Applied Physiology of compliance
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have excellent material and diagrams to write a comprehensive, well-organized answer. Here it is:
Applied Physiology of Compliance
1. Definition and Formula
Compliance is the change in volume produced per unit change in pressure:
C = ΔV / ΔP
It is the inverse of elastance (stiffness). A highly compliant lung inflates easily (like a thin rubber band); a stiff, low-compliance lung requires much more pressure per unit volume change.
Normal values:
- Lung compliance alone: ~200 mL/cm H₂O
- Chest wall compliance alone: ~200 mL/cm H₂O
- Total respiratory system (lungs + chest wall in series): ~110 mL/cm H₂O
Because the lung and chest wall are in series, their compliances combine as reciprocals:
1/C_RS = 1/C_L + 1/C_W
Equivalently: Elastance_RS = Elastance_L + Elastance_W
(Murray & Nadel's Textbook of Respiratory Medicine; Costanzo Physiology 7th Ed., p. 208)
2. Elastic Forces Determining Compliance
Two distinct forces generate elastic recoil in the lung:
(a) Tissue Elastic Forces (~1/3 of total)
Elastin and collagen fibers within the lung parenchyma are kinked and contracted at low volumes. As the lung expands, they stretch and exert increasing recoil. A saline-filled lung (which eliminates the air-fluid interface) demonstrates these tissue forces alone - its compliance is ~3x higher than the same air-filled lung.
(b) Surface Tension Forces (~2/3 of total)
The air-fluid interface lining each alveolus creates an inward collapsing force. Using the Law of Laplace:
P = 2T / r
where P = collapsing pressure, T = surface tension, r = alveolar radius.
In a normal alveolus (radius ~100 µm) with surfactant, this generates ~4 cm H₂O. Without surfactant (pure water T = 72 dynes/cm), this rises to ~18 cm H₂O - demonstrating why surfactant is so important.
(Guyton & Hall Medical Physiology, p. 494-495)
3. The Pressure-Volume (Compliance) Curve and Hysteresis
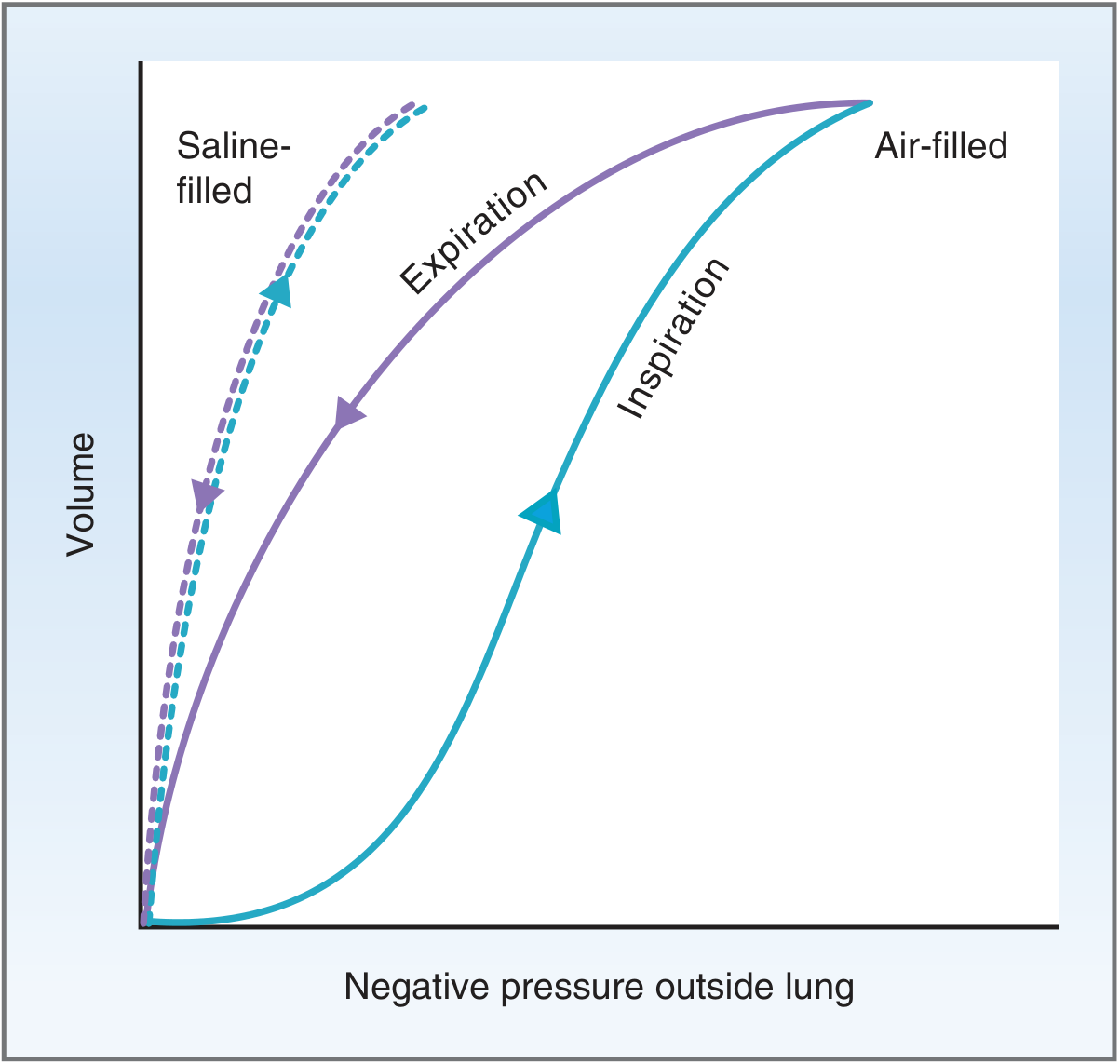
Hysteresis means the inspiration and expiration limbs of the pressure-volume loop are different. This occurs because of surface tension dynamics with surfactant:
- Inspiration limb: At low lung volumes, surfactant molecules are tightly packed. As inflation begins, new surfactant from type II cells enters but initially cannot match the increasing surface area - so surfactant density is low, surface tension is high, compliance is low, and the curve is initially flat. As inflation proceeds, surfactant density catches up and compliance increases.
- Expiration limb: Begins at high volume where intermolecular forces between fluid molecules are low. Surface area decreases faster than surfactant can be removed, so surfactant density stays high, surface tension stays low, and compliance is relatively higher than on the inspiration limb.
- Compliance is typically measured on the expiration limb because the inspiration limb is flattened at maximal volumes.
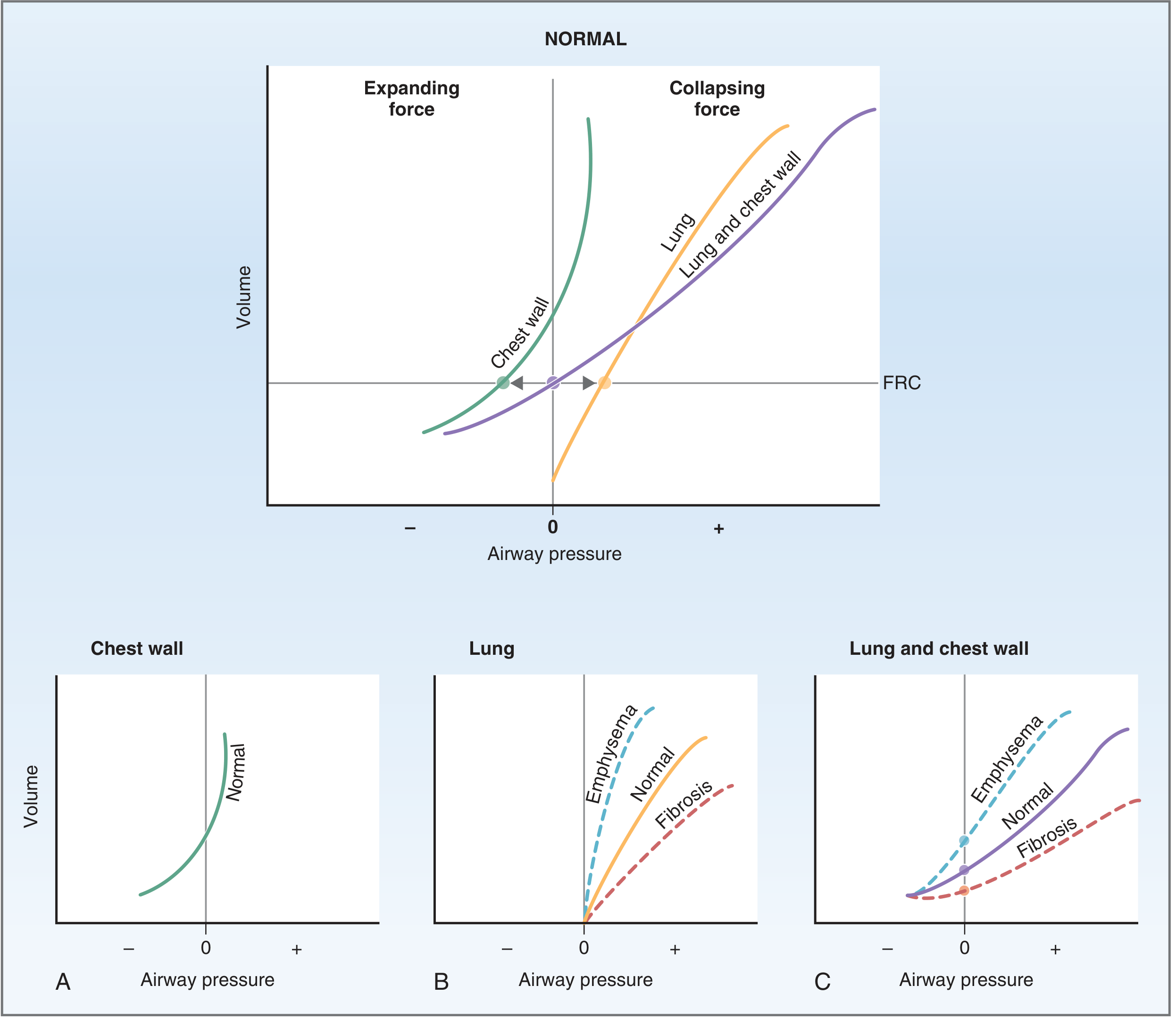
4. Lung and Chest Wall Interaction - FRC
The lung "wants" to collapse; the chest wall "wants" to spring outward. These opposing elastic forces pull on the intrapleural space, creating a negative intrapleural pressure (normally -5 cm H₂O at rest). This negative pressure prevents both lung collapse and chest wall from springing out.
FRC is the equilibrium point where the collapsing force of the lungs exactly equals the expanding force of the chest wall - no net force, airway pressure = atmospheric. This is the resting end-expiratory volume.
- At volumes below FRC: Chest wall recoil exceeds lung recoil → combined system "wants" to expand (airway pressure negative)
- At volumes above FRC: Lung recoil exceeds chest wall recoil → combined system "wants" to collapse (airway pressure positive)
- At very high volumes, both the lung and chest wall "want" to collapse
(Costanzo Physiology 7th Ed., p. 207)
5. Role of Surfactant
Surfactant is a complex phospholipid (predominantly dipalmitoyl phosphatidylcholine, DPPC) secreted by type II alveolar cells, which make up ~10% of the alveolar surface.
Key functions:
- Reduces surface tension from 50 dynes/cm (without surfactant) to 5-30 dynes/cm (normal range) - a 12 to 10-fold reduction
- Increases lung compliance, reducing work of breathing
- Stabilizes alveoli of different sizes: Without surfactant, by Laplace's law, smaller alveoli would have higher collapsing pressure and empty into larger ones. Surfactant preferentially reduces surface tension more in smaller alveoli (surfactant molecules pack more densely as radius decreases), equalizing pressure across alveolar sizes.
Absence of surfactant (e.g., Respiratory Distress Syndrome of the Newborn in premature infants born before 28-32 weeks, before surfactant secretion begins): lung compliance falls dramatically, alveoli collapse (atelectasis), ventilation-perfusion mismatch → hypoxemia. Treatment: exogenous surfactant + CPAP/mechanical ventilation.
(Guyton & Hall, p. 495)
6. Disease States and Compliance
| Condition | Compliance | Mechanism | Effect on FRC | Clinical Features |
|---|---|---|---|---|
| Emphysema | ↑ Increased | Destruction of elastic fibers | ↑ Higher FRC | Barrel chest, pursed-lip breathing, air trapping |
| Pulmonary fibrosis | ↓ Decreased | Stiffening/scarring of lung tissue | ↓ Lower FRC | Increased work of breathing, restrictive pattern |
| Pulmonary edema | ↓ Decreased | Alveolar fluid, surfactant washout | ↓ Lower FRC | Hypoxemia, increased respiratory effort |
| ARDS | ↓ Decreased | Inflammatory exudate, surfactant loss, collapse | ↓ Lower FRC | Severe hypoxemia, requires PEEP |
| Obesity / supine position | ↓ Decreased | Abdominal contents pushing diaphragm up | ↓ Lower FRC | Increased work of breathing under anesthesia |
Emphysema in detail:
Loss of elastic fibers → compliance increases (steeper P-V slope). At the original FRC, the lung's collapsing force is now less than the chest wall's expanding force. To rebalance, volume is added until lung recoil again equals chest wall recoil - the new FRC is higher. Patients breathe at elevated lung volumes → barrel chest.
Fibrosis in detail:
Scar tissue stiffens the lung → compliance decreases (flatter P-V slope). The lung's collapsing force at the original FRC now exceeds the chest wall's expanding force. Volume is expelled until a new balance point is found at a lower FRC. Patients must generate greater inspiratory effort for the same tidal volume.
7. Clinical Applications
PEEP and Compliance
Patients with low lung compliance (e.g., ARDS, pulmonary fibrosis) may receive PEEP during mechanical ventilation to prevent alveolar derecruitment at end-expiration. PEEP increases end-expiratory volume toward (or above) the normal FRC, keeping alveoli open and improving oxygenation. However, not all PEEP is transmitted to the pleural space - the fraction transmitted depends on the ratio of chest wall elastance to total respiratory system elastance:
ΔPpl = PEEP × (Ew / ERS)
If lung compliance is very low (high EL) but chest wall compliance is normal (Ew), a smaller fraction of PEEP reaches the pleura, limiting hemodynamic impact.
Work of Breathing
Inspiratory work has three components:
- Compliance work (elastic work): overcoming elastic recoil of lungs and chest wall - predominant in low-compliance states
- Tissue resistance work: overcoming viscosity of lung/chest tissue
- Airway resistance work: overcoming resistance to airflow
In normal quiet breathing, the respiratory muscles use only 3-5% of total body energy expenditure. In low-compliance states (ARDS, fibrosis), compliance work increases dramatically. At high exercise intensity, respiratory work can increase 50-fold, becoming a limiting factor in exercise tolerance.
Time Constant
The time constant (τ) = R × C (resistance × compliance). It governs how quickly a lung unit fills or empties. In non-uniform compliance (e.g., heterogeneous ARDS), lung units with different time constants fill at different rates - a phenomenon important in selecting appropriate respiratory rate and I:E ratio during mechanical ventilation. Fast rates prevent adequate emptying of slow units (gas trapping) and may overdistend fast units.
Combined Lung-Thorax Compliance
In the intact thorax:
C_combined ≈ 110 mL/cm H₂O (roughly half C_lung alone)
This is because the rigid chest wall adds its own elastic load in series. At the extremes of volume (near TLC or RV), chest wall stiffness increases dramatically and combined compliance may fall to <20% of lung compliance alone.
8. Summary Table
| Parameter | Value | Notes |
|---|---|---|
| Lung compliance alone | 200 mL/cm H₂O | Measured in isolated or paralyzed subject |
| Chest wall compliance | 200 mL/cm H₂O | Measured separately |
| Combined (respiratory system) | ~110 mL/cm H₂O | Series combination |
| Alveolar surface tension (with surfactant) | 5-30 dynes/cm | Varies with lung volume |
| Alveolar surface tension (without surfactant) | ~50 dynes/cm | As in RDS |
| Normal intrapleural pressure at FRC | -5 cm H₂O | Created by opposing elastic forces |
| Respiratory energy at rest | 3-5% of total | Rises dramatically in stiff lungs |
Sources:
- Costanzo Physiology, 7th Ed., pp. 204-212 (Compliance of Lungs, Chest Wall, Diseases of Compliance, Surface Tension)
- Guyton and Hall Textbook of Medical Physiology, pp. 493-496 (Compliance, Surfactant, Surface Tension, Work of Breathing)
- Murray & Nadel's Textbook of Respiratory Medicine (Total Respiratory Compliance, PEEP and Pleural Pressure)
Inflammation of lungs after birth in short
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have enough for a concise, focused answer covering both neonatal pneumonia and BPD (the two main forms of lung inflammation after birth).
Lung Inflammation After Birth (Neonatal)
The two main conditions are Neonatal Pneumonia and Bronchopulmonary Dysplasia (BPD). Both involve lung inflammation in the newborn period but differ in cause, timing, and pathology.
1. Neonatal Pneumonia
Lung infection/inflammation presenting within the first days to weeks of life.
Causes (by organism)
| Organism | Notes |
|---|---|
| Group B Streptococcus | Most common; acquired in utero or during delivery |
| E. coli, Listeria, Klebsiella | Early-onset (<48 hrs); severe, fulminant |
| Chlamydia trachomatis | Late onset (>3 weeks); "staccato" cough, conjunctivitis |
| Bordetella pertussis | Apnea may be the only sign; characteristic whoop absent in neonates |
| Mycobacterium tuberculosis | Transplacental or via infected amniotic fluid |
Features
- Respiratory distress, temperature instability (high or low), poor feeding, lethargy
- Chest X-ray: infiltrates, hyperinflation (Chlamydia), or diffuse haziness
Management
- Sepsis workup (blood/urine cultures, CXR, CBC)
- Parenteral ampicillin + gentamicin (adjust to sensitivities)
- Macrolide for Chlamydia/pertussis
(Tintinalli's Emergency Medicine)
2. Bronchopulmonary Dysplasia (BPD)
Chronic inflammatory lung disease in premature infants - a result of an immature lung being injured by treatment required to keep the infant alive.
Two Forms
| "Old" BPD | "New" BPD | |
|---|---|---|
| Infants | Larger, late-preterm with RDS | Extremely preterm (<1000 g) |
| Cause | O₂ toxicity + barotrauma from ventilation | Developmental arrest + inflammation |
| Histology | Airway metaplasia, fibrosis, cystic changes | Simplified enlarged alveoli, impaired capillary development |
| X-ray | Cysts + alternating atelectasis/hyperinflation | Bilateral diffuse haziness (microatelectasis) |
Key Risk Factors
- Extreme prematurity (main driver)
- Oxygen toxicity - hyperoxia in first 2 weeks linked to BPD severity
- Barotrauma/volutrauma from mechanical ventilation
- Prenatal and postnatal inflammation (e.g., chorioamnionitis)
Diagnosis
Clinically defined as need for supplemental O₂ at 36 weeks' corrected gestational age.
Consequences
- Ventilation-perfusion mismatch
- Increased work of breathing
- In severe cases: pulmonary hypertension, progressive respiratory failure, high mortality
Prevention/Management
- Antenatal corticosteroids (accelerates lung maturation)
- Perinatal surfactant replacement
- Gentle ventilation strategies (avoid volutrauma)
- Target O₂ saturations carefully (both hyper- and hypoxemia carry risks)
- Room air or blended O₂ (30%) preferred for initial resuscitation
(Creasy & Resnik's Maternal-Fetal Medicine; Murray & Nadel's Respiratory Medicine)
In brief: Neonatal pneumonia is an infectious lung inflammation (bacteria/Chlamydia/pertussis) presenting within days to weeks of birth; BPD is a chronic inflammatory-fibrotic lung disease of premature infants caused by oxygen toxicity, mechanical ventilation, and lung immaturity. Both present with respiratory distress and require early, targeted intervention.
What is respiratory distress syndrome (RDS) of the newborn?
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Excellent - I now have pathophysiology diagram, histology image, CXR, and comprehensive text from Robbins Pathology, Grainger & Allison Radiology, and Creasy & Resnik MFM. Here is the full answer:
Respiratory Distress Syndrome (RDS) of the Newborn
Also called Hyaline Membrane Disease (HMD) or Idiopathic RDS (IRDS) - it is the most common cause of respiratory insufficiency in newborns, primarily affecting premature infants.
Definition
RDS is a disorder of premature infants caused by surfactant deficiency in the immature lung. Without sufficient surfactant, alveoli collapse at end-expiration, leading to progressive atelectasis, hypoxia, and respiratory failure.
Incidence
| Gestational Age | Incidence of RDS |
|---|---|
| < 28 weeks | ~60% |
| 28-34 weeks | ~30% |
| > 34 weeks | < 5% |
Risk Factors
Increased risk:
- Prematurity (main factor)
- Male gender
- Maternal diabetes (high insulin suppresses surfactant synthesis)
- Cesarean section before onset of labor (labor stimulates surfactant synthesis)
- Multiple gestation
Decreased risk (protective):
- Intrauterine stress / fetal growth restriction (elevates fetal corticosteroids → stimulates surfactant)
- Prolonged rupture of membranes
- Antenatal corticosteroid administration
Pathogenesis
The core defect is failure of the immature type II pneumocytes to synthesize sufficient surfactant.
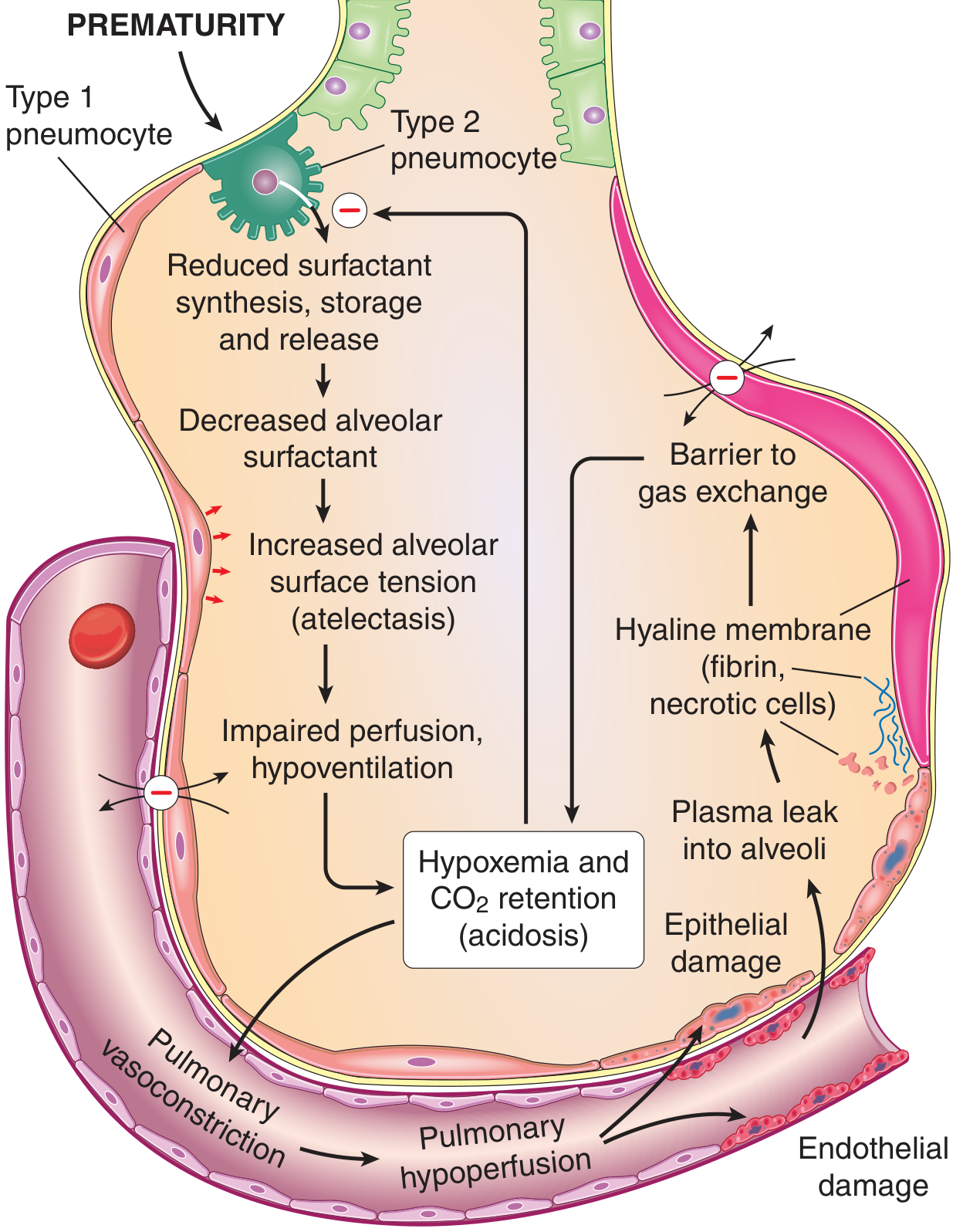
The cascade:
- Prematurity → type II pneumocytes cannot synthesize adequate surfactant (principally dipalmitoyl phosphatidylcholine / lecithin)
- Decreased alveolar surfactant → increased alveolar surface tension
- Alveolar collapse (atelectasis) at end-expiration - infant must re-open collapsed alveoli with every breath
- Infant tires rapidly from the enormous inspiratory effort → generalized atelectasis
- Hypoxia + hypercarbia + acidosis → pulmonary vasoconstriction → pulmonary hypoperfusion
- Endothelial and epithelial damage → plasma leaks into alveoli
- Leaked plasma (fibrin + necrotic cells) forms the characteristic eosinophilic hyaline membranes lining respiratory bronchioles, alveolar ducts, and alveoli
Importantly: corticosteroids stimulate surfactant synthesis, explaining why antenatal steroids are protective and why maternal diabetes (high insulin antagonizing cortisol) is a risk factor.
Morphology / Histology
Gross: Lungs are of normal size but heavy, relatively airless, and mottled purple (atelectatic).
Microscopy:
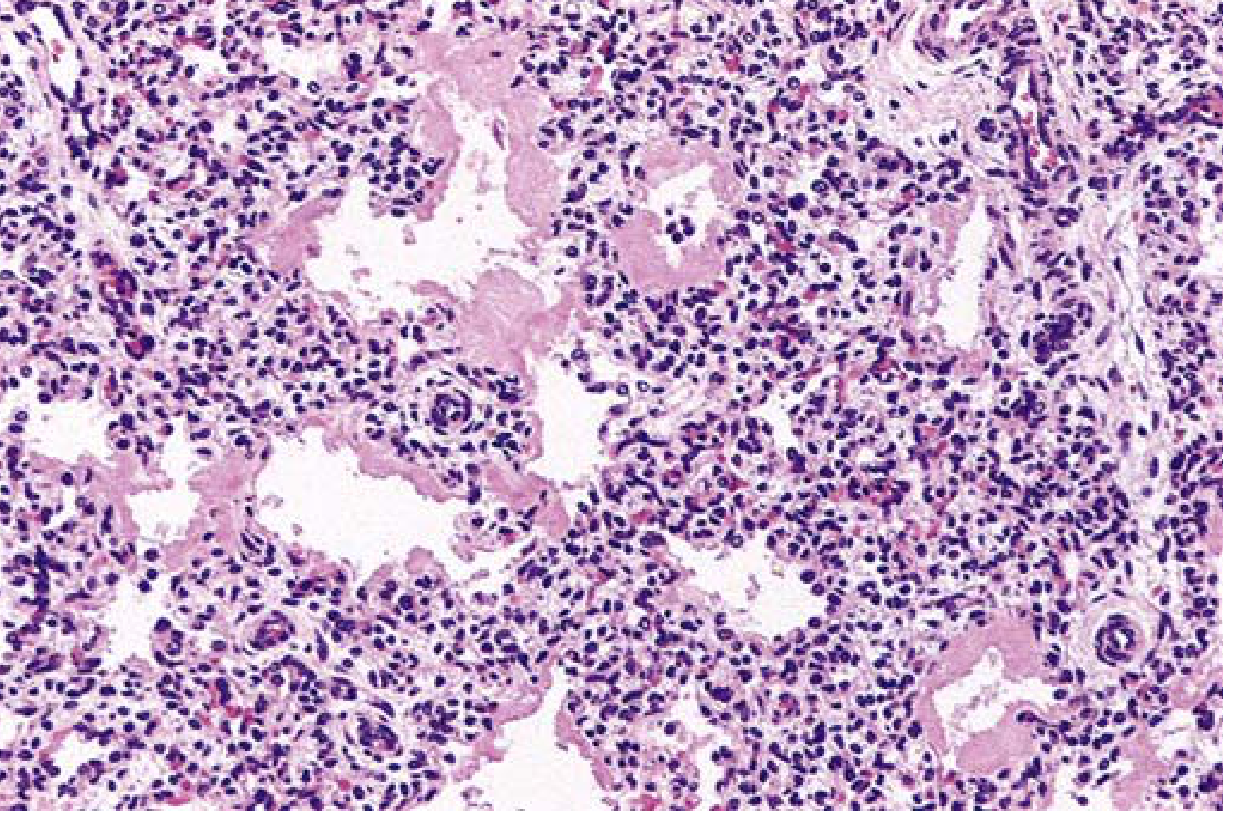
- Alternating collapsed (atelectatic) and dilated alveoli
- Thick, eosinophilic hyaline membranes lining respiratory bronchioles and alveolar ducts (composed of fibrin + necrotic type II pneumocytes)
- Notably absent: neutrophilic inflammatory reaction
- After several days (if survival): proliferation of type II pneumocytes + interstitial fibrosis (reparative phase)
- Hyaline membranes are NOT seen in stillborns or infants dying within the first few hours
Clinical Features
Symptoms appear within minutes of birth:
- Tachypnoea (respiratory rate > 60/min)
- Grunting (expiratory - infant tries to generate PEEP by partially closing glottis)
- Intercostal / subcostal retractions
- Nasal flaring
- Cyanosis
Chest X-Ray Findings

Classic radiographic features:
- Under-aeration (low lung volumes)
- Fine, diffuse, symmetrical granular opacification (ground-glass appearance)
- Air bronchograms - collapsed alveoli around patent bronchioles make the airways visible
- Severe cases: "white-out" of the lungs
- Very premature (<26 weeks): may have clear lungs initially due to structural immaturity
After surfactant treatment: patchy, asymmetric aeration (surfactant may not distribute evenly).
Diagnosis
Primarily clinical + radiological. Prenatal assessment of lung maturity:
- Lecithin/Sphingomyelin (L/S) ratio in amniotic fluid ≥ 2 indicates adequate surfactant/lung maturity
- Phosphatidylglycerol presence in amniotic fluid - additional marker of maturity
Treatment
| Intervention | Details |
|---|---|
| Antenatal corticosteroids | Betamethasone/dexamethasone to mother 48 hrs before delivery - stimulates fetal surfactant synthesis |
| Exogenous surfactant | Given as liquid bolus via ET tube at birth (prophylactic in <28 wks); dramatically reduces severity |
| CPAP | Keeps alveoli open at end-expiration; reduces need for intubation |
| Mechanical ventilation | For severe cases; use gentle strategies to avoid barotrauma |
| Oxygen | Titrate carefully - avoid both hypoxia and hyperoxia |
| High-frequency oscillatory ventilation | Reduces barotrauma in very premature infants |
Recovery begins within 3-4 days in uncomplicated cases.
Complications
| Complication | Mechanism |
|---|---|
| Bronchopulmonary Dysplasia (BPD) | Oxygen toxicity + prolonged ventilation → chronic lung disease |
| Retinopathy of prematurity | Hyperoxia → VEGF suppression → retinal vessel damage; then rebound neovascularization |
| Patent Ductus Arteriosus (PDA) | Common in premature infants; worsened by improved oxygenation after surfactant |
| Intraventricular hemorrhage | Fragile premature cerebral vasculature |
| Necrotizing Enterocolitis (NEC) | Hypoxia and gut immaturity |
| Pneumothorax / PIE | Barotrauma from positive pressure ventilation |
| Pulmonary hemorrhage | Severe hypoxia → capillary damage |
Key Points Summary
- RDS = surfactant deficiency in premature lungs → alveolar collapse → hypoxia → hyaline membrane formation
- Hallmark histology: eosinophilic hyaline membranes (fibrin + necrotic type II cells)
- Hallmark CXR: diffuse granular opacification + air bronchograms + low volumes
- Antenatal steroids + postnatal surfactant have transformed outcomes - death from acute RDS is now uncommon
- RDS can progress to BPD (chronic lung disease of prematurity) - the main long-term complication
(Sources: Robbins & Kumar Basic Pathology; Grainger & Allison's Diagnostic Radiology; Creasy & Resnik's Maternal-Fetal Medicine)
This is a shared conversation. Sign in to Orris to start your own chat.