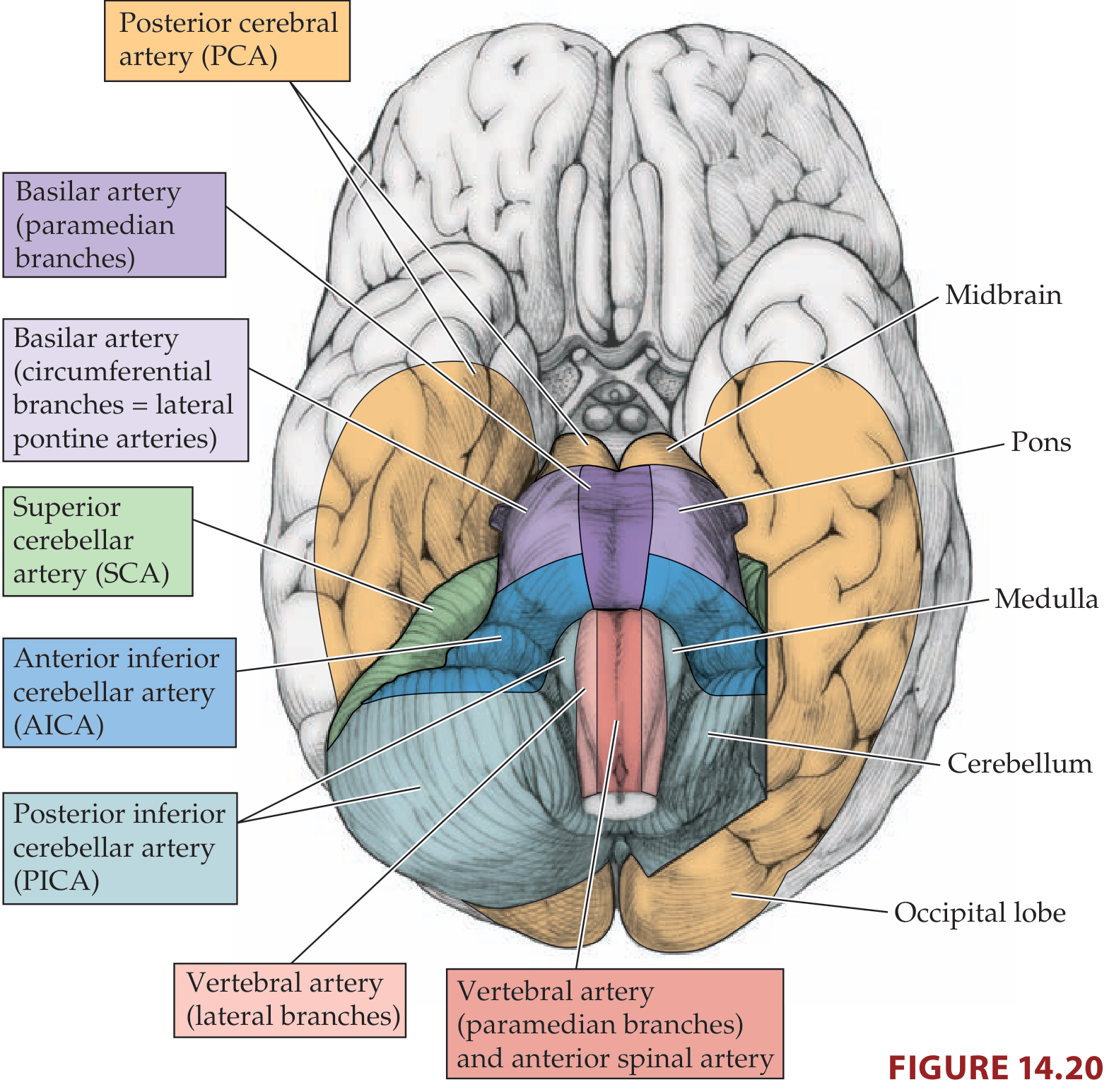
Step 2: The Three Major Branches (One Per Cerebellar Level)
Just as there are 3 cerebral arteries (ACA, MCA, PCA), there are 3 cerebellar arteries, each arising at a different level:
| Artery | Arises From | Level | What It Supplies |
|---|---|---|---|
| PICA (Posterior Inferior Cerebellar A.) | Vertebral artery | Medulla | Lateral medulla + inferior cerebellum |
| AICA (Anterior Inferior Cerebellar A.) | Proximal basilar | Caudal pons | Lateral caudal pons + small cerebellar area + inner ear (labyrinthine a.) |
| SCA (Superior Cerebellar A.) | Top of basilar | Rostral pons / midbrain junction | Superior cerebellum + small dorsolateral rostral pons |
Memory trick: Bottom to top = PICA → AICA → SCA (ascending the brainstem)
Step 3: The Internal Branching Pattern - Medial vs. Lateral
Every level of the brainstem follows the same internal pattern - a medial zone and a lateral zone with different blood supplies:
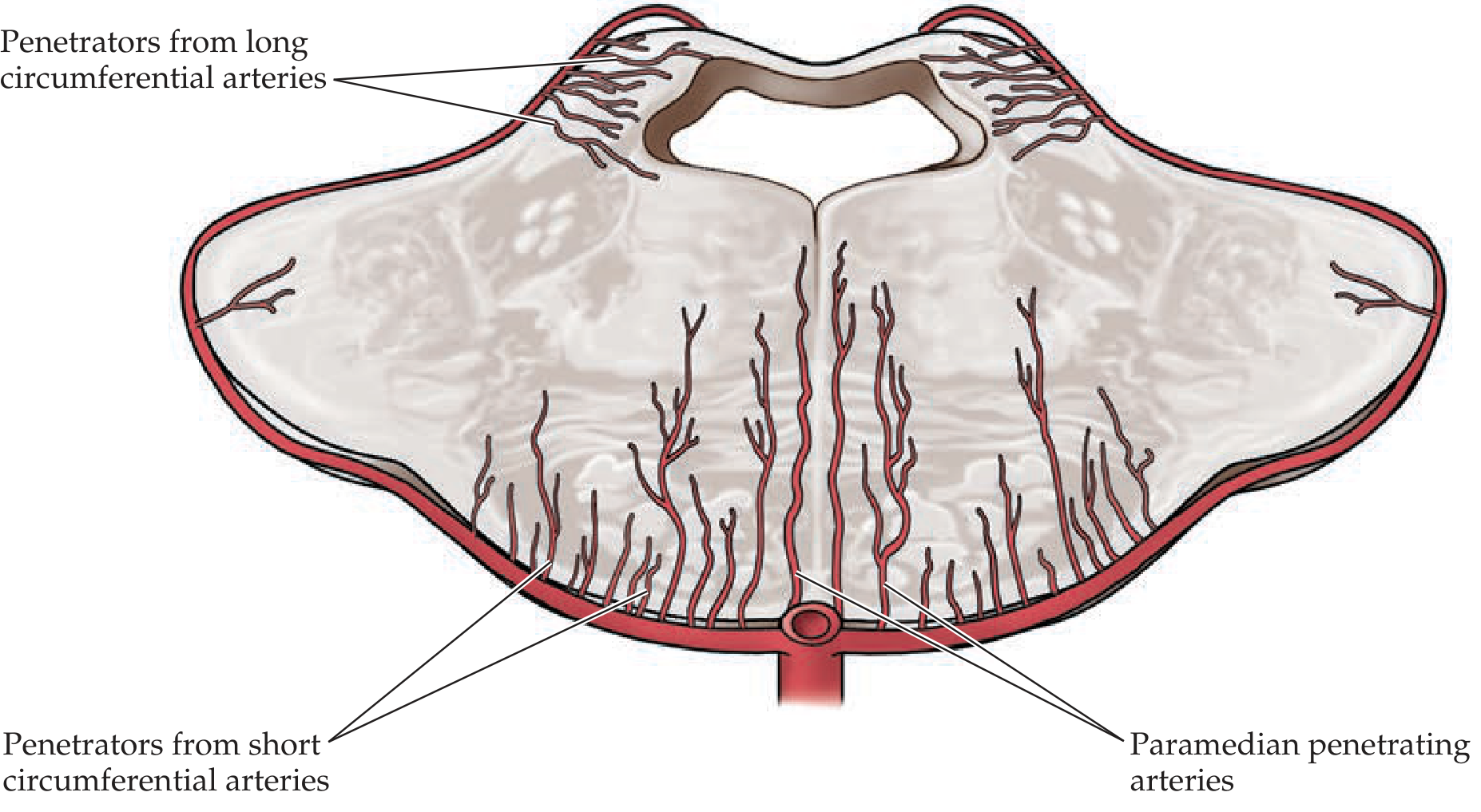
| Zone | Branch Type | Arises From | What it Supplies |
|---|---|---|---|
| Medial / Paramedian | Paramedian penetrating arteries | Basilar / vertebral / anterior spinal | Corticospinal tract, MLF, CN nuclei near midline |
| Lateral / Dorsolateral | Short + long circumferential arteries, PICA/AICA/SCA | Basilar / vertebral | Spinothalamic tract, CN V nucleus, sympathetics, cerebellar peduncles |
This is why medial syndromes affect the corticospinal tract (hemiplegia), and lateral syndromes affect sensory crossing tracts and cranial nerves - they have separate blood supplies.
Step 4: Level-by-Level Summary
MEDULLA
| Region | Artery | Key structures inside |
|---|---|---|
| Medial medulla | Anterior spinal artery (caudal) + vertebral paramedian branches (rostral) | Pyramid (corticospinal tract), CN XII nucleus, medial lemniscus |
| Lateral medulla | Vertebral + PICA branches | CN IX/X nuclei, CN V spinal nucleus, spinothalamic tract, sympathetic fibers, inferior cerebellar peduncle |
PONS
| Region | Artery | Key structures inside |
|---|---|---|
| Medial pons | Paramedian branches of basilar | Corticospinal + corticobulbar tracts, CN VI nucleus, MLF, PPRF |
| Lateral caudal pons | AICA | CN VII fascicles, CN V nucleus, spinothalamic tract, medial lemniscus, vestibular nuclei, middle cerebellar peduncle |
| Lateral rostral pons | Circumferential branches of basilar (lateral pontine arteries) | Same lateral tegmental structures |
MIDBRAIN
| Region | Artery | Key structures inside |
|---|---|---|
| Medial midbrain (cerebral peduncle) | Paramedian branches from top of basilar + proximal PCA | Corticospinal tract, CN III fascicles |
| Lateral/dorsal midbrain | PCA branches | Red nucleus, substantia nigra, CN III nucleus, superior colliculus |
| Thalamus (closely related) | Perforators from top of basilar + proximal PCA | Thalamic nuclei - Artery of Percheron supplies bilateral medial thalamus - occlusion = bilateral infarcts + coma |
Quick Reference - Artery to Clinical Syndrome
| Artery Occluded | Syndrome | Cardinal Signs |
|---|---|---|
| PICA / Vertebral | Lateral Medullary (Wallenberg) | Ipsilateral face pain/temp loss + Horner + dysphagia + ataxia; Contralateral body pain/temp loss; NO hemiplegia |
| Anterior spinal / Vertebral paramedian | Medial Medullary | Contralateral hemiplegia (arm+leg, face spared) + ipsilateral tongue weakness (CN XII) + contralateral vibration/proprioception loss |
| AICA | Lateral Caudal Pontine | Ipsilateral: CN VII palsy, facial sensory loss, Horner, INO, hearing loss, ataxia; Contralateral body pain/temp loss |
| Basilar paramedian (pons) | Medial Pontine (Millard-Gubler) | Ipsilateral CN VI + VII palsy; Contralateral hemiplegia |
| Basilar paramedian (midbrain) | Weber syndrome | Ipsilateral CN III palsy; Contralateral hemiplegia |
| Top of basilar / PCA | "Top of basilar" syndrome | Bilateral cortical blindness, memory loss, CN III palsy, coma; may also cause bilateral thalamic infarcts |
| Artery of Percheron | Bilateral thalamic infarct | Sudden coma + vertical gaze palsy, amnesia - unique to this artery |
The Single Most Useful Bedside Rule
Crossed sign = brainstem lesion - ipsilateral cranial nerve deficit + contralateral hemiplegia/hemisensory loss. This pattern is impossible with a cortical stroke and immediately places the lesion in the brainstem.
Sources: Neuroanatomy through Clinical Cases, 3rd Edition (Blumenfeld); Gray's Anatomy for Students - "Vascular Supply to the Brainstem"
This is a shared conversation. Sign in to Orris to start your own chat.