most common congenital heart disease
Reading File
Searching PubMed
congenital heart disease prevalence epidemiology
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have rich, authoritative content to give a thorough answer. Here it is:
Most Common Congenital Heart Diseases
Congenital heart disease (CHD) affects approximately 6-8 per 1,000 live births. The defects are broadly classified by their hemodynamic pattern into left-to-right shunts (acyanotic), right-to-left shunts (cyanotic), and obstructive lesions.
Frequency Ranking
| Rank | Defect | % of all CHD |
|---|---|---|
| 1 | Ventricular Septal Defect (VSD) | ~25-35% |
| 2 | Atrial Septal Defect (ASD) | ~6-10% |
| 3 | Patent Ductus Arteriosus (PDA) | ~6-8% |
| 4 | Pulmonary Stenosis | ~5-7% |
| 5 | Tetralogy of Fallot (TOF) | ~5-10% |
| 6 | Coarctation of the Aorta | ~5-7% |
| 7 | Transposition of Great Arteries (TGA) | ~3-5% |
| 8 | Atrioventricular (AV) Canal Defect | ~2-3% |
Class 1: Left-to-Right Shunts (Acyanotic - most common group)
These are collectively the most common type of congenital cardiac malformations. They do not cause early cyanosis but can eventually lead to Eisenmenger syndrome with chronic pulmonary hypertension.
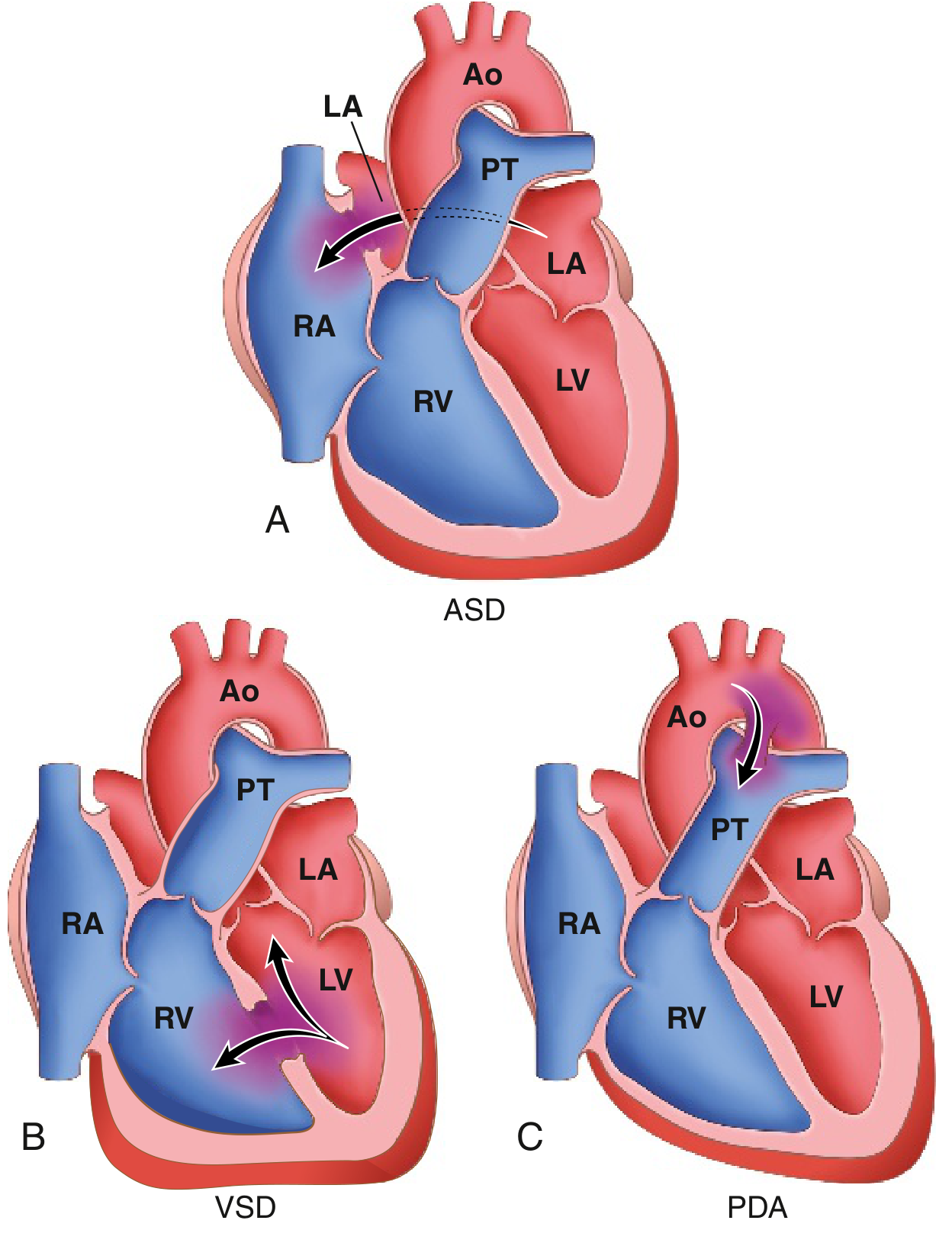
1. Ventricular Septal Defect (VSD) - #1 Most Common
-
Accounts for 25-35% of all CHD - the single most common congenital cardiac anomaly
-
Most frequently located in the membranous (perimembranous/outlet) portion of the interventricular septum
-
Other locations: muscular, inlet (AV canal type), subpulmonary (conal septal)
-
Small VSDs spontaneously close in many children during early life; muscular defects are often pressure-restricted with no hemodynamic consequence
-
Large VSDs cause symptoms of heart failure and poor somatic growth, requiring surgical closure before adulthood
-
Classic murmur: harsh holosystolic murmur at the left sternal border
-
Harrison's Principles of Internal Medicine 22E, p. 2115; Morgan and Mikhail's Clinical Anesthesiology, p. 3039
2. Atrial Septal Defect (ASD)
-
Third most common CHD overall; 1-2 per 1,000 live births, representing ~1% of CHDs (second most common in adults, as many VSDs close)
-
Types:
- Ostium secundum (90% of ASDs) - smooth-walled defect near the foramen ovale; most common type
- Ostium primum (~10%) - located in the lower atrial septum; often associated with mitral valve cleft
- Sinus venosus - near the SVC-RA junction; associated with partial anomalous pulmonary venous return
-
ASD causes right atrial and ventricular volume overload; right ventricular hypertrophy and pulmonary artery dilation
-
Women with unoperated ASD generally tolerate pregnancy well
-
Mulholland and Greenfield's Surgery, p. 1206; Robbins & Kumar Basic Pathology
3. Patent Ductus Arteriosus (PDA)
-
Connection between the aortic isthmus and the origin of the pulmonary artery, normally closing after birth
-
Small PDAs are silent and hemodynamically insignificant
-
Large PDAs cause left heart dilation and can lead to chronically elevated pulmonary vascular resistance and Eisenmenger syndrome
-
Classic murmur: continuous "machinery" murmur heard best below the left clavicle, extending from systole past S2 into diastole (reflects flow gradient from aorta to pulmonary artery)
-
Harrison's Principles of Internal Medicine 22E, p. 2116
Class 2: Right-to-Left Shunts (Cyanotic)
These cause early cyanosis because deoxygenated blood enters the systemic circulation.
4. Tetralogy of Fallot (TOF) - Most Common Cyanotic CHD
-
Occurs in 0.5 per 1,000 live births; most common cyanotic defect in the postinfancy period, accounting for up to 10% of all CHD
-
Four features (all result from anterosuperior displacement of the infundibular septum):
- Large VSD
- Right ventricular outflow tract obstruction (subpulmonic stenosis)
- Overriding aorta
- Right ventricular hypertrophy
-
"Boot-shaped heart" on CXR (coeur en sabot)
-
Severity depends on the degree of pulmonic outflow obstruction
-
The pulmonic stenosis paradoxically protects the pulmonary vasculature from hypertension - right heart failure is rare
-
Treatment: primary surgical repair in infancy
-
Harrison's Principles of Internal Medicine 22E, p. 2116; Robbins & Kumar Basic Pathology
5. Transposition of the Great Arteries (TGA)
- Aorta arises from the RV and the pulmonary artery from the LV - creating two parallel, non-communicating circulations
- Most common cyanotic CHD presenting at birth (neonatal emergency)
- Survival depends on a mixing lesion (PFO, VSD, or PDA)
- Requires urgent surgical correction (arterial switch operation)
Class 3: Obstructive Lesions
- Pulmonary stenosis - most commonly valvular; can be isolated or part of TOF
- Coarctation of the aorta - narrowing of the aorta, typically near the ligamentum arteriosum; associated with bicuspid aortic valve (50%); presents with upper extremity hypertension and weak femoral pulses
- Aortic stenosis - congenital bicuspid aortic valve is the most common congenital cardiac anomaly if PFO is excluded
Key Concept: Eisenmenger Syndrome
With any large, uncorrected left-to-right shunt (VSD, ASD, PDA), chronic pulmonary overcirculation eventually causes irreversible pulmonary hypertension. Once pressures equalize or reverse, the shunt becomes right-to-left, causing cyanosis - this is Eisenmenger syndrome. At this point, structural repair is contraindicated.
- Robbins & Kumar Basic Pathology, p. 348
Summary: VSD is the single most common CHD (~25-35%), followed by ASD and PDA. Collectively, the left-to-right shunt group is the most prevalent category. Among cyanotic defects, Tetralogy of Fallot leads in the postinfancy period, while TGA is the most common cyanotic CHD presenting at birth.
This is a shared conversation. Sign in to Orris to start your own chat.