heart blocks-definition,etiology, classification, symptoms, diagnosis, treatment
Reading File
Finding Sources
Finding Sources
Searching PubMed
"atrioventricular block" OR "heart block"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Searching Images
heart block ECG atrioventricular block types first second third degree
I now have comprehensive content. Let me compile the complete, well-organized answer:
Heart Blocks (Atrioventricular Block)
1. Definition
Heart block (atrioventricular block) is a disturbance of impulse conduction from the atria to the ventricles that can be permanent or transient, depending on anatomic or functional impairment of the AV conduction system. It must be distinguished from interference, a physiologic phenomenon caused by normal refractoriness from a preceding impulse.
AV block exists when an atrial impulse is conducted with delay, or is not conducted at all to the ventricles, at a time when the AV junction is not physiologically refractory. The site of block may be in the:
- AV node (most common in first- and type I second-degree block)
- Bundle of His (infrahisian block)
- Bundle branches / Purkinje system (trifascicular block, usually acquired)
— Braunwald's Heart Disease, p. 579
2. Etiology
| Category | Examples |
|---|---|
| Ischemic / Coronary | AV node ischemia in inferior MI; infranodal block in anterior MI |
| Degenerative | Lev's disease (fibrosis of the left side of the cardiac skeleton), Lenègre's disease (diffuse fibrosis of the bundle branches) — primary degeneration in elderly |
| Inflammatory / Infectious | Rheumatic fever, diphtheria, Lyme disease (Borrelia), viral myocarditis, infective endocarditis with paravalvular abscess |
| Infiltrative | Sarcoidosis, amyloidosis, scleroderma |
| Autoimmune | SLE (congenital CHB via maternal anti-Ro/SSA antibodies), rheumatoid nodules |
| Congenital | Structural heart defects (L-TGA, AV septal defect), maternal anti-Ro antibodies |
| Calcific / Compressive | Calcific aortic stenosis, tumors, calcified annulus |
| Iatrogenic / Drug-induced | Digitalis, beta-blockers, calcium channel blockers, antiarrhythmics (e.g., amiodarone) |
| Vagal / Neurally mediated | Carotid sinus hypersensitivity, vasovagal syncope, Bezold-Jarisch reflex (inferior MI) |
| Metabolic | Hypothyroidism, hyperkalemia, hyperthyroidism (rare) |
| Neuromuscular | Myotonic dystrophy, Kearns-Sayre syndrome, Erb's dystrophy |
| Post-surgical / Traumatic | Cardiac surgery, catheter ablation, TAVI |
| Genetic | SCN5A mutations (also linked to LQT3) |
| Parasitic | Chagas disease |
— Braunwald's Heart Disease, p. 581; Guyton & Hall Medical Physiology, p. 167
3. Classification
Broad Classification of Heart Blocks
| Type | Alternate Name |
|---|---|
| Sinoatrial (SA) block | Exit block |
| Intra-atrial block | |
| Atrioventricular (AV) block | Heart block |
| Intraventricular block | Bundle branch block / fascicular block |
The most clinically relevant is AV block, classified by severity:
Degree-Based Classification of AV Block
🔹 First-Degree AV Block
- Every atrial impulse is conducted to the ventricles, but conduction time is prolonged
- ECG: PR interval > 0.20 sec (200 ms); narrow QRS (if delay is at AV node)
- Site: Usually AV nodal; rarely His-Purkinje
- Clinically benign; normal variant in up to 2% of healthy young adults
- Requires no treatment except withdrawal of nodal-blocking agents
🔹 Second-Degree AV Block
Some but not all atrial impulses reach the ventricles (conduction ratio > 1:1).
| Feature | Type I (Wenckebach / Mobitz I) | Type II (Mobitz II) |
|---|---|---|
| Site of block | AV node (proximal) | Infranodal — bundle of His or bundle branches |
| PR interval | Progressive lengthening then dropped beat | Fixed PR, sudden non-conducted P wave (no warning) |
| QRS | Usually narrow | Usually wide (BBB pattern) |
| Prognosis | Generally benign; often reversible | Serious — may progress to complete block |
| Post-MI | Inferior MI; usually transient | Anterior MI; high mortality |
| Treatment | Often observation; atropine for symptomatic | Pacemaker required |
2:1 AV Block — a special case where every other P wave is blocked; cannot be classified as Mobitz I or II without a longer strip. If QRS is wide → likely Mobitz II; narrow QRS → likely Wenckebach.
High-Grade (Advanced) AV Block — Two or more consecutive P waves fail to conduct, yet some conduction persists intermittently. Etiologies include ACS, rheumatic heart disease, autoimmune disorders, myocarditis, and infiltrative cardiomyopathies. Clinical presentation is indistinguishable from third-degree block.
🔹 Third-Degree (Complete) AV Block
- No atrial impulses conduct to the ventricles; atria and ventricles beat completely independently (AV dissociation)
- Subsidiary pacemaker takes over ventricular rhythm
- AV nodal block (usually congenital): narrow QRS, escape rate 40–60 bpm, more stable
- Infranodal block (usually acquired): wide QRS, escape rate < 40 bpm, less stable, more serious
- ECG: P waves and QRS complexes march through each other at different rates; no relationship between P and QRS
4. ECG Summary Comparison
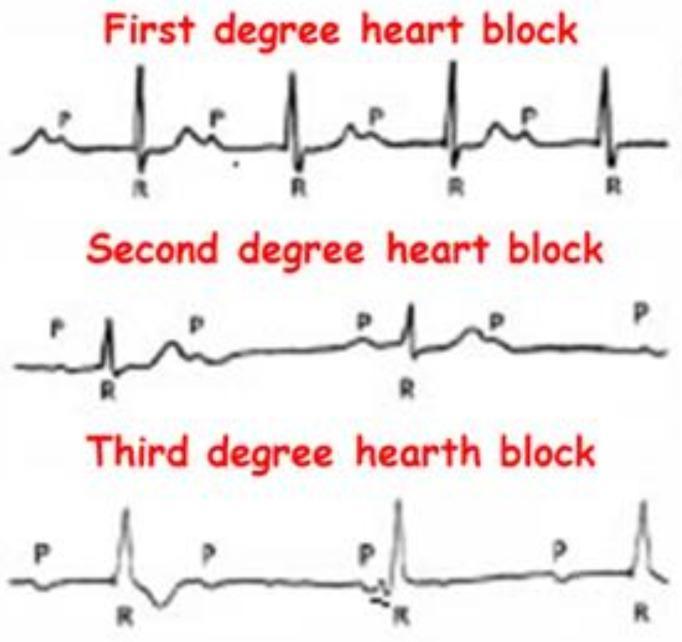
ECG comparison of first-, second-, and third-degree heart block. Note progressive PR lengthening in Wenckebach, fixed PR with sudden dropped beat in Mobitz II, and complete AV dissociation in third-degree block.
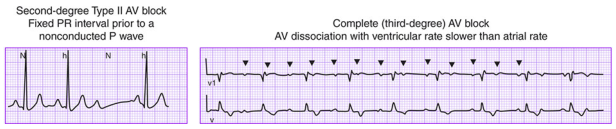
Left: Second-degree Type II — fixed PR interval before a non-conducted P wave. Right: Complete (third-degree) AV block — AV dissociation with ventricular rate slower than atrial rate. (Harrison's Principles of Internal Medicine)
5. Symptoms
Symptoms depend on the degree of block and resulting ventricular rate:
| Degree | Typical Symptoms |
|---|---|
| First-degree | Usually asymptomatic; incidental finding on ECG |
| Second-degree Mobitz I | Often asymptomatic; occasional palpitations, mild fatigue |
| Second-degree Mobitz II / High-grade | Palpitations, fatigue, presyncope, syncope (Stokes-Adams attacks) |
| Third-degree (complete) | Marked fatigue, exertional dyspnea, presyncope/syncope, lightheadedness, heart failure, sudden cardiac death |
Physical examination findings in complete AV block:
- Irregular cannon A waves in the jugular venous pulse (when atria contract against closed tricuspid valve)
- Variable intensity S1 (as PR interval changes)
- Slow, regular pulse (ventricular escape rate)
- Bruit de canon — very loud S1 when PR interval is very short; cyclic variation
Stokes-Adams attacks: Episodes of sudden syncope (or presyncope) from abrupt transition to complete heart block with ventricular asystole before the escape pacemaker takes over. The patient classically goes pale, loses consciousness, then flushes as the escape rhythm restores perfusion.
6. Diagnosis
12-Lead ECG (Primary Tool)
| Block | ECG Finding |
|---|---|
| 1° AV block | PR > 200 ms, every P followed by QRS |
| 2° Mobitz I | Progressive PR prolongation → dropped QRS → repeating cycles |
| 2° Mobitz II | Fixed PR, sudden non-conducted P wave; wide QRS usually |
| 2:1 block | Alternating conducted/non-conducted P waves |
| 3° complete | P waves and QRS complexes completely dissociated; two separate rates |
Additional Investigations
- Ambulatory (Holter) monitoring / Event recorder — for paroxysmal or intermittent block; Holter for 24–48 h; extended loop recorder for weeks; implantable loop recorder (ILR) for months when infrequent symptoms
- Exercise stress test — infranodal block often worsens with exercise; AV nodal block may improve with exercise (sympathetic stimulation)
- Electrophysiology study (EPS) — gold standard for localizing site of block; measures A-H interval (AV node) and H-V interval (His-Purkinje system); H-V ≥ 100 ms indicates significant infranodal disease; procainamide or isoproterenol provocation
- Echocardiogram — assess underlying structural heart disease, LV function, cardiomegaly
- Laboratory — electrolytes (K⁺), digoxin levels, TSH, Lyme serology, inflammatory markers, ANA/anti-Ro (if congenital CHB suspected), troponins (if ACS)
- Cardiac MRI — sarcoidosis, myocarditis, infiltrative disease
7. Treatment
Treatment is directed at the underlying cause and at maintaining adequate heart rate and cardiac output.
Acute / Reversible Causes
- Withdraw offending drugs (beta-blockers, digoxin, CCBs, antiarrhythmics)
- Treat electrolyte abnormalities (hyperkalemia)
- Treat underlying infection/inflammation (Lyme disease → antibiotics; sarcoidosis → steroids)
- In inferior MI with AV nodal block → IV atropine 0.5–1.5 mg (usually transient, resolves with reperfusion)
- Caution: Atropine is ineffective and may worsen infranodal (Mobitz II / complete) block — transcutaneous pacing preferred in this setting
Pharmacological (Temporary / Bridge)
| Drug | Use |
|---|---|
| Atropine (IV 0.5–1.5 mg) | AV nodal block (first-line acute); contraindicated in infranodal block |
| Isoproterenol (IV infusion) | Block at any level; increases rate via β1 stimulation; avoid in acute MI |
| Dopamine / Epinephrine | Hemodynamically unstable patients as bridge to pacing |
Drugs cannot reliably maintain adequate heart rate for more than hours to a few days without significant side effects. Pacing is the definitive treatment.
Pacing
Temporary Pacing
- Transcutaneous pacing (TCP): Non-invasive, rapid; used in emergencies for symptomatic high-grade or complete AV block while awaiting definitive therapy
- Transvenous pacing: Temporary wire placed via subclavian/femoral vein; more reliable for bridge to permanent pacemaker
Permanent Pacemaker — Class I Indications
(Per ACC/AHA/HRS Guidelines)
- Third-degree or advanced second-degree AV block with symptomatic bradycardia
- Third-degree or advanced second-degree AV block in an awake patient with asystole > 3 seconds or escape rate < 40 bpm, or infranodal escape rhythm
- Atrial fibrillation with pause ≥ 5 seconds
- Postoperative AV block not expected to resolve
- AV block with neuromuscular diseases (myotonic dystrophy, Kearns-Sayre, Erb's dystrophy)
- Asymptomatic third-degree AV block if cardiomegaly or LV dysfunction is present, or if block is below the AV node
Class IIa (Reasonable) Indications
- Persistent third-degree AV block with escape rate > 40 bpm in asymptomatic adults without cardiomegaly
- Asymptomatic second-degree infranodal AV block
- Asymptomatic Mobitz II with narrow QRS
- First- or second-degree AV block with symptoms mimicking pacemaker syndrome
Post-MI Permanent Pacing
- Indicated for: transient second- or third-degree infranodal AV block with bundle branch block, and for ongoing symptomatic AV block at any level
- Wenckebach block in inferior MI → rarely persistent enough to warrant permanent pacing
Biventricular Pacing (CRT)
- Consider in patients with pre-existing LV dysfunction and AV block requiring pacing, to prevent or reverse heart failure related to chronic right ventricular pacing
— Braunwald's Heart Disease, p. 582–583; Goldman-Cecil Medicine, p. 326–336
Summary Table
| Type | PR interval | Dropped beats | QRS | Site | Risk | Treatment |
|---|---|---|---|---|---|---|
| 1° AV block | > 200 ms | None | Narrow | AV node | Benign | Observe, stop offending drugs |
| 2° Mobitz I (Wenckebach) | Progressive lengthening | Periodic | Narrow | AV node | Low | Observe; atropine if symptomatic |
| 2° Mobitz II | Fixed (constant) | Sudden | Wide (usually) | Infranodal | High | Permanent pacemaker |
| 2:1 block | Fixed | Every other | Wide or narrow | Variable | Variable | Depends on site |
| High-grade | Fixed | ≥2 consecutive | Wide | Infranodal | High | Pacemaker |
| 3° complete | None (AV dissociation) | All | Wide (acquired) or narrow (congenital) | Any | Very high | Permanent pacemaker |
Sources:
- Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 12th Ed., Ch. 68
- Guyton and Hall Textbook of Medical Physiology, 14th Ed., Ch. 13
- Goldman-Cecil Medicine, 27th Ed., Ch. 54
- Rosen's Emergency Medicine, 9th Ed., Ch. 65
Recent Evidence Note: A 2024 systematic review (PMID 38902995) characterizing AV blocks in hyperthyroidism confirms this as a reversible etiology that resolves with treatment of the underlying thyroid disease. A 2024 meta-analysis (PMID 39120658) supports algorithms that minimize unnecessary right ventricular pacing in patients with pacemakers, consistent with the CRT/biventricular pacing guidance above.
This is a shared conversation. Sign in to Orris to start your own chat.