Bilateral footdrop cause
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I now have comprehensive information from multiple authoritative neurology textbooks. Here is a structured answer:
Bilateral Foot Drop — Causes
Foot drop (inability to dorsiflex the foot) is unilateral when a single common peroneal nerve or L5 root is affected. Bilateral involvement implies a process that is either systemic, bilateral in the spinal cord, or involves the motor unit more diffusely. Causes are best organized by anatomical level:
1. Central / Upper Motor Neuron (Spinal Cord)
Bilateral foot drop with spasticity and upper motor neuron signs points to spinal cord disease:
- Spastic paraparesis from myelopathy (cervical spondylosis, MS, transverse myelitis, tumor, AVM)
- Scissor gait / paraparetic gait with bilateral foot drop, extended knees, and adductor crossover
2. Anterior Horn Cell (Lower Motor Neuron — Spinal)
- Amyotrophic lateral sclerosis (ALS) / Motor Neuron Disease — may begin distally and asymmetrically in the legs
- Progressive Spinal Muscular Atrophy (PSMA)
- Poliomyelitis
3. Lumbosacral Roots
- Bilateral L4–L5 radiculopathy — disc disease, spinal stenosis, cauda equina lesion
- Lumbar plexopathy (bilateral, e.g., retroperitoneal disease)
4. Peripheral Nerve (Polyneuropathy) — Most Common Cause
The most frequent cause of bilateral foot drop:
| Cause | Key Features |
|---|---|
| Charcot-Marie-Tooth disease (CMT / peroneal muscular atrophy) | Hereditary; progressive bilateral foot drop + wrist drop over decades; pes cavus |
| Diabetic polyneuropathy | Length-dependent; distal sensorimotor |
| Inflammatory polyneuropathy (CIDP, GBS) | Acute or subacute; demyelinating |
| Paraproteinemic neuropathy | M-protein; often demyelinating |
| Toxic neuropathy (lead, alcohol) | Lead → bilateral wrist + foot drop; alcohol-nutritional |
| Hereditary Pressure Palsy (HNPP) | Recurrent nerve palsies |
| Sarcoid neuropathy | May present with bilateral foot drop |
| Vasculitic neuropathy | Mononeuritis multiplex → can become bilateral |
5. Neuromuscular Junction
- Typically does not produce isolated foot drop
6. Muscle (Myopathy)
Bilateral foot drop with distal weakness (no sensory loss):
| Cause | Key Features |
|---|---|
| Distal muscular dystrophies (Welander, Miyoshi, Nonaka/GNE) | Progressive bilateral foot drop; onset in early/mid adult life |
| Scapuloperoneal muscular dystrophy | Bilateral foot drop + scapulohumeral involvement |
| Emery-Dreifuss muscular dystrophy | Bilateral foot drop variant described |
| Myotonic dystrophy (DM1/DM2) | Distal leg + forearm + face + eyes |
| Facioscapulohumeral dystrophy (FSHD) | Scapuloperoneal variant with bilateral foot drop |
| Inclusion Body Myositis (IBM) | Asymmetric distal weakness; quadriceps + finger flexors most prominent |
7. Other
- Dystonia — action dystonia of the foot can mimic foot drop
- Sensory ataxia (severe deafferentation, e.g., tabes dorsalis, subacute combined degeneration) — steppage gait with pseudo-foot drop due to proprioceptive loss
Key Distinguishing Points
| Feature | Peripheral nerve | Anterior horn cell | Myopathy | Cord |
|---|---|---|---|---|
| Sensory loss | Yes (polyneuropathy) | No | No | Yes (level) |
| Reflexes | Reduced/absent | Reduced/absent | Reduced | Increased |
| Fasciculations | Rare | Yes | No | No |
| Pattern | Distal, symmetric | Often asymmetric | Distal or proximal | Spastic, UMN signs |
Sources:
- Adams and Victor's Principles of Neurology, 12th Ed. — Steppage gait, distal bilateral limb palsies
- Bradley and Daroff's Neurology in Clinical Practice — Box 25.2: Causes of Foot Drop
- Localization in Clinical Neurology, 8th Ed. — Steppage gait, bilateral foot drop
- Adams and Victor's Principles of Neurology, 12th Ed. — Distal muscular dystrophies, scapuloperoneal dystrophy
Wrist drop causes
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive data. Here is the structured answer:
Wrist Drop — Causes
Wrist drop (inability to extend the wrist and fingers) results from loss of function of the wrist extensors, primarily innervated by the radial nerve (C7). Causes are organized by anatomical level.
1. Radial Nerve Palsy — By Site of Lesion (Most Common Overall Cause)
A. Axillary (High) Radial Nerve Lesion
| Cause | Features |
|---|---|
| Crutch palsy — chronic pressure in axilla from improper crutch use | Wrist drop + triceps weakness + sensory loss |
| Axillary mass / tumour | Wrist drop + triceps weakness |
Triceps is affected here because branches to triceps arise proximal to the spiral groove.
B. Spiral Groove (Mid-Humeral) Lesion — Most Common Site
| Cause | Features |
|---|---|
| "Saturday night palsy" — sleeping with arm draped over bench/chair back while intoxicated | Wrist drop; triceps usually spared (branches arise before spiral groove) |
| Humeral shaft fracture | Wrist drop; triceps usually spared; check radial nerve after all mid-shaft humerus fractures |
| Compression during anaesthesia / improper positioning | "Park bench palsy" |
| Callus formation after healed fracture | Delayed palsy |
| "Honeymooner's palsy" — lover's head on partner's arm during sleep | Same mechanism as Saturday night palsy |
| Tourniquet palsy | Operative complication |
C. Posterior Interosseous Nerve (PIN) Entrapment — Distal to Elbow
- Entrapment in the radial tunnel (at the arcade of Frohse / supinator muscle)
- Trauma or dislocation of radial head
- Lipoma, ganglion, synovial cyst compressing the nerve
- Features: Finger drop (extensors of wrist and fingers weak) but no sensory loss and no true wrist drop — wrist extensors (extensor carpi radialis longus) are partially spared, so the wrist deviates radially on extension rather than fully dropping.
D. Distal / Superficial Radial Nerve Lesion
- Tight wristbands, handcuffs, IV catheter — sensory loss only (cheiralgia paresthetica), no wrist drop
2. C7 Nerve Root Radiculopathy
- C6–C7 disc herniation — the most common cervical root involved
- Wrist drop + triceps weakness + triceps reflex loss + sensory loss over 2nd and 3rd digits
- Causes: cervical disc prolapse, cervical spondylosis, tumour, trauma
3. Brachial Plexus (Posterior Cord / Middle Trunk)
- Posterior cord lesion of the brachial plexus — wrist drop + deltoid weakness (axillary nerve also from posterior cord)
- Erb-Duchenne palsy (C5–C6) — affects upper trunk; does NOT typically cause wrist drop
- Pancoast tumour (apical lung tumour) invading lower plexus — predominantly C8/T1 but can extend
4. Cortical / Central (Rare)
- Cerebral cortical infarct in the "hand knob" area of the precentral gyrus can mimic wrist drop (pseudo-radial nerve palsy) — but the weakness is upper motor neuron (spastic, hyperreflexic, no sensory loss in radial distribution)
5. Toxic / Systemic Causes (Bilateral Wrist Drop)
| Cause | Notes |
|---|---|
| Lead neuropathy | Classic cause of bilateral wrist drop ± foot drop; predominantly motor; painless; associated with lead lines on gum (Burton's lines) and basophilic stippling |
| Arsenic neuropathy | Distal motor and sensory neuropathy |
| Dapsone neuropathy | Predominantly motor neuropathy |
| Distal muscular dystrophies | Bilateral wrist + foot drop (Welander, CMT) |
| Charcot-Marie-Tooth disease | Progressive bilateral distal weakness; wrist drop + foot drop |
| Mononeuritis multiplex | Vasculitis, diabetes, sarcoid, leprous neuropathy — asymmetric nerve involvement |
6. Summary by Level
| Level | Cause | Triceps | Sensory Loss |
|---|---|---|---|
| Axilla (pre-spiral) | Crutch palsy | Weak | Yes |
| Spiral groove | Saturday night palsy, # humerus | Spared | Yes (dorsal hand) |
| Elbow / PIN | Radial tunnel entrapment | Spared | No |
| C7 root | Disc herniation | Weak | Digits 2–3 |
| Posterior cord plexus | Plexus injury | Weak (deltoid also) | Yes |
| Cortex (pseudo-palsy) | Stroke "hand knob" | Spared | No radial-pattern loss |
| Bilateral (toxic) | Lead, CMT | Variable | Variable |
Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed. — Radial neuropathy
- Neuroanatomy through Clinical Cases, 3rd Ed. — Radial neuropathy, upper extremity nerve injuries
- General Anatomy & Musculoskeletal System (THIEME Atlas) — Wrist drop; radial nerve lesion sites
- Bradley and Daroff's Neurology in Clinical Practice — Radial neuropathy; lead neuropathy
- Localization in Clinical Neurology, 8th Ed. — Pseudo-radial nerve palsy (cortical)
- Katzung's Basic & Clinical Pharmacology, 16th Ed. — Lead-induced wrist drop
Wasting of small muscle of hand dd
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Excellent — I have rich data from multiple authoritative sources. Here is the comprehensive differential diagnosis:
Wasting of the Small Muscles of the Hand — Differential Diagnosis
The small (intrinsic) muscles of the hand are the lumbricals, interossei, thenar (LOAF muscles — median nerve), and hypothenar muscles (ulnar nerve). Their motor supply converges at C8–T1. Wasting is therefore the hallmark of pathology at any level from C8–T1 downwards.
Anatomical Framework
Cortex / UMN → Spinal cord (C8–T1) → Anterior horn cells
→ Nerve roots (C8, T1) → Lower trunk brachial plexus
→ Median + Ulnar nerves → Intrinsic hand muscles
1. Peripheral Nerve
Ulnar Nerve Palsy
- Compression at elbow (cubital tunnel / ulnar groove) — most common cause of intrinsic wasting
- Compression at wrist (Guyon's canal) — hypothenar + interossei, sparing forearm muscles
- Chronic pressure from air hammers, prolonged leaning on elbow
- Wasting of hypothenar eminence, first dorsal interosseous, interossei → claw hand (4th & 5th fingers)
- Associated: sensory loss over 4th–5th fingers and ulnar border
Median Nerve Palsy
- Carpal tunnel syndrome — most common peripheral nerve entrapment; thenar wasting (LOAF muscles)
- Proximal median nerve compression (pronator teres, anterior interosseous nerve)
- Features: thenar (lateral) wasting; sensory loss over thumb/index/middle finger; positive Tinel/Phalen
Combined Ulnar + Median = Complete Intrinsic Wasting
- Both nerves injured → "all-intrinsic" wasting
2. Brachial Plexus (Lower Trunk — C8, T1)
| Cause | Notes |
|---|---|
| Pancoast tumour (superior sulcus apical lung carcinoma) | Classic — lower trunk compression; wasting + pain + Horner syndrome (T1 sympathetics) |
| Cervical rib / thoracic outlet syndrome | Compression of C8–T1 / lower trunk; hypothenar + interossei wasting; ulnar-side paresthesias |
| Klumpke's palsy (Dejerine-Klumpke) | Birth injury (breech), traction on abducted arm; wasting of all small hand muscles + clawhand |
| Post-radiation plexopathy | After axillary/breast radiotherapy; typically painless paresthesias |
| Infiltrating tumour | Breast, lymphoma invading plexus |
| Neuralgic amyotrophy (Parsonage-Turner) | Acute onset, usually upper plexus, but lower plexus forms exist |
3. Nerve Roots (C8–T1)
| Cause | Notes |
|---|---|
| Cervical spondylosis (C7–T1 disc) | Radiculopathy; wasting may be unilateral; neck pain/stiffness |
| Cervical disc prolapse | C8 or T1 root compression |
| Cervical cord compression (myelopathy) | "Hand wasting in spondylotic high cord compression" — selective C8–T1 anterior horn ischaemia with UMN signs in legs |
| Tumours (extradural, intradural) | Metastases, meningioma, neurofibroma |
4. Spinal Cord (C8–T1 Anterior Horn / Cord)
| Cause | Notes |
|---|---|
| Motor Neuron Disease / ALS | Bilateral wasting + fasciculations; often starts in one hand; UMN + LMN signs; no sensory loss |
| Progressive Muscular Atrophy (PMA) | Pure LMN variant of MND |
| Syringomyelia | Central cord cavitation at C8–T1; dissociated sensory loss (pain/temp lost, touch preserved); cape distribution; bilateral wasting; kyphoscoliosis |
| Spinal Muscular Atrophy (SMA) | Kennedy disease (SBMA) — X-linked; bulbar + hand wasting |
| Poliomyelitis / Post-polio syndrome | Asymmetric LMN wasting; history of childhood illness |
| Intramedullary tumour (ependymoma, glioma) | Cord expansion on MRI |
5. Distal Myopathy / Muscle Disease
| Cause | Notes |
|---|---|
| Inclusion Body Myositis (IBM) | Selective involvement of finger flexors (FDP) + quadriceps; distal hand wasting; middle-aged/elderly |
| Distal muscular dystrophies (Welander, Miyoshi, Nonaka) | Bilateral progressive distal wasting |
| Myotonic dystrophy (DM1) | Distal hand wasting + myotonia + frontal baldness + cataracts + cardiac conduction defects |
6. Vasculitic / Multifocal Neuropathy
| Cause | Notes |
|---|---|
| Mononeuritis multiplex | Vasculitis (RA, PAN, SLE), diabetes, sarcoid, leprosy — asymmetric involvement of multiple named nerves |
| Leprous neuropathy | Thickened ulnar/median nerves; predilection for cool superficial nerve segments |
Summary Table by Distribution
| Pattern of Wasting | Most Likely Level/Cause |
|---|---|
| Thenar only | Median nerve (CTS, proximal median palsy), C6–C7 radiculopathy |
| Hypothenar + interossei | Ulnar nerve (elbow/wrist) |
| All intrinsics (bilateral) | ALS/MND, syringomyelia, cervical cord compression, bilateral CTS + ulnar palsy |
| All intrinsics + Horner + pain | Pancoast tumour |
| All intrinsics + clawhand + sensory ulnar border | Lower brachial plexus (Klumpke, TOS, cervical rib) |
| Distal wasting + myotonia | Myotonic dystrophy |
| Distal finger flexors + quadriceps | IBM |
| Wasting + fasciculations + UMN signs | ALS |
| Wasting + dissociated sensory loss | Syringomyelia |
Sources:
- Adams and Victor's Principles of Neurology, 12th Ed. — Lower brachial plexus paralysis; thoracic outlet syndrome
- Bradley and Daroff's Neurology in Clinical Practice — Ulnar neuropathy; thoracic outlet; ALS
- Eric Kandel Principles of Neural Science, 6th Ed. — ALS and hand wasting
- Gray's Anatomy for Students — Cervical rib; intrinsic wasting
- Harrison's Principles of Internal Medicine, 22nd Ed. — Thoracic outlet syndrome
- Localization in Clinical Neurology, 8th Ed. — Cervical cord; syringomyelia
Small muscle of hand wasting approach for diagnosis investigations and Differential for viva
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Now I have everything needed for a comprehensive viva-style answer. Let me compile it:
Small Muscles of the Hand — Wasting: A Complete Viva Approach
Step 1: Anatomy — What Are the Small Muscles of the Hand?
The small (intrinsic) hand muscles receive their motor supply almost exclusively from C8 and T1 spinal segments via the median and ulnar nerves:
| Muscle Group | Nerve | Root |
|---|---|---|
| Thenar (APB, opponens pollicis, FPB superficial head) | Median (recurrent branch) | C8, T1 |
| Hypothenar (ADM, FDM, opponens digiti minimi) | Ulnar (deep branch) | C8, T1 |
| Lumbricals 1 & 2 | Median | C8, T1 |
| Lumbricals 3 & 4, all interossei, adductor pollicis, FPB deep head | Ulnar (deep branch) | C8, T1 |
Viva key point: All intrinsic hand muscles are C8–T1. Any lesion affecting C8–T1 at any level can cause wasting.
Step 2: Clinical Approach — History
Ask systematically to localize before investigating:
A. Pattern of wasting
- Thenar only → median nerve (CTS) until proven otherwise
- Hypothenar + interossei → ulnar nerve
- All intrinsics, unilateral → C8/T1 root, lower trunk, or cord
- All intrinsics, bilateral → ALS, syringomyelia, bilateral entrapment, distal myopathy
B. Sensory symptoms
- Thumb/index/middle fingers, nocturnal → CTS (median)
- Ring/little finger, medial forearm → ulnar nerve / lower trunk
- Dissociated (pain/temp lost, touch preserved) → syringomyelia
- No sensory loss → anterior horn cell (ALS, PMA) or myopathy
C. Pain
- Neck pain + arm radiation → cervical radiculopathy/spondylosis
- Severe shoulder/arm pain at onset → Pancoast tumour, Parsonage-Turner
- Aching ulnar forearm → thoracic outlet syndrome
- Painless progressive → ALS, hereditary neuropathy (CMT), myopathy
D. Other features
- Fasciculations → anterior horn cell disease
- Horner syndrome (ptosis, miosis, anhidrosis) → C8/T1 lesion, Pancoast, syringomyelia
- Legs involved → consider cord lesion (ALS, spondylotic myelopathy, syringomyelia)
- Occupation/trauma → entrapment, repetitive stress
- Bilateral wrist + foot drop → lead neuropathy, CMT, myopathy
Step 3: Clinical Examination Approach
General Inspection
- Thenar wasting → flat thenar eminence (CTS, median palsy, C6–C7 but also C8 root)
- Hypothenar + first dorsal interosseous wasting → ulnar palsy (characteristic "guttering")
- All intrinsics → generalised pitting on dorsum
- Claw hand → ulnar (4th/5th) or all fingers (combined median + ulnar)
- Fasciculations → ALS
Motor Testing
| Test | Muscle | Nerve |
|---|---|---|
| Thumb abduction against resistance | APB | Median |
| Little finger abduction | ADM | Ulnar |
| Index finger abduction (Froment-adjacent) | First dorsal interosseous | Ulnar |
| Adductor pollicis (Froment's test — paper held between thumb and index) | Adductor pollicis | Ulnar |
Reflexes
| Reflex | Root |
|---|---|
| Triceps | C7 |
| Finger flexors (Hoffman / inverted supinator) | C8–T1 |
Absent finger flexor reflex = C8/T1 involvement at root or cord level
Sensory Testing
- Map carefully: median territory (lateral 3½ digits), ulnar (medial 1½), T1 inner forearm
- Test pain/temp separately from touch → if dissociated = syringomyelia
Look for Associated Signs
| Finding | Significance |
|---|---|
| Horner syndrome | C8/T1 sympathetics — Pancoast, TOS, syringomyelia |
| UMN signs in legs (spastic paraparesis, hyperreflexia, upgoing plantar) | Cord lesion — spondylotic myelopathy, ALS, syringomyelia |
| Fasciculations in tongue + limbs | ALS |
| Thickened ulnar nerve at elbow | Leprosy, CMT, chronic entrapment |
| Numb/clumsy hands + wide-based gait | Spondylotic cervical myelopathy |
| Myotonia on percussion | Myotonic dystrophy |
| "Split-hand" pattern (thenar + FDI > hypothenar) | Specific for ALS |
Step 4: Localization Framework
Cortex → rarely (pseudoulnar palsy with parietal/precentral infarct)
↓
Cervical cord (C8–T1) → spondylotic myelopathy, syringomyelia,
ALS, intramedullary tumour
↓
Nerve roots (C8, T1) → disc prolapse, spondylosis, trauma
↓
Lower trunk / brachial plexus → Pancoast, cervical rib/TOS, Klumpke
↓
Peripheral nerve → ulnar (elbow/wrist), median (CTS), combined
↓
Neuromuscular junction → not a significant cause
↓
Muscle → IBM, distal dystrophy, myotonic dystrophy
Step 5: Key Differentiating Features (High-Yield Viva)
| Diagnosis | Wasting Pattern | Sensory | Reflexes | Other Clues |
|---|---|---|---|---|
| CTS | Thenar | Thumb/index/middle (nocturnal) | Normal | Tinel/Phalen positive, nocturnal pain |
| Ulnar neuropathy at elbow | Hypothenar + interossei | Ring/little + ulnar forearm | Normal | Clawing 4–5, Froment +ve |
| Lower trunk plexopathy (Pancoast / TOS) | All intrinsics | Medial forearm + ulnar hand | ↓ finger flexor | Horner, shoulder/arm pain, apical lung mass |
| C8/T1 radiculopathy | All intrinsics | Medial forearm/arm | ↓ finger flexor | Neck pain, reproduced by neck movement |
| Spondylotic cervical myelopathy | C8–T1 intrinsics | Numb clumsy hands | LMN at level, UMN below | UMN signs legs, bladder involvement |
| Syringomyelia | C8–T1, bilateral | Dissociated (cape distribution) | ↓ at level, ↑ below | Horner, kyphoscoliosis, Chiari |
| ALS | Split-hand (APB/FDI > ADM) | None | Mixed (LMN + UMN) | Fasciculations, bulbar signs, no sensory loss |
| Lead neuropathy | Bilateral, distal | Minimal | ↓ | Bilateral wrist + foot drop, Burton's lines |
| CMT (HMSN) | Bilateral distal | Mild distal | ↓ | Pes cavus, stork legs, family history |
| Myotonic dystrophy | Distal hand | Absent | ↓ | Myotonia, frontal baldness, cataracts, cardiac |
| IBM | Finger flexors (FDP) + quadriceps | Absent | ↓ | Age >50, asymmetric, falls |
| Klumpke's palsy | All intrinsics | Medial arm/forearm/hand | ↓ | Birth injury, clawhand, Horner |
| Leprosy | Ulnar > median distribution | Hypoaesthetic patches | ↓ | Thickened nerves, painless injuries, endemic area |
Step 6: Investigations
First-Line
| Investigation | What It Detects |
|---|---|
| NCS (nerve conduction studies) | Localizes peripheral nerve lesion; median/ulnar conduction velocity, latency, amplitude |
| EMG (electromyography) | Denervation (fibrillations, positive sharp waves) = LMN lesion; split-hand pattern → ALS; myopathic changes (small polyphasic MUPs) |
| MRI cervical spine | Cord compression (spondylosis, disc, tumour), syrinx, intramedullary pathology |
Second-Line (Targeted)
| Investigation | Indication |
|---|---|
| Chest X-ray / CT chest | Pancoast tumour (apical opacity), cervical rib |
| MRI brachial plexus | Plexus infiltration, TOS, Pancoast |
| Serum CK | Raised in myopathy (IBM, dystrophy) |
| Anti-GM1, anti-ganglioside antibodies | Multifocal motor neuropathy (MMN) — motor-only neuropathy mimicking ALS |
| Blood lead level, 24-hr urine lead | Lead neuropathy |
| Serology (ANCA, ANA, RF, cryoglobulins) | Vasculitic neuropathy / mononeuritis multiplex |
| Nerve biopsy | Vasculitis, amyloid, leprosy |
| Muscle biopsy | IBM (COX-negative fibres, rimmed vacuoles), dystrophy |
| Genetic testing | CMT (PMP22, MPZ mutations), Kennedy disease (CAG repeat in androgen receptor), SMA |
| ACE, chest imaging | Sarcoid neuropathy |
| Abdominal fat pad / rectal biopsy | Amyloid neuropathy |
Step 7: Classic Viva Questions & Answers
Q: What is split-hand syndrome and what does it indicate?
A: Preferential wasting of the APB (median) and first dorsal interosseous (FDI, ulnar) over the ADM (ulnar hypothenar), despite all being C8/T1 muscles. It is specific to ALS and reflects greater excitability/vulnerability of corticospinal projections to APB and FDI motor neurons.
Q: What is the significance of Horner syndrome with hand wasting?
A: Indicates a C8/T1 lesion interrupting sympathetic fibres — think Pancoast tumour, syringomyelia, or Klumpke's palsy.
Q: How do you differentiate CTS from C6–C7 radiculopathy?
A: CTS affects thenar muscles but spares forearm muscles (pronator teres, FCR). C7 radiculopathy causes wrist extensor weakness (wrist drop tendency), triceps weakness, and triceps reflex loss. NCS in CTS shows prolonged distal latency across the wrist.
Q: What is the "numb clumsy hands" syndrome?
A: A presentation of spondylotic cervical myelopathy — intrinsic hand wasting (C8/T1 anterior horn ischaemia) with a glove-pattern sensory loss and UMN signs in the lower limbs, caused by venous stagnation in the mid-cervical cord.
Q: Why can a C3–C5 cord lesion cause C8–T1 hand wasting?
A: Spondylotic narrowing at C3–C5 can cause stagnant venous hypoxia spreading to C8–T1 anterior horn cells distally, causing intrinsic hand wasting despite the mechanical lesion being at a higher level.
Sources:
- Localization in Clinical Neurology, 8th Ed. — Split-hand; C8/T1 cord lesions; spondylotic myelopathy; TOS
- Adams and Victor's Principles of Neurology, 12th Ed. — Lower plexus paralysis; TOS; patterns of myopathic weakness
- Bradley and Daroff's Neurology in Clinical Practice — Radial/ulnar/median neuropathy; ALS split-hand; TOS electrodiagnostics
- Harrison's Principles of Internal Medicine, 22nd Ed. — TOS; nerve investigations
- Eric Kandel Principles of Neural Science, 6th Ed. — ALS and hand wasting
Worsening of stroke pt on day 7
Finding Sources
Finding Sources
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Cheery red spot
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Now I have everything needed for a comprehensive answer. Here is the complete coverage:
Cherry-Red Spot — Complete Overview
Definition & Mechanism
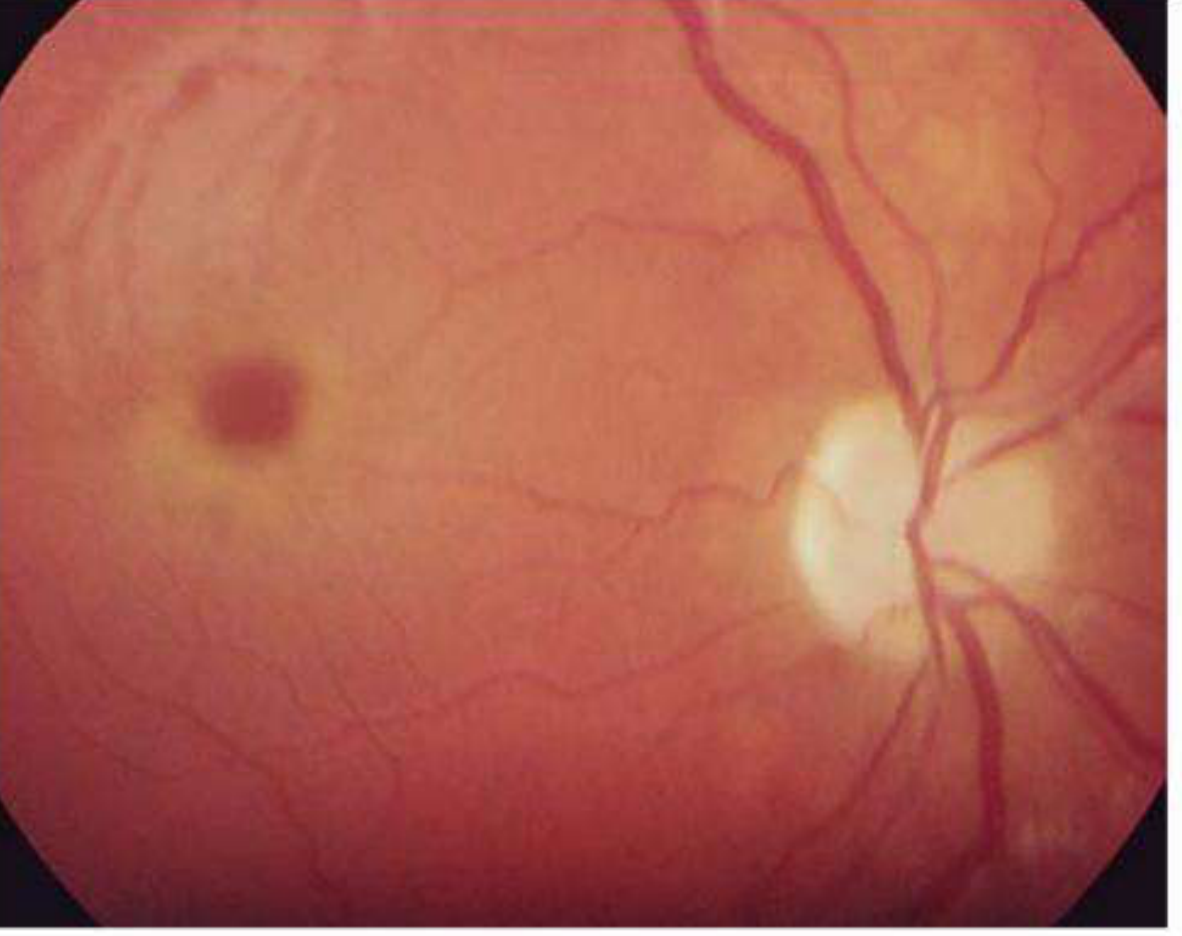
A cherry-red spot is a fundoscopic sign at the fovea (centre of the macula) where a bright red/orange area contrasts against an abnormally pale, whitened surrounding retina.
Why it appears — two distinct mechanisms:
| Mechanism | Example |
|---|---|
| Retinal ischaemia/oedema — ischaemic retina becomes opaque white; the fovea, being the thinnest part of the retina with no overlying ganglion cells, remains transparent and the underlying orange-red choroidal circulation is visible | Central retinal artery occlusion (CRAO) |
| Storage material accumulation — lipid/glycolipid deposits in retinal ganglion cells surrounding the fovea make the perifoveal ring opaque; the fovea itself (devoid of ganglion cells) remains clear and the choroid shows through | Tay-Sachs, Niemann-Pick, etc. |
Key point: The fovea appears red in both cases for the same reason — it has no ganglion cells, so the choroidal blush is unobstructed; the surrounding retina is white/opaque due to ischaemia or storage material.
Causes — Classified
1. Vascular (Acute — Unilateral)
| Cause | Notes |
|---|---|
| Central Retinal Artery Occlusion (CRAO) | Most common vascular cause; sudden painless monocular visual loss; cherry-red spot is the pathognomonic sign; disappears within days as retina atrophies |
| Cilioretinal artery occlusion (if fovea is involved) | Less common; partial visual field loss |
| Ophthalmic artery occlusion | Usually NO cherry-red spot — entire retina whitens including fovea (no choroidal perfusion either) |
Etiology of CRAO (for viva):
- Emboli: cholesterol (Hollenhorst plaque — carotid atheromas), calcium (cardiac valves), platelet-fibrin
- Thrombosis: in situ; associated with carotid stenosis, GCA
- GCA (giant cell arteritis) — always exclude in >55 yr
- Cardiac embolism (AF, endocarditis, valvular disease)
- Hypercoagulable states, sickle cell disease
2. Lysosomal Storage Diseases (Bilateral — Symmetric — Present in Infancy/Childhood)
| Disease | Enzyme Defect | Inheritance | Additional Features |
|---|---|---|---|
| Tay-Sachs disease (GM2 gangliosidosis — HexA deficiency) | Hexosaminidase A | AR; Ashkenazi Jewish | Onset 3–6 months; hypotonia → hyperreflexia → seizures → blindness → death by 2–4 yrs; NO organomegaly |
| Sandhoff disease (GM2 gangliosidosis — HexA+B deficiency) | Hexosaminidase A and B | AR; non-Jewish | Same as Tay-Sachs + hepatosplenomegaly, bone marrow involvement |
| GM1 gangliosidosis | β-Galactosidase | AR | Severe neuro + coarse facies, hepatosplenomegaly; death by age 2 |
| Niemann-Pick disease type A | Sphingomyelinase | AR; Ashkenazi Jewish | Hepatosplenomegaly, progressive neuro deterioration; cherry-red spot in types A and B only (not type C) |
| Niemann-Pick disease type B | Sphingomyelinase (partial) | AR | Milder; visceral disease predominant; ring may be diffuse/indistinct |
| Sialidosis (Mucolipidosis type I) | Neuraminidase (sialidase) | AR | Late-onset form: myoclonus + seizures ("cherry-red spot myoclonus syndrome"); more severe infantile form has corneal clouding + optic atrophy |
| Farber disease (lipogranulomatosis) | Ceramidase | AR | Aphonia, periarticular nodules, dermatitis, psychomotor retardation; pinguecula-like conjunctival lesions |
| Metachromatic leukodystrophy | Arylsulfatase A | AR | Rare cause; primarily white matter disease |
3. Toxic Causes
- Carbon monoxide poisoning
- Methanol poisoning
- Quinine toxicity
- Dapsone toxicity
- Gentamicin toxicity (intraocular)
4. Trauma
- Commotio retinae (Berlin's oedema) — blunt ocular trauma; retinal whitening from photoreceptor outer segment fragmentation; cherry-red spot at posterior pole; usually resolves spontaneously but may mimic CRAO
Key Distinguishing Points (Viva)
| Feature | CRAO | Storage Disease |
|---|---|---|
| Laterality | Unilateral | Bilateral |
| Age | Usually adult | Infancy / childhood |
| Onset | Acute (seconds) | Gradual |
| Duration of sign | Disappears in days–weeks | Persists (until retinal degeneration) |
| Systemic associations | Vascular risk factors, cardiac embolism, GCA | Neurological deterioration, hepatosplenomegaly, developmental regression |
| Retinal appearance | Pale retina + boxcar segmentation of vessels | Pale perifoveal halo, optic atrophy later |
Cherry-Red Spot Myoclonus Syndrome
A distinct entity — sialidosis type I (late-onset, adult neuraminidase deficiency) — presenting with:
- Progressive myoclonus (severe, incapacitating, intention myoclonus)
- Visual failure
- Cherry-red spot
- Autosomal recessive; sialidase (neuraminidase) deficiency
- Listed as a cause of myoclonic epilepsy
Important Viva Mnemonics
"TAN FMS" — Storage diseases with cherry-red spot:
- Tay-Sachs (GM2)
- ALS-like variants of hexosaminidase deficiency (adult)
- Niemann-Pick (A, B)
- Farber disease
- Mucolipidosis I / Sialidosis
- Sandhoff disease (GM2)
"No cherry-red spot" clue: Ophthalmic artery occlusion (both retina AND choroid infarcted → retina white, fovea also white) — distinguishes it from CRAO where choroid is intact.
Sources:
- Kanski's Clinical Ophthalmology, 10th Ed. — Cherry-red spot at the macula; storage diseases
- Robbins, Cotran & Kumar Pathologic Basis of Disease — CRAO mechanism; Tay-Sachs; storage diseases
- Adams and Victor's Principles of Neurology, 12th Ed. — Diseases displaying cherry-red macular spot; sialidosis; Tay-Sachs; Sandhoff
- The Wills Eye Manual — Differential diagnosis of cherry-red spot; CRAO etiology
- Rosen's Emergency Medicine — CRAO clinical features
Aseptic meningitis and drugs causing meningitis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
I now have comprehensive data. Here is the full structured answer:
Aseptic Meningitis — Complete Overview
Definition
The term aseptic meningitis (originally coined because bacterial cultures are negative) now refers to a clinical syndrome of meningeal inflammation with:
- Fever, headache, meningismus (neck stiffness, Kernig/Brudzinski signs)
- CSF pleocytosis — predominantly lymphocytic
- Normal CSF glucose (occasionally mildly reduced)
- Mildly elevated CSF protein
- Negative bacterial cultures
It is a syndrome with many causes — the majority are viral, but important non-infectious causes exist.
CSF Profile in Aseptic vs. Bacterial Meningitis
| Parameter | Aseptic Meningitis | Bacterial Meningitis |
|---|---|---|
| Cells | 10–1000 (up to >1000 in LCM) — lymphocytes | Thousands — neutrophils |
| Glucose | Normal (>60% serum) | Low (<45 mg/dL) |
| Protein | Mildly elevated | Markedly elevated |
| Gram stain | Negative | Often positive |
| Culture | Negative | Positive (bacterial) |
Note: In early viral meningitis, neutrophils may predominate for the first 24–48 hours. Also, drug-induced meningitis (especially TMP-SMX) often causes neutrophilic CSF pleocytosis — an important trap.
Causes — Classified
1. Viral (Most Common — 80%+)
| Virus | Notes |
|---|---|
| Enteroviruses (Echovirus, Coxsackievirus) | Most common overall; ~80% of cases where a specific viral cause is identified; summer/autumn peak; may have rash (echovirus 9), herpangina (Coxsackie A) |
| HSV-2 | 2nd most common in adults; associated with genital herpes; most important cause of Mollaret's meningitis (recurrent); cauda equina neuritis |
| HSV-1 | Rare cause of meningitis (usually causes encephalitis) |
| VZV (Varicella-zoster) | Meningitis with/without rash |
| HIV | Acute seroconversion syndrome — mononucleosis-like; meningitis during primary infection |
| Mumps | Now rare (vaccinated populations); males 3× more; glucose may be mildly depressed; orchitis, parotitis |
| EBV (Infectious mononucleosis) | Pharyngitis, lymphadenopathy, splenomegaly; abnormal LFTs |
| CMV | Immunocompromised patients |
| LCM (Lymphocytic choriomeningitis virus) | Rodent contact; intense pleocytosis >1000 cells (all lymphocytes); mild hypoglycorrhachia in 20–30% |
| HHV-6 | Immunosuppressed (transplant, HIV) |
| Parvovirus B19 | Meningitis + encephalitis, particularly in immunosuppressed |
| Arboviruses (West Nile, Dengue, Japanese encephalitis) | Endemic exposure history |
| Adenovirus | Less common |
2. Bacterial (Atypical / Culture-negative)
| Organism | Notes |
|---|---|
| Mycoplasma pneumoniae | Respiratory illness preceding CNS involvement; cold agglutinins ↑ |
| Leptospirosis | Jaundice, hepatitis, renal failure; uveitis (later) |
| Lyme disease (Borrelia burgdorferi) | Tick exposure; facial nerve palsy (CN VII), radiculopathy, arthritis |
| Treponema pallidum (syphilis) | Serology on CSF; secondary/tertiary syphilis |
| Brucellosis | Animal exposure; undulant fever |
| Rickettsial infections (Q fever) | Pneumonia; hepatitis |
| Partially treated bacterial meningitis | Culture-negative but neutrophilic |
| TB meningitis | Subacute/chronic; low glucose; high protein |
3. Non-Infectious — Systemic Disease
| Cause | Notes |
|---|---|
| Systemic Lupus Erythematosus (SLE) | Can cause lymphocytic or neutrophilic pleocytosis; may be thousands/mm³; normal glucose; can recur |
| Sarcoidosis | Chronic; cranial nerve palsies; hypoglycorrhachia |
| Behçet's syndrome | Uveitis, oral/genital ulcers, CNS involvement |
| Familial Mediterranean Fever | Recurrent episodes |
| Granulomatosis with polyangiitis (Wegener's) | Vasculitic; sinus disease |
| Kawasaki disease | Children; coronary aneurysm |
| Still's disease | Systemic juvenile idiopathic arthritis |
| Lead poisoning | Especially in children |
| Cogan syndrome | Interstitial keratitis + audiovestibular disease |
4. Neoplastic (Carcinomatous/Lymphomatous Meningitis)
- Metastatic carcinoma (breast, lung, melanoma)
- CNS tumours: meningeal gliomatosis, dysgerminomas, ependymomas
- Epidermoid/dermoid cyst rupture (releases squamous cells + cholesterol crystals into CSF → chemical meningitis)
- Hypoglycorrhachia is the clue — low CSF glucose suggests neoplastic or granulomatous meningitis
5. Drug-Induced Aseptic Meningitis (DIAM)
A hypersensitivity/idiosyncratic reaction, not dose-dependent; recurs with re-exposure.
A. NSAIDs (Most Common Drug Class)
| Drug | Notes |
|---|---|
| Ibuprofen | Most frequently implicated NSAID; can occur at therapeutic doses or overdose; idiosyncratic; propionic acid derivatives as a class |
| Naproxen, ketoprofen, sulindac | Same class |
| Diclofenac | Less common |
| Tolmetin | Described in SLE patients especially |
Patients with SLE and connective tissue diseases have disproportionately higher risk of NSAID-induced meningitis.
B. Antimicrobials
| Drug | Notes |
|---|---|
| Trimethoprim-sulfamethoxazole (Co-trimoxazole) | Important cause; classically causes neutrophilic pleocytosis (not the usual lymphocytic pattern) |
| Amoxicillin / Penicillin | Rare |
| Isoniazid | Rare |
| Ciprofloxacin | Reported |
C. Immunologics / Biologics
| Drug | Notes |
|---|---|
| Intravenous Immunoglobulin (IVIG) | Relatively well-recognised complication; mechanism unclear — possibly aggregated IgG activating complement; usually resolves; occurs in normal and IgA-deficient patients |
| OKT3 (Muromonab-CD3) | Anti-T cell antibody used in transplant; well-known cause |
| Immunoglobulin preparations generally | Including subcutaneous forms |
D. Other Drugs
| Drug | Notes |
|---|---|
| Intrathecal agents — methotrexate, cytarabine, contrast media | Chemical meningitis; sclerosing arachnoiditis with persistent pleocytosis |
| Carbamazepine | Rare |
| Azathioprine | Rare reports |
| Allopurinol | Rare |
| Ranitidine | Rare |
| Lamotrigine | Rare |
6. Chemical/Inflammatory (Non-Drug)
- Epidermoid/dermoid cyst rupture — cholesterol crystals, keratin in CSF
- Craniopharyngioma leakage
- Post-neurosurgical or post-LP chemical irritation
- Intrathecal contrast or drugs → arachnoiditis
Mollaret's Meningitis (Recurrent Benign Lymphocytic Meningitis)
- HSV-2 is the primary cause (>80% of cases confirmed by CSF PCR)
- Recurrent self-limited episodes of headache, fever, meningismus over years
- Each attack lasts a few days and resolves spontaneously
- Classic CSF finding: Mollaret cells — large ghost-like endothelial/epithelioid cells (pathognomonic but transient)
- Drug-induced meningitis (NSAIDs, IVIG) can also recur with re-exposure and mimic this syndrome
- Also caused by: SLE, dermoid cyst leakage, Behçet's disease
Key Viva Points
Q: What is the most common cause of aseptic meningitis?
A: Enteroviruses (echovirus and Coxsackievirus) — 80% of cases where an aetiology is established.
Q: Which drug most commonly causes aseptic meningitis?
A: Ibuprofen (and other propionic acid derivative NSAIDs); IVIG is another well-recognised cause.
Q: How does drug-induced meningitis differ from viral meningitis on CSF?
A: DIAM (especially TMP-SMX) often causes neutrophilic pleocytosis rather than the expected lymphocytic response — a trap that can mimic bacterial meningitis.
Q: In which patients are NSAIDs most likely to cause aseptic meningitis?
A: Patients with SLE and connective tissue diseases are at disproportionately higher risk.
Q: What is Mollaret's meningitis caused by?
A: Predominantly HSV-2 (>80%); characterised by recurrent self-limited attacks with Mollaret cells in CSF.
Q: What non-infectious cause gives low CSF glucose (hypoglycorrhachia)?
A: Malignant (carcinomatous/lymphomatous) meningitis and sarcoidosis — important to distinguish from TB.
Sources:
- Adams and Victor's Principles of Neurology, 12th Ed. — Acute aseptic meningitis; causes; CSF findings
- Goldman-Cecil Medicine — Non-infectious causes of aseptic meningitis; drug hypersensitivity table
- Bradley and Daroff's Neurology in Clinical Practice — Recurrent meningitis; Mollaret's; NSAID-induced; IVIG
- Rosen's Emergency Medicine — NSAID-induced meningitis; ibuprofen
- Harrison's Principles of Internal Medicine, 22nd Ed. — Viral meningitis; CSF differentiation
Causes of optic neuritis
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive, authoritative data. Here is the complete structured answer:
Causes of Optic Neuritis
Definition
Optic neuritis is inflammation of the optic nerve causing acute/subacute visual loss, typically with:
- Pain on eye movement (~90%)
- Reduced visual acuity and colour vision (red desaturation)
- Relative Afferent Pupillary Defect (RAPD) — Marcus Gunn pupil
- Visual field defect (central/cecocentral scotoma most common)
- Disc swelling (papillitis) in ~1/3; normal disc (retrobulbar neuritis) in ~2/3
- Uhthoff's sign — worsening with heat/exercise (suggests demyelination)
Classification: Typical vs. Atypical
| Feature | Typical | Atypical |
|---|---|---|
| Laterality | Unilateral | Bilateral |
| Pain | Present (90%) | May be absent |
| Recovery | Good (starts within 1 month) | Poor |
| Disc swelling | Mild if present | Severe / haemorrhages / exudates |
| Associated cause | MS / idiopathic | NMOSD, MOGAD, infectious |
| Risk of MS | High (72% at 15 yrs if MRI lesions) | Negligible |
Causes — Classified
1. Demyelinating Disease (Most Common in Adults — ~85% of Typical Cases)
| Cause | Notes |
|---|---|
| Multiple Sclerosis (MS) | By far the most common overall; optic neuritis is the initial presentation of MS in ~25%; risk of developing MS within 15 years is 72% if MRI shows T2 lesions, 25% if MRI normal at presentation |
| Neuromyelitis Optica Spectrum Disorder (NMOSD / Devic disease) | Anti-AQP4-IgG (anti-aquaporin-4); severe, bilateral, often simultaneous optic neuritis; long-segment transverse myelitis; poor visual recovery; typically middle-aged women |
| MOG Antibody Disease (MOGAD) | Anti-MOG-IgG (myelin oligodendrocyte glycoprotein); bilateral simultaneous optic neuritis common; distinct from MS and NMOSD; better recovery |
| Acute Disseminated Encephalomyelitis (ADEM) | Post-infectious/post-vaccination; multifocal CNS demyelination; children > adults |
| Schilder's disease | Very rare; relentlessly progressive; bilateral optic neuritis; onset <10 years |
| Isolated/Idiopathic optic neuritis | Clinically Isolated Syndrome (CIS) — first demyelinating event; high conversion risk to MS |
2. Infectious Causes
Viral
| Virus | Notes |
|---|---|
| Measles | Post-infectious; more common in children |
| Mumps | Parotitis, orchitis; post-infectious ON |
| Chickenpox (VZV) | Post-infectious ON in children; zoster ophthalmicus in adults |
| Herpes zoster | Direct viral and post-infectious involvement |
| EBV (Infectious mononucleosis) | Pharyngitis, lymphadenopathy, hepatitis |
| HSV | Direct and post-infectious |
| HIV | Directly or via opportunistic co-infections |
| Encephalitis viruses (CMV, HHV-6) | Immunocompromised patients |
Bacterial
| Organism | Notes |
|---|---|
| Syphilis (Treponema pallidum) | Neuroretinitis pattern; CSF VDRL; any age |
| Tuberculosis | Granulomatous ON; chronic; associated with TB meningitis |
| Lyme disease (Borrelia burgdorferi) | Tick exposure; facial palsy, arthritis |
| Bartonella henselae (Cat scratch disease) | Neuroretinitis with macular star (stellate maculopathy + disc swelling); self-limited |
| Brucellosis | Animal/unpasteurised milk exposure |
Fungal
| Organism | Notes |
|---|---|
| Cryptococcus neoformans | Immunocompromised; meningitis; intracranial hypertension can compress optic nerves |
Parasitic
| Organism | Notes |
|---|---|
| Toxoplasma gondii | Posterior uveitis + optic nerve involvement |
| Toxocara | Rare; choroidoretinitis spreading to optic nerve |
3. Autoimmune / Systemic Inflammatory Diseases
| Cause | Notes |
|---|---|
| Sarcoidosis | Granulomatous optic neuritis; may be bilateral; uveitis, cranial nerve palsies; chest disease |
| Systemic Lupus Erythematosus (SLE) | Vasculitic or immune-mediated; can cause optic neuritis or ischaemic optic neuropathy |
| Sjögren's syndrome | Associated with optic neuritis; may overlap with NMOSD |
| Antiphospholipid antibody syndrome | Vascular and inflammatory optic nerve disease |
| Behçet's disease | Uveitis, oral/genital ulcers; neuroretinitis |
| Chronic Relapsing Inflammatory Optic Neuropathy (CRION) | Steroid-responsive; recurrent; seronegative |
| Wegener's granulomatosis (GPA) | Orbital involvement compressing/infiltrating optic nerve |
4. Contiguous Spread / Local Inflammation
- Orbital cellulitis / abscess
- Sinusitis (especially ethmoid/sphenoid — posterior orbit)
- Meningitis — meningeal inflammation spreading to optic nerve sheath
- Orbital tumour — compressive, mimics optic neuritis
5. Post-Infectious / Post-Vaccination
- Childhood vaccinations (measles, mumps, varicella)
- Post-viral syndrome (ADEM spectrum)
- Often bilateral in children; viral infection ~2–4 weeks prior
6. Special Situations
| Situation | Notes |
|---|---|
| Pregnancy | Can precipitate MS relapse including optic neuritis |
| Neuroretinitis | Disc swelling + macular star (Leber's stellate maculopathy); usually infectious (Bartonella); not associated with MS |
| Toxic/Nutritional optic neuropathy | Painless, bilateral, progressive — NOT true optic neuritis but important DD: alcohol, tobacco-alcohol amblyopia, ethambutol, isoniazid, chloroquine, heavy metals, B12 deficiency |
| Leber's Hereditary Optic Neuropathy (LHON) | Mitochondrial; males; sequential painless bilateral visual loss; optic atrophy; peripapillary telangiectasia — important DD |
Key Differentials of Optic Neuritis
| Condition | Pain? | Laterality | Disc | Visual loss | Clue |
|---|---|---|---|---|---|
| Optic neuritis | Yes (90%) | Unilateral usually | Normal or mild swelling | Over days | RAPD, colour loss, Uhthoff |
| NAION | Usually no | Unilateral | Hyperaemic → pale swelling | Sudden | Age >50, altitudinal field defect |
| GCA (arteritic AION) | Headache, scalp tenderness | Unilateral | Chalk-white swelling | Sudden | ESR/CRP elevated, age >55 |
| Papilledema | Headache (raised ICP) | Bilateral | Swollen | Preserved early | No colour loss, no RAPD |
| LHON | No | Bilateral (sequential) | Telangiectasia → atrophy | Subacute | Young male, mitochondrial DNA |
| Compressive optic neuropathy | No / proptosis | Unilateral | Pale or swollen | Gradual | MRI mass lesion |
| Toxic optic neuropathy | No | Bilateral | Normal → pale | Painless, progressive | Drug/nutritional history |
MS Risk After First Optic Neuritis (Optic Neuritis Treatment Trial)
| MRI at onset | 15-year MS risk |
|---|---|
| ≥1 T2 lesion | 72% |
| No lesions | 25% |
Sources:
- Bradley and Daroff's Neurology in Clinical Practice — Typical/atypical optic neuritis; MS; NMOSD; MS risk; OCT
- The Wills Eye Manual — Etiology; differential diagnosis; Uhthoff; signs; MOGAD
- Kanski's Clinical Ophthalmology, 10th Ed. — Demyelinating optic neuritis; NMOSD; MOGAD; Schilder's
- Harrison's Principles of Internal Medicine, 22nd Ed. — NMOSD optic neuritis; visual loss
- Tintinalli's Emergency Medicine — Infectious causes; post-vaccination; workup
- Goldman-Cecil Medicine — Systemic inflammatory and infectious associations
Elderly female with pancerebellar inv - history to ask , examination, investigations and dd
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.


Screenshot_20260603_121322_Xodo.jpg
Screenshot_20260603_121309_Xodo.jpg
Prepare me a list of matching rak wise result with roll number
Here is the DM - Neurology result list with AML Rank and CML Rank matched by Roll Number:
30. DM - Neurology — Combined Rank List
| Roll No. | AML Rank | Total Marks (100) | CML Rank | Theory Marks (80) |
|---|---|---|---|---|
| 5180053 | 1 | 89.667 | 1 | 70.667 |
| 5185357 | 2 | 88.333 | 2 | 70.333 |
| 5183092 | 3 | 77.667 | 7 | 60.667 |
| 5181813 | 4 | 77.333 | 3 | 62.333 |
| 5181795 | 5 | 76.333 | 5 | 61.333 |
| 5182522 | 6 | 75.667 | 11 | 56.667 |
| 5180977 | 7 | 75.000 | 9 | 59.000 |
| 5183106 | 8 | 73.333 | 4 | 61.333 |
| 5182844 | 9 | 72.333 | 10 | 57.333 |
| 5185476 | 10 | 70.333 | 15 | 56.333 |
| 5180051 | 11 | 69.667 | 12 | 56.667 |
| 5180985 | 12 | 67.333 | 25 | 53.333 |
| 5183351 | 13 | 67.333 | — | — |
| 5180492 | 14 | 66.333 | 16 | 56.333 |
| 5184240 | 15 | 66.000 | 6 | 61.000 |
| 5185800 | 16 | 65.667 | 22 | 53.667 |
| 5182613 | 17 | 65.667 | — | — |
| 5182053 | 18 | 65.333 | — | — |
| 5184413 | 19 | 64.333 | 14 | 56.333 |
| 5181428 | 20 | 64.000 | 8 | 59.000 |
| 5183902 | 21 | 63.333 | — | — |
| 5182840 | 22 | 62.667 | — | — |
| 5183609 | 23 | 62.000 | 17 | 56.000 |
| 5181444 | 24 | 61.667 | — | — |
| 5180981 | 25 | 61.667 | — | — |
| 5184100 | 26 | 61.333 | 13 | 56.333 |
| 5181442 | 27 | 61.333 | 19 | 55.333 |
| 5184321 | — | — | 18 | 55.333 |
| 5181803 | — | — | 20 | 54.667 |
| 5184421 | — | — | 21 | 54.333 |
| 5183369 | — | — | 23 | 53.667 |
| 5185560 | — | — | 24 | 53.667 |
| 5180490 | — | — | 26 | 53.000 |
Notes:
- "—" means that roll number did not appear in the visible portion of the other list (may be on a page not shown).
- The images show only partial data — image 1 shows AML Ranks 1–27, image 2 shows CML Ranks 1–26. Some roll numbers appear in one list but not the other within the visible range.
- AML Rank = based on Total Marks out of 100 (includes practical/viva).
- CML Rank = based on Theory Marks out of 80 only.
Would you like this exported as an Excel or PDF file?
This is a shared conversation. Sign in to Orris to start your own chat.