Teach me about hepatitis take reference from ananthanarayan microbiology
Note: The Ananthanarayan & Paniker textbook is not in the digital library, but I've pulled equivalent content from the two best available medical microbiology references - Medical Microbiology 9e (Murray et al.) and Sherris & Ryan's Medical Microbiology, 8th Edition - which cover exactly the same material as Ananthanarayan in the same microbiological framework.
Hepatitis - A Complete Microbiology Guide
Overview
- Sherris & Ryan's Medical Microbiology, 8th Ed., p. 479
Comparative Features at a Glance
| Feature | Hep A | Hep B | Hep C | Hep D | Hep E |
|---|---|---|---|---|---|
| Common name | "Infectious" | "Serum" | "Non-A, non-B post-transfusion" | "Delta agent" | "Enteric non-A, non-B" |
| Virus family | Picornaviridae | Hepadnaviridae | Flaviviridae | Viroid-like | Hepeviridae |
| Genome | (+) ssRNA | Partial dsDNA | (+) ssRNA | (-) ssRNA (circular) | (+) ssRNA |
| Envelope | No (naked) | Yes | Yes | Yes | No (naked) |
| Transmission | Fecal-oral | Parenteral, sexual | Parenteral, sexual | Parenteral, sexual | Fecal-oral |
| Onset | Abrupt | Insidious | Insidious | Variable | Abrupt |
| Incubation | 15-50 days | 45-160 days | 14-180+ days | 15-64 days | 15-50 days |
| Chronicity | None | 10% adults; >90% neonates | 70-85% | 50-80% | Rare |
| Carrier state | No | Yes | Yes | Yes | No |
| HCC risk | No | Yes | Yes | Yes | No |
| Mortality | <0.5% | 1-2% | ~4% | High | Normal: 1-2%; Pregnant: 20% |
| Vaccine available | Yes | Yes | No | (HBV vaccine protects) | No (limited) |
- Medical Microbiology 9e, Table 55.1
1. Hepatitis A Virus (HAV)
Classification
- Family: Picornaviridae, Genus: Hepatovirus
- Formerly called Enterovirus 72
Structure
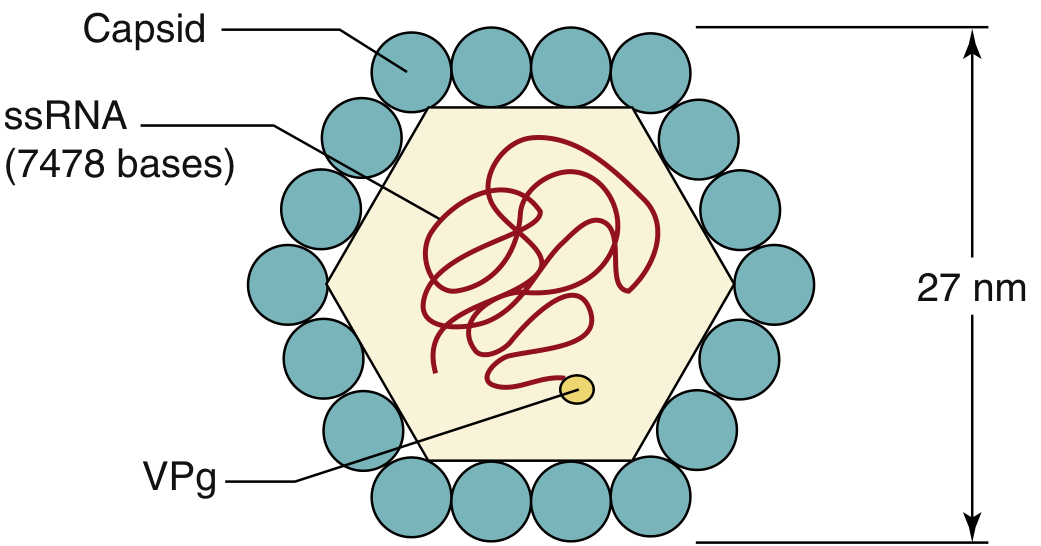
- 27 nm, naked icosahedral capsid
- Positive-sense ssRNA genome (~7,470 nucleotides)
- VPg protein on 5' end; polyadenylate tail on 3' end
- Only one serotype but multiple genotypes
- Capsid is extremely stable - resistant to acid (pH 1), ether, chloroform, detergents, salt water, and drying
- Inactivated by: chlorine in drinking water, formalin, UV radiation
- Medical Microbiology 9e, p. 619
Transmission & Pathogenesis
- Fecal-oral route - contaminated water, shellfish, food
- Enters via gut, replicates in hepatocytes
- Unlike other picornaviruses, HAV is not cytolytic - damage is immune-mediated
- Released by exocytosis
- Receptor: HAVCR-1 (TIM-1) glycoprotein on liver cells and T cells
Clinical Features
- Incubation: 15-50 days (mean 25 days)
- Sudden onset: fever, malaise, anorexia → nausea, vomiting, RUQ pain → jaundice, dark urine, pale stools
- Disease is usually mild and self-limiting
- No chronicity, no carrier state
- Mortality <0.5%
- Severity worse in adults; often subclinical in children
Diagnosis
- Anti-HAV IgM - acute infection
- Anti-HAV IgG - past infection / immunity
Treatment & Prevention
- Supportive treatment only
- Pre-exposure prophylaxis: inactivated HAV vaccine (two doses)
- Post-exposure prophylaxis: immune serum globulin (ISG) within 2 weeks
2. Hepatitis B Virus (HBV)
Classification
- Family: Hepadnaviridae
- The complete virion is called the Dane particle (42 nm)
Structure
- 42 nm enveloped particle
- Outer envelope contains HBsAg (hepatitis B surface antigen)
- 27 nm nucleocapsid core contains:
- HBcAg (hepatitis B core antigen)
- HBeAg (hepatitis B e antigen) - secreted form, marker of active replication
- Partially double-stranded DNA (~3,200 nucleotides) - smallest known DNA virus genome
- DNA polymerase with reverse transcriptase activity
- Three morphological forms in blood:
- 42 nm Dane particles (complete virions)
- 22 nm spherical particles (excess HBsAg - non-infectious)
- Filamentous forms (excess HBsAg - non-infectious)
Replication (Unique Feature)
Transmission
- Parenteral: blood, blood products, needle-sharing (IV drug use)
- Sexual: semen, vaginal secretions
- Vertical: mother-to-child at birth (perinatal transmission - highest risk for chronicity)
- NOT by fecal-oral route
High-Risk Groups
- IV drug users
- Healthcare workers (needle-stick injuries)
- People with multiple sexual partners
- Neonates of HBsAg-positive mothers
- Hemodialysis patients
- People from endemic regions (China, parts of Africa, Alaska, Pacific Islands)
Pathogenesis
- Immune-mediated damage, not direct cytopathic effect
- Cytotoxic CD8+ T cells kill infected hepatocytes
- Serum-sickness-like prodrome (rash, arthritis) from circulating immune complexes (HBsAg-anti-HBs complexes) that activate complement
- Immune complex deposition in kidneys → glomerulonephritis
- Extrahepatic: polyarteritis nodosa, glomerulonephritis
Clinical Outcomes
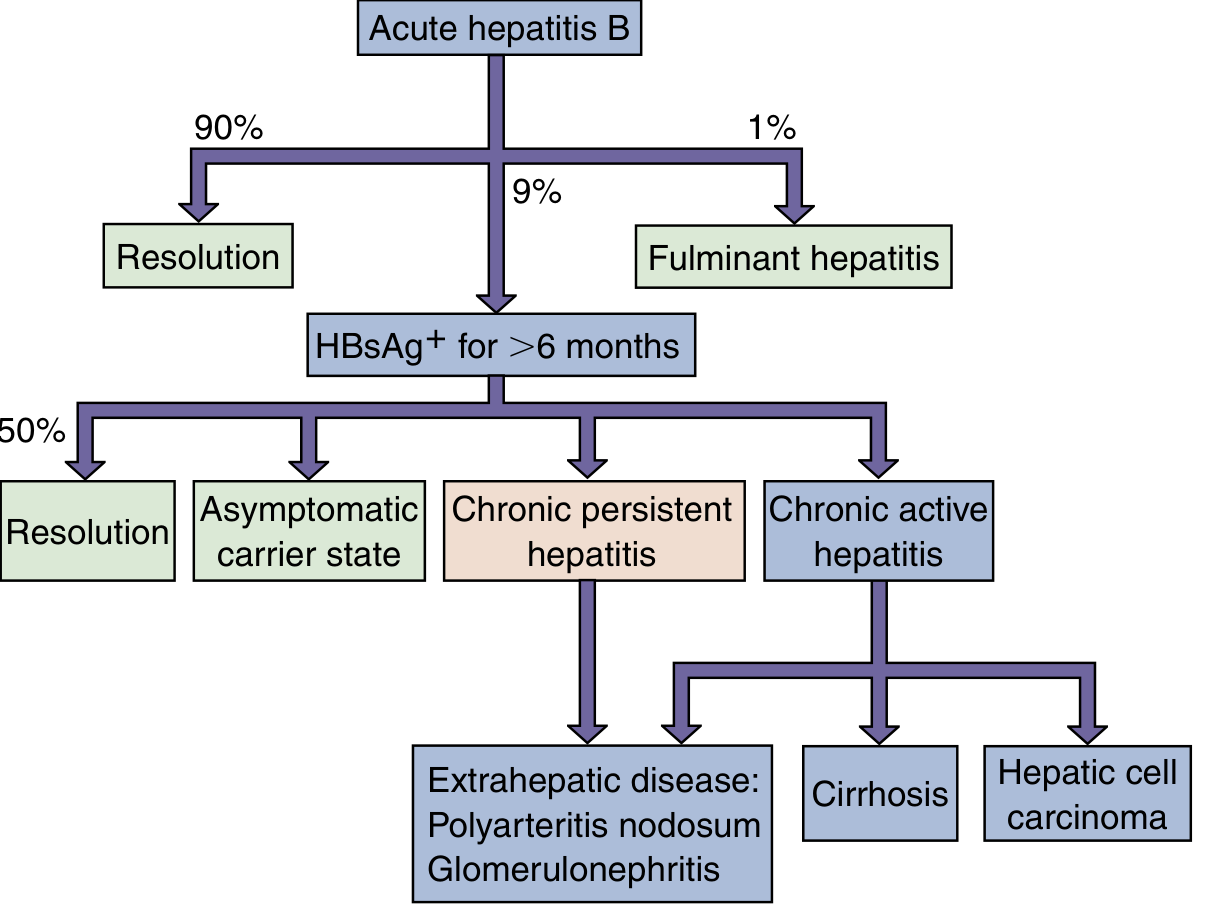
- Incubation: 45-160 days (mean 90 days)
- 90% resolve completely
- 9% → chronic infection (HBsAg+ >6 months)
- Asymptomatic carrier state
- Chronic persistent hepatitis
- Chronic active hepatitis → cirrhosis / hepatocellular carcinoma (HCC)
- Extrahepatic disease (polyarteritis nodosa, glomerulonephritis)
- 1% → fulminant hepatitis (high mortality)
- Neonatal infection: >90% chronicity
Serological Markers - Key for Diagnosis
| Marker | Meaning |
|---|---|
| HBsAg | Active infection (surface antigen) |
| Anti-HBs | Immunity (recovery or vaccination) |
| HBeAg | Active replication, high infectivity |
| Anti-HBe | Declining replication, lower infectivity |
| Anti-HBc IgM | Acute infection ("window period" marker) |
| Anti-HBc IgG | Past infection |
| HBV DNA | Viral load, confirms active replication |
- Window period: HBsAg disappears but anti-HBs not yet detectable - only anti-HBc IgM is positive
- Sherris & Ryan's, p. 489-490
Treatment
- Acute: supportive
- Chronic:
- Alpha-interferon (pegylated)
- Reverse transcriptase inhibitors: lamivudine, tenofovir, entecavir, adefovir
Prevention
- Recombinant HBsAg vaccine (subunit vaccine)
- Infants: at birth, 1 month, 6 months
- Provides long-term protection
- Anti-HBs >10 mIU/mL = protective
- HBIG (Hepatitis B immunoglobulin): post-exposure prophylaxis (e.g., needle-stick, neonate of HBsAg+ mother)
3. Hepatitis C Virus (HCV)
Classification
- Family: Flaviviridae, Genus: Hepacivirus
- Formerly called "non-A, non-B post-transfusion hepatitis"
Structure
- Enveloped virus with positive-sense ssRNA genome (~9,600 nucleotides)
- Highly variable envelope glycoproteins (E1, E2) → responsible for immune evasion
- 6 major genotypes (1-6) with multiple subtypes - genotype 1 is most common worldwide and less responsive to older interferon therapy
Transmission
- Predominantly parenteral: IV drug use, blood transfusions (before 1992 screening), needle-stick
- Sexual transmission (less efficient than HBV)
- Vertical transmission (uncommon)
Pathogenesis
- Both direct cytopathic effects AND immune-mediated damage
- High mutation rate → viral quasispecies → escapes immune surveillance → chronicity
- 70-85% of acute HCV infections become chronic
Clinical Features
- Incubation: 14-180 days (mean 14-84 days)
- Acute infection: usually subclinical/asymptomatic (70% have no symptoms)
- Chronic infection: slowly progressive liver damage
- Complications: cirrhosis (20% over 20 years), hepatocellular carcinoma
- Extrahepatic: mixed cryoglobulinemia, membranoproliferative glomerulonephritis, porphyria cutanea tarda
Diagnosis
- Anti-HCV ELISA (screening)
- HCV RNA by PCR (confirmatory, quantitative)
- HCV genotyping (guides treatment duration)
Treatment
- Old: pegylated interferon + ribavirin (poor response, many side effects)
- Current (DAAs - Direct-Acting Antivirals): sofosbuvir, ledipasvir, daclatasvir, velpatasvir - >95% cure rates with 8-12 week courses
- No vaccine available
4. Hepatitis D Virus (HDV) - The Delta Agent
Classification
- Satellite virus - defective, cannot replicate independently
- Requires HBV co-infection (needs HBsAg as its envelope)
- Viroid-like particle; belongs to genus Deltavirus
Structure
- 35-37 nm enveloped particle
- Negative-sense, circular ssRNA (~1,700 nucleotides) - smallest RNA virus of humans
- Contains HDAg (hepatitis D antigen) inside
- Outer envelope: HBsAg (borrowed from HBV)
Transmission
- Same as HBV: parenteral, sexual, vertical
- Two patterns:
- Co-infection: HBV and HDV acquired simultaneously - usually resolves but more severe acute disease
- Superinfection: HDV acquired in a chronic HBV carrier - severe, often leads to fulminant hepatitis; >50-80% chronicity
Clinical Features
- Incubation: 15-64 days
- Co-infection: bimodal rise in transaminases (two peaks - one for each virus)
- Superinfection: rapid deterioration, high risk of fulminant hepatitis and cirrhosis
- Mortality: high to very high
Diagnosis
- Anti-HDV ELISA (IgM = acute; IgG = past/chronic)
- HDAg detection in serum
Prevention
- HBV vaccination prevents HDV (no HBV = no HDV)
- HBIG post-exposure for HBV also protects against HDV
5. Hepatitis E Virus (HEV)
Classification
- Family: Hepeviridae, Genus: Orthohepevirus
- Formerly called "enteric non-A, non-B hepatitis"
Structure
- 27-34 nm naked, icosahedral capsid
- Positive-sense ssRNA (~7,200 nucleotides)
- Similar appearance to HAV but genetically distinct
Transmission
- Fecal-oral route - contaminated water (major route)
- Common in endemic regions: South Asia (India, Pakistan, Bangladesh), Central Asia, Africa, Mexico
- Waterborne outbreaks in resource-limited settings
- Zoonotic potential: genotype 3/4 from pigs (in developed countries)
Clinical Features
- Incubation: 15-50 days (mean 40 days)
- Clinically similar to HAV - acute, self-limiting
- No chronicity in immunocompetent patients; no carrier state
- Special danger in pregnancy:
- Mortality 20% in pregnant women (especially 3rd trimester)
- Can cause fulminant hepatic failure
- Can cause chronic infection in immunocompromised patients (transplant recipients)
Diagnosis
- Anti-HEV IgM (acute)
- HEV RNA by PCR (in immunocompromised)
Prevention
- No licensed vaccine widely available (a vaccine approved in China)
- Safe water supply, good sanitation
- ISG is NOT protective (unlike HAV)
6. Hepatitis G Virus (HGV) / GBV-C
- A flavivirus related to HCV
- Identified in some blood donors and in patients co-infected with HCV or HIV
- Not associated with any clinical hepatic disease so far
- No standard treatment or vaccine
- May actually have a protective effect against HIV progression (studied but not conclusive)
Summary: Key Distinguishing Points for Exams
| Point | Detail |
|---|---|
| Only DNA hepatitis virus | HBV |
| Fecal-oral viruses | HAV and HEV |
| No carrier state | HAV and HEV |
| Worst in pregnancy | HEV (20% mortality) |
| Needs HBV to replicate | HDV |
| Highest chronicity rate | HCV (70-85%) |
| Smallest human DNA virus | HBV (~3,200 bp) |
| Vaccine available | HAV, HBV (HDV protected by HBV vaccine) |
| Uses reverse transcriptase | HBV |
| Bimodal transaminase peaks | HDV co-infection with HBV |
| Serum sickness-like prodrome | HBV (immune complex disease) |
| Mixed cryoglobulinemia | HCV |
| Window period marker | Anti-HBc IgM |
| Protective antibody in HBV | Anti-HBs |
Create a reference guide PDF summarizing all hepatitis serological markers and their interpretations
ls -la /home/daytona/workspace/
mkdir -p /home/daytona/workspace/hepatitis-guide
~/hepatitis-guide/generate_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import cm, mm
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, KeepTogether
)
from reportlab.lib.enums import TA_CENTER, TA_LEFT, TA_JUSTIFY
from reportlab.platypus import PageBreak
OUTPUT = "/home/daytona/workspace/hepatitis-guide/Hepatitis_Serological_Markers_Reference.pdf"
# ── Colour palette ────────────────────────────────────────────────────────────
NAVY = colors.HexColor("#1A3557")
TEAL = colors.HexColor("#1B7A8C")
LIGHT_TEAL = colors.HexColor("#D6EEF2")
AMBER = colors.HexColor("#E8A020")
LIGHT_AMBER = colors.HexColor("#FFF3D6")
RED = colors.HexColor("#C0392B")
GREEN = colors.HexColor("#1A7A4A")
LIGHT_GREEN = colors.HexColor("#D6F0E3")
LIGHT_GREY = colors.HexColor("#F4F6F8")
MID_GREY = colors.HexColor("#BDC3C7")
WHITE = colors.white
DARK_TEXT = colors.HexColor("#1C1C1E")
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
leftMargin=1.8*cm, rightMargin=1.8*cm,
topMargin=2*cm, bottomMargin=2*cm,
title="Hepatitis Serological Markers – Reference Guide",
author="Orris Medical Reference"
)
styles = getSampleStyleSheet()
# Custom styles
def S(name, parent="Normal", **kwargs):
return ParagraphStyle(name, parent=styles[parent], **kwargs)
title_style = S("MyTitle", fontSize=22, textColor=WHITE, alignment=TA_CENTER, fontName="Helvetica-Bold", leading=28, spaceAfter=4)
sub_style = S("MySub", fontSize=11, textColor=LIGHT_TEAL, alignment=TA_CENTER, fontName="Helvetica", leading=15, spaceAfter=2)
h1_style = S("MyH1", fontSize=13, textColor=WHITE, fontName="Helvetica-Bold", leading=18, spaceBefore=4, spaceAfter=2)
h2_style = S("MyH2", fontSize=11, textColor=NAVY, fontName="Helvetica-Bold", leading=15, spaceBefore=8, spaceAfter=3)
body_style = S("MyBody", fontSize=9, textColor=DARK_TEXT, fontName="Helvetica", leading=13, spaceBefore=2, spaceAfter=2, alignment=TA_JUSTIFY)
note_style = S("MyNote", fontSize=8, textColor=colors.HexColor("#555555"), fontName="Helvetica-Oblique", leading=11, spaceBefore=2, spaceAfter=2)
footer_style = S("MyFooter", fontSize=7.5, textColor=MID_GREY, alignment=TA_CENTER, fontName="Helvetica-Oblique")
cell_hdr = S("CellHdr", fontSize=8.5, textColor=WHITE, fontName="Helvetica-Bold", leading=11, alignment=TA_CENTER)
cell_body = S("CellBody", fontSize=8, textColor=DARK_TEXT, fontName="Helvetica", leading=11, alignment=TA_LEFT)
cell_center = S("CellCtr", fontSize=8, textColor=DARK_TEXT, fontName="Helvetica", leading=11, alignment=TA_CENTER)
pos_style = S("Pos", fontSize=8, textColor=GREEN, fontName="Helvetica-Bold", leading=11, alignment=TA_CENTER)
neg_style = S("Neg", fontSize=8, textColor=RED, fontName="Helvetica-Bold", leading=11, alignment=TA_CENTER)
interp_style = S("Interp", fontSize=8, textColor=NAVY, fontName="Helvetica-Bold", leading=11, alignment=TA_CENTER)
warn_style = S("Warn", fontSize=8, textColor=RED, fontName="Helvetica-Bold", leading=11, alignment=TA_CENTER)
story = []
# ═══════════════════════════════════════════════════════════════════════════════
# HEADER BANNER
# ═══════════════════════════════════════════════════════════════════════════════
banner_data = [[Paragraph("Hepatitis Serological Markers", title_style)],
[Paragraph("Complete Reference Guide for Interpretation", sub_style)],
[Paragraph("Based on Ananthanarayan Microbiology & Medical Microbiology 9e (Murray et al.)", note_style)]]
banner_table = Table(banner_data, colWidths=[17.4*cm])
banner_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), NAVY),
("TOPPADDING", (0,0), (-1,-1), 10),
("BOTTOMPADDING",(0,0), (-1,-1), 10),
("LEFTPADDING", (0,0), (-1,-1), 16),
("RIGHTPADDING", (0,0), (-1,-1), 16),
("ROUNDEDCORNERS", [6]),
]))
story.append(banner_table)
story.append(Spacer(1, 0.4*cm))
# ═══════════════════════════════════════════════════════════════════════════════
# QUICK INTRO
# ═══════════════════════════════════════════════════════════════════════════════
story.append(Paragraph(
"Serological testing is the cornerstone of diagnosing viral hepatitis. Each virus generates a characteristic pattern "
"of antigens and antibodies over time. This guide covers HBV (most complex), HAV, HCV, HDV, and HEV markers, "
"their clinical significance, and interpretation patterns for common clinical scenarios.",
body_style))
story.append(Spacer(1, 0.3*cm))
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 1 – HEPATITIS B (most detailed)
# ═══════════════════════════════════════════════════════════════════════════════
def section_header(text, color=NAVY):
data = [[Paragraph(text, h1_style)]]
t = Table(data, colWidths=[17.4*cm])
t.setStyle(TableStyle([
("BACKGROUND", (0,0),(-1,-1), color),
("TOPPADDING", (0,0),(-1,-1), 7),
("BOTTOMPADDING", (0,0),(-1,-1), 7),
("LEFTPADDING", (0,0),(-1,-1), 12),
("ROUNDEDCORNERS",[4]),
]))
return t
story.append(section_header("SECTION 1 — Hepatitis B Virus (HBV) Markers"))
story.append(Spacer(1, 0.25*cm))
story.append(Paragraph(
"HBV serology is the most complex among hepatitis viruses. Three antigen-antibody systems are clinically relevant: "
"HBsAg/anti-HBs (surface), HBcAg/anti-HBc (core), and HBeAg/anti-HBe (e-antigen). "
"HBcAg is NOT detectable in serum (only intracellularly), so only anti-HBc is measured clinically.",
body_style))
story.append(Spacer(1, 0.2*cm))
# ── Individual markers table ───────────────────────────────────────────────────
story.append(Paragraph("1.1 Individual Marker Reference", h2_style))
hbv_markers_header = [
Paragraph("Marker", cell_hdr),
Paragraph("What It Is", cell_hdr),
Paragraph("When Present", cell_hdr),
Paragraph("Clinical Significance", cell_hdr),
]
hbv_markers = [
["HBsAg\n(Hepatitis B Surface Antigen)",
"Outer envelope protein of HBV",
"Acute infection; persists >6 months in chronic infection",
"FIRST marker to appear (2–10 wks post-exposure). Defines active infection. Persistence >6 months = chronic HBV. Used for blood bank screening."],
["Anti-HBs\n(Antibody to HBsAg)",
"Neutralizing antibody against HBsAg",
"After resolution of acute infection OR after vaccination",
"PROTECTIVE antibody. Titre >10 mIU/mL = immune. ONLY marker positive after vaccination (anti-HBc negative). Indicates recovery and non-infectivity."],
["HBcAg\n(Core Antigen)",
"Nucleocapsid core protein",
"Only inside hepatocytes (NOT in serum)",
"NOT detectable in serum. Seen only on liver biopsy immunostaining. DO NOT order serum HBcAg."],
["Anti-HBc IgM\n(IgM to Core Antigen)",
"IgM antibody to nucleocapsid",
"Acute infection (first 6 months)",
"MARKER OF ACUTE INFECTION. Critical during the WINDOW PERIOD (when HBsAg has cleared but anti-HBs not yet detectable). High titre = acute; low titre = reactivation."],
["Anti-HBc IgG\n(IgG to Core Antigen)",
"IgG antibody to nucleocapsid",
"Persists lifelong after infection (acute or chronic)",
"Indicates past or current HBV exposure. Present in all: acute, chronic, and resolved infection. NOT present after vaccination alone."],
["Anti-HBc Total\n(IgM + IgG)",
"Combined anti-HBc assay",
"Any time after exposure to HBV",
"Used in blood banks. Positive = HBV exposure at some point. Differentiates vaccination (anti-HBs only) from natural infection (anti-HBc + anti-HBs)."],
["HBeAg\n(Hepatitis B e Antigen)",
"Secreted peptide derived from precore region",
"Active viral replication phase",
"Marker of HIGH INFECTIVITY and active replication. Correlates with high viral load (HBV DNA). Important for treatment decisions."],
["Anti-HBe\n(Antibody to HBeAg)",
"Antibody to e-antigen",
"After HBeAg seroconversion (recovery or treatment response)",
"Indicates DECLINING viral replication. Associated with lower infectivity. Seroconversion (HBeAg → anti-HBe) is a key treatment endpoint."],
["HBV DNA\n(Viral Load)",
"Quantitative PCR of HBV genome",
"Active infection / replication",
"Gold standard for viral replication. Guides treatment initiation (>2,000 IU/mL in HBeAg-negative chronic hepatitis). Monitors antiviral therapy response."],
["HBsAg Quantitative",
"Quantitative HBsAg level",
"Active infection",
"Predicts functional cure likelihood. Declining levels suggest immune control. <100 IU/mL with HBV DNA undetectable associated with HBsAg loss."],
]
col_widths = [3.5*cm, 3*cm, 3.2*cm, 7.7*cm]
row_data = [hbv_markers_header]
for r in hbv_markers:
row_data.append([
Paragraph(r[0], cell_body),
Paragraph(r[1], cell_body),
Paragraph(r[2], cell_body),
Paragraph(r[3], cell_body),
])
marker_table = Table(row_data, colWidths=col_widths, repeatRows=1)
marker_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), TEAL),
("BACKGROUND", (0,1), (-1,1), LIGHT_TEAL),
("BACKGROUND", (0,2), (-1,2), WHITE),
("BACKGROUND", (0,3), (-1,3), LIGHT_TEAL),
("BACKGROUND", (0,4), (-1,4), WHITE),
("BACKGROUND", (0,5), (-1,5), LIGHT_TEAL),
("BACKGROUND", (0,6), (-1,6), WHITE),
("BACKGROUND", (0,7), (-1,7), LIGHT_TEAL),
("BACKGROUND", (0,8), (-1,8), WHITE),
("BACKGROUND", (0,9), (-1,9), LIGHT_TEAL),
("BACKGROUND", (0,10), (-1,10), WHITE),
("GRID", (0,0), (-1,-1), 0.4, MID_GREY),
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 5),
("RIGHTPADDING", (0,0), (-1,-1), 5),
]))
story.append(marker_table)
story.append(Spacer(1, 0.4*cm))
# ── HBV Interpretation Patterns ───────────────────────────────────────────────
story.append(Paragraph("1.2 HBV Serological Pattern Interpretation", h2_style))
interp_hdr = [
Paragraph("HBsAg", cell_hdr),
Paragraph("Anti-HBs", cell_hdr),
Paragraph("Anti-HBc IgM", cell_hdr),
Paragraph("Anti-HBc IgG", cell_hdr),
Paragraph("HBeAg", cell_hdr),
Paragraph("Anti-HBe", cell_hdr),
Paragraph("HBV DNA", cell_hdr),
Paragraph("Interpretation", cell_hdr),
]
# +/- colour helper
def P(text, style=None):
if text == "+":
return Paragraph(text, pos_style)
elif text == "−":
return Paragraph(text, neg_style)
elif style:
return Paragraph(text, style)
else:
return Paragraph(text, cell_center)
interp_rows = [
["+", "−", "+", "+/−", "+", "−", "High", "Acute HBV infection (early)"],
["+", "−", "+", "+", "−", "+", "Low/−", "Acute HBV – resolving (late acute)"],
["−", "−", "+", "+", "−", "+/−","Low/−", "Window period (acute HBV) – critical!"],
["−", "+", "−", "+", "−", "+/−","−", "Past HBV infection – fully resolved"],
["−", "+", "−", "−", "−", "−", "−", "Vaccinated (immune) – no prior infection"],
["+", "−", "−", "+", "+", "−", "High", "Chronic HBV – immune active (HBeAg+)"],
["+", "−", "−", "+", "−", "+", "Low–mod", "Chronic HBV – immune control (HBeAg−)"],
["+", "−", "−", "+", "−", "+", "High", "Chronic HBV – HBeAg-negative hepatitis"],
["+", "+", "−", "+", "+/−","−/+","Var", "Rare co-existing or unusual pattern – retest"],
["−", "+", "+", "+", "−", "+/−","Low", "Acute HBV resolving (early seroconversion)"],
]
interp_col_w = [1.6*cm, 1.6*cm, 2*cm, 2*cm, 1.6*cm, 1.6*cm, 1.8*cm, 5.2*cm]
interp_data = [interp_hdr]
for i, row in enumerate(interp_rows):
bg_color = LIGHT_AMBER if "Window" in row[-1] else (LIGHT_GREEN if "Vaccinated" in row[-1] or "resolved" in row[-1] else (LIGHT_GREY if i % 2 == 0 else WHITE))
interp_data.append([P(row[0]), P(row[1]), P(row[2]), P(row[3]), P(row[4]), P(row[5]),
Paragraph(row[6], cell_center),
Paragraph(row[7], interp_style if "Window" in row[-1] else cell_body)])
interp_table = Table(interp_data, colWidths=interp_col_w, repeatRows=1)
interp_style_ts = TableStyle([
("BACKGROUND", (0,0), (-1,0), NAVY),
("GRID", (0,0), (-1,-1), 0.4, MID_GREY),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 4),
("RIGHTPADDING", (0,0), (-1,-1), 4),
("BACKGROUND", (0,1), (-1,1), LIGHT_GREY),
("BACKGROUND", (0,2), (-1,2), WHITE),
("BACKGROUND", (0,3), (-1,3), LIGHT_AMBER), # window period
("BACKGROUND", (0,4), (-1,4), WHITE),
("BACKGROUND", (0,5), (-1,5), LIGHT_GREEN), # vaccinated
("BACKGROUND", (0,6), (-1,6), LIGHT_GREY),
("BACKGROUND", (0,7), (-1,7), LIGHT_GREY),
("BACKGROUND", (0,8), (-1,8), WHITE),
("BACKGROUND", (0,9), (-1,9), LIGHT_GREY),
("BACKGROUND", (0,10), (-1,10), WHITE),
# Highlight window period row
("FONTNAME", (0,3), (-1,3), "Helvetica-Bold"),
("TEXTCOLOR", (7,3), (7,3), RED),
])
interp_table.setStyle(interp_style_ts)
story.append(interp_table)
story.append(Spacer(1, 0.2*cm))
story.append(Paragraph(
"⚠ Window Period: HBsAg has cleared but anti-HBs not yet detectable. "
"Only Anti-HBc IgM is positive. Do NOT report as 'not infected' — order HBV DNA to confirm.",
note_style))
story.append(Spacer(1, 0.3*cm))
# ── HBV timeline note ─────────────────────────────────────────────────────────
story.append(Paragraph("1.3 Temporal Sequence of HBV Markers", h2_style))
timeline_data = [
[Paragraph("Phase", cell_hdr), Paragraph("Weeks Post-Exposure", cell_hdr),
Paragraph("Key Markers Present", cell_hdr), Paragraph("Key Markers Absent", cell_hdr)],
[Paragraph("Incubation", cell_body), Paragraph("2–10 weeks", cell_center),
Paragraph("HBsAg (rises), HBeAg, HBV DNA (high)", cell_body),
Paragraph("Anti-HBs, Anti-HBc", cell_body)],
[Paragraph("Acute symptomatic", cell_body), Paragraph("10–16 weeks", cell_center),
Paragraph("HBsAg, HBeAg, HBV DNA, Anti-HBc IgM, ALT elevated", cell_body),
Paragraph("Anti-HBs, Anti-HBe", cell_body)],
[Paragraph("Window period", cell_body), Paragraph("16–24 weeks", cell_center),
Paragraph("Anti-HBc IgM ✦ (only reliable marker), Anti-HBc IgG", cell_body),
Paragraph("HBsAg (cleared), Anti-HBs (not yet)", cell_body)],
[Paragraph("Recovery", cell_body), Paragraph(">24 weeks", cell_center),
Paragraph("Anti-HBs, Anti-HBc IgG, Anti-HBe", cell_body),
Paragraph("HBsAg, HBeAg, HBV DNA, Anti-HBc IgM", cell_body)],
[Paragraph("Chronic (>6 months)", cell_body), Paragraph(">26 weeks with HBsAg", cell_center),
Paragraph("HBsAg, HBV DNA, Anti-HBc IgG; ± HBeAg", cell_body),
Paragraph("Anti-HBs", cell_body)],
]
tl_table = Table(timeline_data, colWidths=[3*cm, 3.5*cm, 5.7*cm, 5.2*cm], repeatRows=1)
tl_table.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), TEAL),
("BACKGROUND", (0,3), (-1,3), LIGHT_AMBER),
("FONTNAME", (0,3), (-1,3), "Helvetica-Bold"),
("GRID", (0,0), (-1,-1), 0.4, MID_GREY),
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 5),
("ROWBACKGROUNDS",(0,1), (-1,-1), [LIGHT_GREY, WHITE]),
("BACKGROUND", (0,3), (-1,3), LIGHT_AMBER),
]))
story.append(tl_table)
story.append(Spacer(1, 0.4*cm))
# ═══════════════════════════════════════════════════════════════════════════════
# PAGE BREAK + SECTION 2 – HEPATITIS A
# ═══════════════════════════════════════════════════════════════════════════════
story.append(PageBreak())
story.append(section_header("SECTION 2 — Hepatitis A Virus (HAV) Markers", TEAL))
story.append(Spacer(1, 0.25*cm))
story.append(Paragraph(
"HAV serology is relatively straightforward. There are only two clinically relevant markers: Anti-HAV IgM and Anti-HAV IgG. "
"There is no antigen test used routinely. No chronic infection occurs so no carrier-state monitoring is needed.",
body_style))
story.append(Spacer(1, 0.2*cm))
hav_data = [
[Paragraph("Marker", cell_hdr), Paragraph("When Detectable", cell_hdr),
Paragraph("Duration", cell_hdr), Paragraph("Clinical Interpretation", cell_hdr)],
[Paragraph("Anti-HAV IgM", cell_body),
Paragraph("5–10 days before symptom onset; peaks at 1 month", cell_body),
Paragraph("Positive for 3–6 months", cell_body),
Paragraph("ACUTE HAV infection. Diagnostic of current/recent infection. "
"IgM is the primary confirmatory test. Do NOT diagnose acute HAV without IgM.", cell_body)],
[Paragraph("Anti-HAV IgG\n(Total Anti-HAV)", cell_body),
Paragraph("Appears after IgM; rises as IgM falls", cell_body),
Paragraph("Lifelong persistence", cell_body),
Paragraph("Past infection or prior vaccination. Indicates IMMUNITY to HAV. "
"Present in ~45% of adults >50 years in endemic regions.", cell_body)],
[Paragraph("HAV RNA (PCR)", cell_body),
Paragraph("Viraemic phase (before/during symptoms)", cell_body),
Paragraph("Clears with resolution", cell_body),
Paragraph("Used in research/outbreak investigations. Not routinely ordered clinically. "
"Confirms viraemia in atypical or immunocompromised cases.", cell_body)],
]
hav_t = Table(hav_data, colWidths=[3.5*cm, 3.8*cm, 3.3*cm, 6.8*cm], repeatRows=1)
hav_t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), TEAL),
("ROWBACKGROUNDS",(0,1), (-1,-1), [LIGHT_TEAL, WHITE, LIGHT_TEAL]),
("GRID", (0,0), (-1,-1), 0.4, MID_GREY),
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 5),
]))
story.append(hav_t)
story.append(Spacer(1, 0.25*cm))
hav_interp = [
[Paragraph("Anti-HAV IgM", cell_hdr), Paragraph("Anti-HAV IgG", cell_hdr), Paragraph("Interpretation", cell_hdr)],
[P("+"), P("−"), Paragraph("Early acute HAV infection", cell_body)],
[P("+"), P("+"), Paragraph("Acute HAV infection (IgG appearing)", cell_body)],
[P("−"), P("+"), Paragraph("Past infection or vaccinated — immune", cell_body)],
[P("−"), P("−"), Paragraph("Susceptible — no prior exposure, not vaccinated", cell_body)],
]
hav_i_t = Table(hav_interp, colWidths=[4*cm, 4*cm, 9.4*cm], repeatRows=1)
hav_i_t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), NAVY),
("ROWBACKGROUNDS",(0,1),(-1,-1), [LIGHT_GREY, WHITE, LIGHT_GREEN, LIGHT_AMBER]),
("GRID", (0,0), (-1,-1), 0.4, MID_GREY),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 5),
]))
story.append(Paragraph("HAV Interpretation Patterns", h2_style))
story.append(hav_i_t)
story.append(Spacer(1, 0.4*cm))
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 3 – HEPATITIS C
# ═══════════════════════════════════════════════════════════════════════════════
story.append(section_header("SECTION 3 — Hepatitis C Virus (HCV) Markers", colors.HexColor("#2E6B8A")))
story.append(Spacer(1, 0.25*cm))
story.append(Paragraph(
"HCV testing follows a two-step algorithm: screen with Anti-HCV antibody, then confirm with HCV RNA (PCR). "
"A positive antibody alone does NOT mean active infection — antibody persists lifelong after resolution. "
"HCV RNA is the definitive marker of active viraemia.",
body_style))
story.append(Spacer(1, 0.2*cm))
hcv_markers = [
[Paragraph("Marker", cell_hdr), Paragraph("Method", cell_hdr),
Paragraph("Clinical Role", cell_hdr), Paragraph("Interpretation", cell_hdr)],
[Paragraph("Anti-HCV\n(Total antibody)", cell_body),
Paragraph("ELISA / CMIA\n(3rd/4th gen)", cell_body),
Paragraph("Screening", cell_body),
Paragraph("Detectable 8–11 weeks post-exposure. Persists lifelong — does NOT distinguish acute, chronic, or resolved. "
"Reactive result MUST be confirmed by HCV RNA.", cell_body)],
[Paragraph("HCV RNA\n(Qualitative PCR)", cell_body),
Paragraph("RT-PCR (NAAT)", cell_body),
Paragraph("Confirmation of viraemia", cell_body),
Paragraph("Detectable within 1–2 weeks of exposure (before antibody). Positive = active HCV infection. "
"Negative + positive anti-HCV = resolved infection.", cell_body)],
[Paragraph("HCV RNA\n(Quantitative — viral load)", cell_body),
Paragraph("Real-time PCR\n(IU/mL)", cell_body),
Paragraph("Baseline, treatment monitoring", cell_body),
Paragraph("Pre-treatment baseline. Assessed at weeks 4, 12 of therapy. Undetectable at week 12 = early virological response (EVR). "
"Undetectable 12 weeks post-treatment = SVR12 (cure).", cell_body)],
[Paragraph("HCV Genotype\n(1–6)", cell_body),
Paragraph("Sequencing / LiPA", cell_body),
Paragraph("Treatment selection", cell_body),
Paragraph("Genotype 1 (most common globally, less responsive to old IFN therapy). "
"Genotype 3 (associated with faster fibrosis progression, steatosis). "
"Guides DAA regimen choice and duration.", cell_body)],
[Paragraph("HCV Core Antigen\n(HCVcAg)", cell_body),
Paragraph("ELISA", cell_body),
Paragraph("Alternative to RNA", cell_body),
Paragraph("Detectable during viraemia. Can substitute for RNA testing in resource-limited settings. "
"Undetectable in resolved infection.", cell_body)],
[Paragraph("Liver Fibrosis Tests\n(FIB-4, APRI, FibroScan)", cell_body),
Paragraph("Blood tests / elastography", cell_body),
Paragraph("Staging", cell_body),
Paragraph("Not direct HCV serology but essential in chronic HCV to assess fibrosis stage (F0–F4). "
"FibroScan (liver stiffness >12.5 kPa = cirrhosis). Guides treatment urgency.", cell_body)],
]
hcv_t = Table(hcv_markers, colWidths=[3.3*cm, 2.8*cm, 3.2*cm, 8.1*cm], repeatRows=1)
hcv_t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), colors.HexColor("#2E6B8A")),
("ROWBACKGROUNDS",(0,1), (-1,-1), [LIGHT_TEAL, WHITE, LIGHT_TEAL, WHITE, LIGHT_TEAL, WHITE]),
("GRID", (0,0), (-1,-1), 0.4, MID_GREY),
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 5),
]))
story.append(hcv_t)
story.append(Spacer(1, 0.25*cm))
story.append(Paragraph("HCV Testing Algorithm", h2_style))
algo_data = [
[Paragraph("Step 1: Screen with Anti-HCV antibody (ELISA)", cell_body)],
[Paragraph(" ↓ Reactive ↓ Non-reactive", cell_body)],
[Paragraph("Step 2: HCV RNA (NAAT) Report: HCV not detected (if low pre-test probability)", cell_body)],
[Paragraph(" ↓ Detected ↓ Not detected", cell_body)],
[Paragraph("Active HCV infection Resolved past infection (or false+ antibody)", cell_body)],
[Paragraph("Step 3: Genotype + Viral Load → Initiate DAA therapy", cell_body)],
[Paragraph("Step 4: SVR12 check (12 weeks after end of treatment) → Undetectable RNA = CURED", cell_body)],
]
algo_t = Table(algo_data, colWidths=[17.4*cm])
algo_t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), LIGHT_TEAL),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING", (0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 12),
("BOX", (0,0), (-1,-1), 0.8, TEAL),
("FONTNAME", (0,0), (-1,-1), "Helvetica"),
("FONTSIZE", (0,0), (-1,-1), 8.5),
("TEXTCOLOR", (0,0), (-1,-1), DARK_TEXT),
]))
story.append(algo_t)
story.append(Spacer(1, 0.4*cm))
# ═══════════════════════════════════════════════════════════════════════════════
# PAGE BREAK + SECTION 4 – HDV
# ═══════════════════════════════════════════════════════════════════════════════
story.append(PageBreak())
story.append(section_header("SECTION 4 — Hepatitis D Virus (HDV) Markers", colors.HexColor("#6B3A7D")))
story.append(Spacer(1, 0.25*cm))
story.append(Paragraph(
"HDV (the delta agent) is a defective satellite virus that REQUIRES HBV for replication — it uses HBsAg as its envelope. "
"HDV testing is ONLY relevant when HBsAg is positive. Two clinical scenarios: co-infection (HBV+HDV simultaneously) "
"vs. superinfection (HDV in a chronic HBV carrier). Superinfection is far more severe.",
body_style))
story.append(Spacer(1, 0.2*cm))
hdv_markers = [
[Paragraph("Marker", cell_hdr), Paragraph("When Present", cell_hdr),
Paragraph("Clinical Significance", cell_hdr)],
[Paragraph("HDAg (HDV Antigen)", cell_body),
Paragraph("Early acute HDV infection (days 1–3 of symptoms); transient", cell_body),
Paragraph("Earliest detectable marker. Window is narrow — easily missed. "
"Detection confirms active HDV replication.", cell_body)],
[Paragraph("Anti-HDV IgM", cell_body),
Paragraph("Acute co-infection and superinfection", cell_body),
Paragraph("Indicates recent/acute HDV infection. In co-infection, appears transiently. "
"In superinfection, persists longer with progression to chronic HDV.", cell_body)],
[Paragraph("Anti-HDV IgG (Total Anti-HDV)", cell_body),
Paragraph("Chronic HDV or past resolved HDV", cell_body),
Paragraph("Persists in chronic HDV infection. High titre + HBsAg positive = chronic HDV. "
"Low titre after acute co-infection that resolved = past exposure.", cell_body)],
[Paragraph("HDV RNA (PCR)", cell_body),
Paragraph("Active HDV replication", cell_body),
Paragraph("Confirmatory and quantitative. Most sensitive marker. Used for treatment monitoring. "
"Undetectable RNA = goal of HDV-directed therapy (bulevirtide).", cell_body)],
]
hdv_t = Table(hdv_markers, colWidths=[3.8*cm, 5*cm, 8.6*cm], repeatRows=1)
hdv_t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), colors.HexColor("#6B3A7D")),
("ROWBACKGROUNDS",(0,1), (-1,-1), [LIGHT_GREY, WHITE, LIGHT_GREY, WHITE]),
("GRID", (0,0), (-1,-1), 0.4, MID_GREY),
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 5),
]))
story.append(hdv_t)
story.append(Spacer(1, 0.3*cm))
story.append(Paragraph("HDV Co-infection vs. Superinfection — Key Differences", h2_style))
cosuper = [
[Paragraph("Feature", cell_hdr),
Paragraph("Co-infection (HBV + HDV simultaneously)", cell_hdr),
Paragraph("Superinfection (HDV in chronic HBV carrier)", cell_hdr)],
[Paragraph("Definition", cell_body),
Paragraph("Both HBV and HDV acquired at the same time", cell_body),
Paragraph("HDV acquired by someone already chronically infected with HBV", cell_body)],
[Paragraph("HBsAg", cell_body), P("+"), P("+")],
[Paragraph("Anti-HBc IgM", cell_body), P("+"), P("−")],
[Paragraph("Anti-HDV IgM", cell_body), P("+"), P("+")],
[Paragraph("Severity of acute illness", cell_body),
Paragraph("Moderate to severe (bimodal transaminase peaks)", cell_body),
Paragraph("Severe to fulminant", cell_body)],
[Paragraph("Risk of chronicity", cell_body),
Paragraph("Low (~5%) — mirrors HBV co-infection resolution", cell_body),
Paragraph("Very high (>80%) — chronic HDV hepatitis", cell_body)],
[Paragraph("Outcome", cell_body),
Paragraph("Usually self-limiting; fulminant hepatitis possible", cell_body),
Paragraph("Often cirrhosis; high HCC risk", cell_body)],
]
cosuper_t = Table(cosuper, colWidths=[3.5*cm, 6.8*cm, 7.1*cm], repeatRows=1)
cosuper_t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), NAVY),
("BACKGROUND", (0,2), (0,7), LIGHT_GREY),
("ROWBACKGROUNDS",(0,1), (-1,-1), [LIGHT_GREY, WHITE, LIGHT_GREY, WHITE, LIGHT_GREY, WHITE, LIGHT_GREY]),
("BACKGROUND", (0,5), (-1,5), LIGHT_AMBER),
("BACKGROUND", (0,6), (-1,6), colors.HexColor("#FFE4E4")),
("GRID", (0,0), (-1,-1), 0.4, MID_GREY),
("VALIGN", (0,0), (-1,-1), "MIDDLE"),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 5),
]))
story.append(cosuper_t)
story.append(Spacer(1, 0.4*cm))
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 5 – HEV
# ═══════════════════════════════════════════════════════════════════════════════
story.append(section_header("SECTION 5 — Hepatitis E Virus (HEV) Markers", colors.HexColor("#7D5A1A")))
story.append(Spacer(1, 0.25*cm))
story.append(Paragraph(
"HEV is transmitted by the fecal-oral route like HAV. It causes self-limiting acute hepatitis in most patients "
"but carries a 20% mortality in pregnant women. Chronic HEV (genotypes 3/4) can occur in immunocompromised patients. "
"Immune serum globulin does NOT protect against HEV.",
body_style))
story.append(Spacer(1, 0.2*cm))
hev_markers = [
[Paragraph("Marker", cell_hdr), Paragraph("When Present", cell_hdr),
Paragraph("Duration", cell_hdr), Paragraph("Interpretation", cell_hdr)],
[Paragraph("Anti-HEV IgM", cell_body),
Paragraph("Onset of symptoms", cell_body),
Paragraph("1–3 months", cell_body),
Paragraph("Acute HEV infection. Primary diagnostic marker. Must be interpreted with clinical context (false positives in endemic areas). "
"Confirm with HEV RNA if doubt.", cell_body)],
[Paragraph("Anti-HEV IgG", cell_body),
Paragraph("Shortly after IgM", cell_body),
Paragraph("Years; may wane over time", cell_body),
Paragraph("Past infection or immunity. Used in seroprevalence studies. Does NOT guarantee lifelong protection "
"(unlike anti-HAV IgG).", cell_body)],
[Paragraph("HEV RNA (PCR)", cell_body),
Paragraph("1 week before symptoms; during acute phase", cell_body),
Paragraph("Clears in acute; persists in chronic (immunocompromised)", cell_body),
Paragraph("Gold standard — most sensitive. Used in: blood bank screening, immunocompromised patients, "
"monitoring ribavirin therapy, confirming seronegative HEV in organ transplant recipients.", cell_body)],
[Paragraph("HEV Antigen", cell_body),
Paragraph("Acute viraemic phase", cell_body),
Paragraph("Short window", cell_body),
Paragraph("Alternative to PCR in resource-limited settings. Less sensitive than RNA PCR.", cell_body)],
]
hev_t = Table(hev_markers, colWidths=[3.2*cm, 3.2*cm, 3.2*cm, 7.8*cm], repeatRows=1)
hev_t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), colors.HexColor("#7D5A1A")),
("ROWBACKGROUNDS",(0,1), (-1,-1), [LIGHT_AMBER, WHITE, LIGHT_AMBER, WHITE]),
("GRID", (0,0), (-1,-1), 0.4, MID_GREY),
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 5),
]))
story.append(hev_t)
story.append(Spacer(1, 0.25*cm))
story.append(Paragraph(
"Special note: In pregnancy (especially 3rd trimester), HEV can cause fulminant hepatic failure with 20% mortality. "
"HEV RNA should be tested in any pregnant woman with acute hepatitis and epidemiological exposure risk.",
note_style))
story.append(Spacer(1, 0.4*cm))
# ═══════════════════════════════════════════════════════════════════════════════
# PAGE BREAK + SECTION 6 – MASTER COMPARISON
# ═══════════════════════════════════════════════════════════════════════════════
story.append(PageBreak())
story.append(section_header("SECTION 6 — Master Comparison: All Hepatitis Serological Markers", NAVY))
story.append(Spacer(1, 0.25*cm))
master = [
[Paragraph("Virus", cell_hdr), Paragraph("Antigen(s)", cell_hdr),
Paragraph("IgM Antibody", cell_hdr), Paragraph("IgG/Total Antibody", cell_hdr),
Paragraph("Nucleic Acid", cell_hdr), Paragraph("Chronicity Marker", cell_hdr),
Paragraph("Protective Antibody", cell_hdr)],
[Paragraph("HAV", cell_body), Paragraph("None (routine)", cell_body),
Paragraph("Anti-HAV IgM → Acute", cell_body), Paragraph("Anti-HAV IgG → Past/immune", cell_body),
Paragraph("HAV RNA (PCR) – research only", cell_body), Paragraph("None – no chronicity", cell_body),
Paragraph("Anti-HAV IgG", cell_body)],
[Paragraph("HBV", cell_body),
Paragraph("HBsAg (surface)\nHBeAg (e-antigen)", cell_body),
Paragraph("Anti-HBc IgM → Acute (incl. window period)", cell_body),
Paragraph("Anti-HBc IgG → Past/current\nAnti-HBe → Seroconversion", cell_body),
Paragraph("HBV DNA (PCR) – viral load", cell_body),
Paragraph("HBsAg >6 months\nHBV DNA\nHBeAg (if +)", cell_body),
Paragraph("Anti-HBs >10 mIU/mL", cell_body)],
[Paragraph("HCV", cell_body), Paragraph("HCV core Ag (limited use)", cell_body),
Paragraph("Anti-HCV (ELISA) – screen only; IgM not differentiated", cell_body),
Paragraph("Anti-HCV total – persists lifelong; does NOT indicate active infection", cell_body),
Paragraph("HCV RNA (PCR) – confirms active infection\nGenotype – guides treatment", cell_body),
Paragraph("Anti-HCV + HCV RNA\nFibrosis stage", cell_body),
Paragraph("None – no protective antibody; can be reinfected", cell_body)],
[Paragraph("HDV", cell_body), Paragraph("HDAg (early, transient)", cell_body),
Paragraph("Anti-HDV IgM → Acute", cell_body),
Paragraph("Anti-HDV IgG/Total → Chronic or past", cell_body),
Paragraph("HDV RNA (PCR) – confirms replication, monitors therapy", cell_body),
Paragraph("Anti-HDV IgG + HBsAg + HDV RNA", cell_body),
Paragraph("Anti-HBs (prevents by blocking HBV, which HDV requires)", cell_body)],
[Paragraph("HEV", cell_body), Paragraph("HEV Ag (limited)", cell_body),
Paragraph("Anti-HEV IgM → Acute", cell_body),
Paragraph("Anti-HEV IgG → Past (may wane)", cell_body),
Paragraph("HEV RNA (PCR) – gold standard; essential in immunocompromised", cell_body),
Paragraph("None (except immunocompromised: HEV RNA persists)", cell_body),
Paragraph("Partial anti-HEV IgG (wanes; not lifelong like anti-HAV)", cell_body)],
]
master_t = Table(master, colWidths=[1.5*cm, 2.8*cm, 3*cm, 3.2*cm, 3*cm, 2.4*cm, 2.5*cm], repeatRows=1)
master_t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), NAVY),
("ROWBACKGROUNDS",(0,1), (-1,-1), [LIGHT_TEAL, colors.HexColor("#EBF4FA"), LIGHT_TEAL, colors.HexColor("#EBF4FA"), LIGHT_TEAL]),
("GRID", (0,0), (-1,-1), 0.4, MID_GREY),
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING", (0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 4),
("FONTNAME", (0,1), (0,-1), "Helvetica-Bold"),
]))
story.append(master_t)
story.append(Spacer(1, 0.4*cm))
# ═══════════════════════════════════════════════════════════════════════════════
# SECTION 7 – HIGH-YIELD EXAM POINTS
# ═══════════════════════════════════════════════════════════════════════════════
story.append(section_header("SECTION 7 — High-Yield Exam Points & Clinical Pearls", AMBER))
story.append(Spacer(1, 0.2*cm))
pearls = [
("Window Period (HBV)",
"HBsAg has cleared but anti-HBs not yet detectable. ONLY anti-HBc IgM is positive. "
"Never report as 'no HBV' — confirm with HBV DNA."),
("Vaccination vs. Natural Immunity (HBV)",
"Vaccination: only Anti-HBs positive. Natural infection: Anti-HBs + Anti-HBc IgG both positive."),
("Chronic HBV Definition",
"HBsAg positive for >6 months. Subdivide by HBeAg status, ALT, and HBV DNA levels."),
("HCV Antibody ≠ Active Infection",
"Anti-HCV persists lifelong — even after cure (SVR). Always confirm with HCV RNA PCR."),
("SVR12 = HCV Cure",
"Undetectable HCV RNA 12 weeks after end of DAA therapy = sustained virological response = functional cure (~99% permanent)."),
("HDV Requires HBV",
"HDV cannot infect without HBV co-infection. HBV vaccination PREVENTS HDV. "
"Test for HDV ONLY when HBsAg is positive."),
("HEV in Pregnancy",
"20% mortality in 3rd trimester. Always test HEV RNA in pregnant women with acute hepatitis + travel history to endemic areas."),
("No Protective Antibody in HCV",
"Unlike HAV and HBV, resolved HCV infection does NOT confer protection. Reinfection is possible."),
("HBV DNA vs. HBeAg",
"HBeAg-negative chronic hepatitis can still have HIGH HBV DNA (precore mutant). Always measure HBV DNA, not HBeAg alone."),
("Anti-HBc IgM – Low Titre",
"Low titre anti-HBc IgM in a known chronic HBV patient suggests HBV reactivation, not new acute infection."),
("Occult HBV",
"HBsAg negative but HBV DNA detectable (with or without anti-HBc). Risk of reactivation with immunosuppression. Screen with anti-HBc total."),
]
pearl_data = [[Paragraph("Clinical Pearl", cell_hdr), Paragraph("Key Point", cell_hdr)]]
for i, (title, content) in enumerate(pearls):
bg = LIGHT_AMBER if i % 2 == 0 else WHITE
pearl_data.append([
Paragraph(title, S("PearlTitle", fontSize=8, fontName="Helvetica-Bold", textColor=NAVY, leading=11)),
Paragraph(content, cell_body)
])
pearl_t = Table(pearl_data, colWidths=[4.5*cm, 12.9*cm], repeatRows=1)
pearl_t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), AMBER),
("GRID", (0,0), (-1,-1), 0.4, MID_GREY),
("VALIGN", (0,0), (-1,-1), "TOP"),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 6),
("ROWBACKGROUNDS",(0,1), (-1,-1), [LIGHT_AMBER, WHITE] * 6),
]))
story.append(pearl_t)
story.append(Spacer(1, 0.4*cm))
# ═══════════════════════════════════════════════════════════════════════════════
# FOOTER / REFERENCES
# ═══════════════════════════════════════════════════════════════════════════════
story.append(HRFlowable(width="100%", thickness=0.5, color=MID_GREY))
story.append(Spacer(1, 0.15*cm))
story.append(Paragraph(
"References: Ananthanarayan & Paniker's Textbook of Microbiology | "
"Murray et al., Medical Microbiology 9e | Sherris & Ryan's Medical Microbiology 8e | "
"Generated by Orris Medical Reference — June 2026",
footer_style))
# ── BUILD ──────────────────────────────────────────────────────────────────────
doc.build(story)
print(f"PDF generated: {OUTPUT}")
cd /home/daytona/workspace/hepatitis-guide && python generate_pdf.py 2>&1
ls -lh /home/daytona/workspace/hepatitis-guide/
Hepatitis Serological Markers Reference
PDF Document · PDF
Section 1 — Hepatitis B Virus (HBV)
- Individual marker table covering all 10 markers: HBsAg, Anti-HBs, HBcAg (why it's not ordered), Anti-HBc IgM/IgG, HBeAg, Anti-HBe, HBV DNA, and quantitative HBsAg
- 10-row interpretation pattern table with colour-coded rows - including the window period highlighted in amber
- Temporal sequence table showing which markers appear and disappear across 5 clinical phases
Section 2 — Hepatitis A (HAV)
- Anti-HAV IgM vs. IgG explained clearly
- 4-pattern interpretation matrix (acute, acute+recovering, immune, susceptible)
Section 3 — Hepatitis C (HCV)
- Full testing algorithm (screen → confirm → genotype → treat → SVR12)
- Role of each marker: anti-HCV, HCV RNA qual/quant, genotype, core antigen, FibroScan
Section 4 — Hepatitis D (HDV)
- HDAg, Anti-HDV IgM/IgG, HDV RNA explained
- Co-infection vs. Superinfection comparison table - a frequent exam topic
Section 5 — Hepatitis E (HEV)
- Anti-HEV IgM/IgG, HEV RNA - with special note on pregnancy risk
Section 6 — Master Comparison Table
Section 7 — 11 High-Yield Clinical Pearls
Make a comprehensive diagram of all the contents about hepatitis
ls -la /home/daytona/workspace/hepatitis-guide/
~/hepatitis-guide/generate_diagram.py
import matplotlib
matplotlib.use('Agg')
import matplotlib.pyplot as plt
import matplotlib.patches as mpatches
import matplotlib.patches as patches
from matplotlib.patches import FancyBboxPatch, FancyArrowPatch, Arc
from matplotlib.lines import Line2D
import matplotlib.patheffects as pe
import numpy as np
# ── Canvas ─────────────────────────────────────────────────────────────────────
fig = plt.figure(figsize=(28, 38), facecolor='#0D1B2A')
fig.patch.set_facecolor('#0D1B2A')
# ── Colour palette ─────────────────────────────────────────────────────────────
BG = '#0D1B2A'
PANEL_BG = '#122336'
CARD_BG = '#17304A'
CARD_BG2 = '#1A3A56'
WHITE = '#FFFFFF'
CREAM = '#F0F4F8'
GOLD = '#F5A623'
TEAL = '#2DD4BF'
CYAN = '#38BDF8'
ORANGE = '#FB923C'
RED = '#F87171'
GREEN = '#4ADE80'
PURPLE = '#C084FC'
PINK = '#F472B6'
YELLOW = '#FDE68A'
LIME = '#BEF264'
SLATE = '#94A3B8'
BLUE = '#60A5FA'
# Virus colours
HAV_C = '#22D3EE' # cyan
HBV_C = '#4ADE80' # green
HCV_C = '#F97316' # orange
HDV_C = '#C084FC' # purple
HEV_C = '#FBBF24' # amber
# ── Helper functions ───────────────────────────────────────────────────────────
def add_panel(ax, title, title_color=TEAL, bg=PANEL_BG, alpha=0.95):
ax.set_facecolor(bg)
ax.set_xlim(0, 1)
ax.set_ylim(0, 1)
ax.axis('off')
ax.text(0.5, 0.97, title, ha='center', va='top', fontsize=11,
fontweight='bold', color=title_color, fontfamily='DejaVu Sans',
transform=ax.transAxes)
def card(ax, x, y, w, h, color, text, fontsize=8, textcolor=WHITE, valign='center', bold=False, radius=0.025):
box = FancyBboxPatch((x, y), w, h,
boxstyle=f"round,pad=0,rounding_size={radius}",
facecolor=color, edgecolor='none', alpha=0.88,
transform=ax.transAxes, zorder=3)
ax.add_patch(box)
fw = 'bold' if bold else 'normal'
ax.text(x + w/2, y + h/2, text, ha='center', va=valign,
fontsize=fontsize, color=textcolor, fontweight=fw,
transform=ax.transAxes, zorder=4,
wrap=True, multialignment='center')
def hline(ax, y, color=SLATE, lw=0.6, alpha=0.4):
ax.axhline(y=y, color=color, lw=lw, alpha=alpha, transform=ax.transAxes)
def badge(ax, x, y, text, color, fontsize=7.5, textcolor=WHITE):
box = FancyBboxPatch((x-0.005, y-0.012), len(text)*0.013+0.01, 0.034,
boxstyle="round,pad=0,rounding_size=0.012",
facecolor=color, edgecolor='none', alpha=0.9,
transform=ax.transAxes, zorder=5)
ax.add_patch(box)
ax.text(x + len(text)*0.0065, y, text, ha='center', va='center',
fontsize=fontsize, color=textcolor, fontweight='bold',
transform=ax.transAxes, zorder=6)
# ═══════════════════════════════════════════════════════════════════════════════
# GRID LAYOUT
# ═══════════════════════════════════════════════════════════════════════════════
# Row heights (top-to-bottom): title, virus cards, comparison table,
# serology/pathogenesis, transmission/clinical, treatment/prevention, pearls
gs = fig.add_gridspec(
8, 6,
top=0.975, bottom=0.01,
left=0.01, right=0.99,
hspace=0.045, wspace=0.03,
height_ratios=[0.038, 0.13, 0.15, 0.14, 0.145, 0.13, 0.13, 0.075]
)
# ═══════════════════════════════════════════════════════════════════════════════
# ROW 0 — TITLE BAR
# ═══════════════════════════════════════════════════════════════════════════════
ax_title = fig.add_subplot(gs[0, :])
ax_title.set_facecolor('#061120')
ax_title.axis('off')
ax_title.text(0.5, 0.55, 'HEPATITIS VIRUSES — COMPREHENSIVE REFERENCE DIAGRAM',
ha='center', va='center', fontsize=18, fontweight='bold',
color=WHITE, fontfamily='DejaVu Sans', transform=ax_title.transAxes,
path_effects=[pe.withStroke(linewidth=3, foreground='#38BDF8')])
ax_title.text(0.5, 0.08, 'Based on Ananthanarayan Microbiology | Medical Microbiology 9e (Murray et al.) | Sherris & Ryan\'s Medical Microbiology 8e',
ha='center', va='bottom', fontsize=8, color=SLATE,
transform=ax_title.transAxes)
# ═══════════════════════════════════════════════════════════════════════════════
# ROW 1 — VIRUS IDENTITY CARDS (one per virus + one for overview)
# ═══════════════════════════════════════════════════════════════════════════════
virus_info = [
('HAV', 'Hepatitis A', HAV_C,
'Family: Picornaviridae\nGenus: Hepatovirus\nGenome: (+)ssRNA\nSize: 27 nm\nEnvelope: NONE\nSerotypes: 1',
'Fecal-oral\n(water, shellfish)', 'Self-limiting\nNo chronicity\nMortality <0.5%'),
('HBV', 'Hepatitis B', HBV_C,
'Family: Hepadnaviridae\nDane particle: 42 nm\nGenome: Partial dsDNA\nEnvelope: YES\nPolymerase: Reverse\ntranscriptase',
'Parenteral\nSexual\nVertical (mother→child)', 'Chronicity: 10%\n(neonates >90%)\nHCC risk: YES'),
('HCV', 'Hepatitis C', HCV_C,
'Family: Flaviviridae\nGenus: Hepacivirus\nGenome: (+)ssRNA\nSize: ~50 nm\nEnvelope: YES\nGenotypes: 6',
'Parenteral\n(IVDU dominant)\nSexual (low rate)', 'Chronicity: 70–85%\nHCC risk: YES\nCurable with DAAs'),
('HDV', 'Hepatitis D', HDV_C,
'Delta agent (satellite)\nRequires HBV\nGenome: (-)ssRNA\n(circular, 1700 nt)\nEnvelope: HBsAg\nSize: 35–37 nm',
'Parenteral\nSexual\n(same as HBV)', 'Co-infect: resolves\nSuperinfect:\n>80% chronic'),
('HEV', 'Hepatitis E', HEV_C,
'Family: Hepeviridae\nGenus: Orthohepevirus\nGenome: (+)ssRNA\nSize: 27–34 nm\nEnvelope: NONE\nGenotypes: 4',
'Fecal-oral\n(waterborne)\nZoonotic (G3/G4)', 'Usually self-limit\nPregnancy: 20% mort.\nChronic: immunosupp.'),
]
for i, (abbr, name, col, struct, trans, outcome) in enumerate(virus_info):
ax = fig.add_subplot(gs[1, i])
ax.set_facecolor(PANEL_BG)
ax.set_xlim(0, 1); ax.set_ylim(0, 1); ax.axis('off')
# Top colour stripe
stripe = FancyBboxPatch((0, 0.82), 1, 0.18,
boxstyle="round,pad=0,rounding_size=0",
facecolor=col, edgecolor='none', alpha=0.9,
transform=ax.transAxes, zorder=2)
ax.add_patch(stripe)
ax.text(0.18, 0.91, abbr, ha='center', va='center', fontsize=16,
fontweight='bold', color='#0D1B2A', transform=ax.transAxes, zorder=3)
ax.text(0.62, 0.91, name, ha='center', va='center', fontsize=9,
fontweight='bold', color='#0D1B2A', transform=ax.transAxes, zorder=3)
# Structure block
ax.text(0.05, 0.79, 'STRUCTURE', ha='left', va='top', fontsize=6.5,
fontweight='bold', color=col, transform=ax.transAxes)
ax.text(0.05, 0.73, struct, ha='left', va='top', fontsize=6.8,
color=CREAM, transform=ax.transAxes, linespacing=1.5)
hline(ax, 0.40)
ax.text(0.05, 0.39, 'TRANSMISSION', ha='left', va='top', fontsize=6.5,
fontweight='bold', color=ORANGE, transform=ax.transAxes)
ax.text(0.05, 0.34, trans, ha='left', va='top', fontsize=7,
color=CREAM, transform=ax.transAxes, linespacing=1.5)
hline(ax, 0.18)
ax.text(0.05, 0.17, 'OUTCOME', ha='left', va='top', fontsize=6.5,
fontweight='bold', color=RED, transform=ax.transAxes)
ax.text(0.05, 0.12, outcome, ha='left', va='top', fontsize=7,
color=CREAM, transform=ax.transAxes, linespacing=1.5)
# Border
for spine in ['top','bottom','left','right']:
ax.spines[spine].set_visible(False)
rect = FancyBboxPatch((0.005, 0.005), 0.99, 0.99,
boxstyle="round,pad=0,rounding_size=0.04",
facecolor='none', edgecolor=col, linewidth=1.5, alpha=0.6,
transform=ax.transAxes, zorder=5)
ax.add_patch(rect)
# ═══════════════════════════════════════════════════════════════════════════════
# ROW 2 — COMPARISON TABLE
# ═══════════════════════════════════════════════════════════════════════════════
ax_cmp = fig.add_subplot(gs[2, :])
ax_cmp.set_facecolor(PANEL_BG)
ax_cmp.set_xlim(0, 1); ax_cmp.set_ylim(0, 1); ax_cmp.axis('off')
ax_cmp.text(0.5, 0.975, 'COMPARATIVE FEATURES OF HEPATITIS VIRUSES',
ha='center', va='top', fontsize=10, fontweight='bold',
color=TEAL, transform=ax_cmp.transAxes)
# Table data
headers = ['Feature', 'HAV', 'HBV', 'HCV', 'HDV', 'HEV']
rows = [
['Common name', '"Infectious"', '"Serum"', '"Non-A,non-B\npost-transf."', '"Delta agent"', '"Enteric non-A,non-B"'],
['Genome', '(+)ssRNA', 'Partial dsDNA', '(+)ssRNA', '(-)ssRNA circular', '(+)ssRNA'],
['Envelope', 'NO', 'YES', 'YES', 'YES (HBsAg)', 'NO'],
['Incubation', '15–50 days', '45–160 days', '14–180 days', '15–64 days', '15–50 days'],
['Onset', 'Abrupt', 'Insidious', 'Insidious', 'Variable', 'Abrupt'],
['Chronicity', 'NONE', '10% (adults)\n>90% neonates', '70–85%', '50–80%\n(superinfection)', 'NONE*'],
['Carrier state', 'No', 'Yes', 'Yes', 'Yes', 'No'],
['HCC risk', 'No', 'YES', 'YES', 'YES', 'No'],
['Mortality', '<0.5%', '1–2%', '~4%', 'High–very high', '1–2%\n(20% pregnant)'],
['Vaccine', 'YES (inactivated)', 'YES (recombinant)', 'NO', 'Via HBV vaccine', 'China only'],
['Key diagnosis', 'Anti-HAV IgM', 'HBsAg + Anti-HBc IgM', 'Anti-HCV + HCV RNA', 'Anti-HDV + HDV RNA', 'Anti-HEV IgM'],
['Treatment', 'Supportive', 'IFN + NRTIs', 'DAAs (>95% cure)', 'Bulevirtide (limited)', 'Supportive\n(Ribavirin: chronic)'],
]
col_colors = ['#1E3A52', HAV_C, HBV_C, HCV_C, HDV_C, HEV_C]
col_w = [0.155, 0.155, 0.155, 0.165, 0.16, 0.165]
col_x = [0.005]
for w in col_w[:-1]:
col_x.append(col_x[-1] + w)
n_rows = len(rows)
row_h = 0.845 / n_rows
header_y = 0.915
# Header row
for j, (hdr, cx, cw, cc) in enumerate(zip(headers, col_x, col_w, col_colors)):
hbox = FancyBboxPatch((cx+0.001, header_y - 0.042), cw-0.002, 0.042,
boxstyle="round,pad=0,rounding_size=0.008",
facecolor=cc if j > 0 else '#1B4F72',
edgecolor='none', alpha=0.95,
transform=ax_cmp.transAxes, zorder=2)
ax_cmp.add_patch(hbox)
ax_cmp.text(cx + cw/2, header_y - 0.021, hdr,
ha='center', va='center', fontsize=8.5,
fontweight='bold', color='#0D1B2A' if j > 0 else WHITE,
transform=ax_cmp.transAxes, zorder=3)
# Data rows
green_rows = {0, 9, 10} # common name, vaccine, diagnosis
amber_rows = {3, 4, 8} # incubation, onset, mortality
red_rows = {5, 6, 7} # chronicity, carrier, HCC
special_vals = {
('NONE', HAV_C): RED, ('NONE', HEV_C): RED,
('Yes', HBV_C): RED, ('Yes', HCV_C): RED, ('Yes', HDV_C): RED,
('NO', HCV_C): RED,
('YES', HBV_C): RED, ('YES', HCV_C): RED, ('YES', HDV_C): RED,
}
for i, row in enumerate(rows):
y_top = header_y - 0.045 - i * row_h - 0.004
row_bg = '#132A40' if i % 2 == 0 else '#0F2030'
for j, (val, cx, cw) in enumerate(zip(row, col_x, col_w)):
bg = row_bg if j == 0 else row_bg
if j == 0:
tc = SLATE
fs = 7.5
fw = 'bold'
else:
tc = CREAM
fs = 7.2
fw = 'normal'
# Highlight important values
v = val.strip()
if v in ('YES', '>95% cure', 'YES (inactivated)', 'YES (recombinant)'):
tc = GREEN; fw = 'bold'
elif v in ('NONE', 'NO', 'No', 'Supportive'):
tc = SLATE
elif v in ('High–very high', '70–85%', '20% pregnant', '>90% neonates'):
tc = RED; fw = 'bold'
elif v in ('Anti-HAV IgM', 'HBsAg + Anti-HBc IgM', 'Anti-HCV + HCV RNA',
'Anti-HDV + HDV RNA', 'Anti-HEV IgM'):
tc = CYAN; fw = 'bold'
rbox = FancyBboxPatch((cx+0.001, y_top), cw-0.002, row_h-0.004,
boxstyle="round,pad=0,rounding_size=0.004",
facecolor=bg, edgecolor='none', alpha=1,
transform=ax_cmp.transAxes, zorder=2)
ax_cmp.add_patch(rbox)
ax_cmp.text(cx + cw/2, y_top + row_h/2 - 0.002, val,
ha='center', va='center', fontsize=fs, color=tc,
fontweight=fw, transform=ax_cmp.transAxes, zorder=3,
multialignment='center', linespacing=1.35)
# ═══════════════════════════════════════════════════════════════════════════════
# ROW 3 — SEROLOGY (left 3 cols) + PATHOGENESIS (right 3 cols)
# ═══════════════════════════════════════════════════════════════════════════════
ax_sero = fig.add_subplot(gs[3, :3])
add_panel(ax_sero, 'HBV SEROLOGICAL MARKERS & PATTERNS', TEAL)
sero_markers = [
('HBsAg', 'Surface antigen — 1st marker; active infection', HBV_C),
('Anti-HBs', 'Protective Ab; recovery or vaccination', GREEN),
('HBeAg', 'High infectivity / active replication', ORANGE),
('Anti-HBe', 'Seroconversion; declining replication', YELLOW),
('Anti-HBc IgM','ACUTE infection; sole marker in window period', RED),
('Anti-HBc IgG','Past or current exposure; persists lifelong', SLATE),
('HBV DNA', 'Viral load; gold standard for replication', CYAN),
]
y_start = 0.88
dy = 0.093
for marker, meaning, col in sero_markers:
box = FancyBboxPatch((0.01, y_start - 0.065), 0.23, 0.06,
boxstyle="round,pad=0,rounding_size=0.015",
facecolor=col, edgecolor='none', alpha=0.85,
transform=ax_sero.transAxes, zorder=3)
ax_sero.add_patch(box)
ax_sero.text(0.125, y_start - 0.035, marker,
ha='center', va='center', fontsize=7.5, fontweight='bold',
color='#0D1B2A', transform=ax_sero.transAxes, zorder=4)
ax_sero.text(0.26, y_start - 0.035, meaning,
ha='left', va='center', fontsize=7.2, color=CREAM,
transform=ax_sero.transAxes, zorder=4)
y_start -= dy
# Interpretation patterns (mini table)
ax_sero.text(0.5, 0.33, 'KEY INTERPRETATION PATTERNS', ha='center', va='center',
fontsize=7.5, fontweight='bold', color=TEAL, transform=ax_sero.transAxes)
patterns = [
('+', '–', '+', '–', '+', '+', 'Acute infection'),
('–', '–', '–', '–', '+', '+', '⚠ Window period — test HBV DNA'),
('–', '+', '–', '–', '–', '+', 'Resolved — immune'),
('–', '+', '–', '–', '–', '–', 'Vaccinated only'),
('+', '–', '–', '+', '+', '+', 'Chronic (HBeAg+)'),
('+', '–', '+', '–', '–', '+', 'Chronic (HBeAg−)'),
]
hdrs_p = ['HBsAg','Anti-HBs','HBeAg','Anti-HBe','IgM','IgG','Meaning']
px = [0.02, 0.12, 0.22, 0.32, 0.42, 0.50, 0.58]
pw = [0.09, 0.09, 0.09, 0.09, 0.07, 0.07, 0.42]
hdr_y = 0.285
for hd, x, w in zip(hdrs_p, px, pw):
ax_sero.text(x + w/2, hdr_y, hd, ha='center', va='center',
fontsize=6.5, fontweight='bold', color=TEAL,
transform=ax_sero.transAxes)
for ri, pat in enumerate(patterns):
py = hdr_y - 0.04 - ri * 0.038
bg_col = '#0A1F30' if ri % 2 == 0 else '#0D2840'
if '⚠' in pat[-1]:
bg_col = '#3D1A00'
rb = FancyBboxPatch((0.01, py - 0.015), 0.98, 0.032,
boxstyle="round,pad=0,rounding_size=0.006",
facecolor=bg_col, edgecolor='none',
transform=ax_sero.transAxes, zorder=2)
ax_sero.add_patch(rb)
for vi, (val, x, w) in enumerate(zip(pat, px, pw)):
if vi < 6:
tc = GREEN if val == '+' else RED if val == '–' else WHITE
fw = 'bold'
else:
tc = YELLOW if '⚠' in val else CREAM
fw = 'normal'
ax_sero.text(x + w/2, py, val, ha='center', va='center',
fontsize=6.8, color=tc, fontweight=fw,
transform=ax_sero.transAxes)
# Pathogenesis panel
ax_path = fig.add_subplot(gs[3, 3:])
add_panel(ax_path, 'PATHOGENESIS — HOW HEPATITIS VIRUSES CAUSE DISEASE', PURPLE)
path_data = [
('HAV', HAV_C,
'Entry via fecal-oral → hepatocytes → NOT cytolytic\n→ Immune-mediated damage (CD8+ T cells)\n→ Self-limiting; strong immune response clears virus'),
('HBV', HBV_C,
'Parenteral entry → hepatocyte infection → reverse transcriptase replication\n→ Immune-mediated (CD8+ T cells kill infected cells)\n→ Immune complex disease: serum sickness, glomerulonephritis\n→ Integrated DNA → oncogenesis (HCC)'),
('HCV', HCV_C,
'Parenteral entry → hepatocyte infection → HIGH mutation rate\n→ Quasispecies escape immune surveillance\n→ Direct cytopathic + immune-mediated damage\n→ Chronic inflammation → fibrosis → cirrhosis → HCC'),
('HDV', HDV_C,
'Requires HBsAg envelope to enter hepatocytes\n→ HDAg disrupts HBV replication (superinfection)\n→ Immune and direct cytopathic mechanisms\n→ Superinfection: rapid progression; co-infection: resolves'),
('HEV', HEV_C,
'Fecal-oral entry → gut → portal circulation → hepatocytes\n→ Direct cytopathic + immune-mediated\n→ Self-limiting usually; severe in pregnancy (hormonal)\n→ Chronic in transplant patients (genotype 3)'),
]
yp = 0.90
for abbr, col, text in path_data:
bbox = FancyBboxPatch((0.01, yp - 0.145), 0.98, 0.145,
boxstyle="round,pad=0,rounding_size=0.015",
facecolor=CARD_BG, edgecolor=col, linewidth=1,
transform=ax_path.transAxes, zorder=2)
ax_path.add_patch(bbox)
ax_path.text(0.045, yp - 0.04, abbr, ha='center', va='center',
fontsize=9, fontweight='bold', color=col,
transform=ax_path.transAxes, zorder=3)
ax_path.text(0.09, yp - 0.028, text, ha='left', va='top',
fontsize=6.8, color=CREAM, transform=ax_path.transAxes,
zorder=3, linespacing=1.5)
yp -= 0.17
# ═══════════════════════════════════════════════════════════════════════════════
# ROW 4 — TRANSMISSION (left 3) + CLINICAL FEATURES (right 3)
# ═══════════════════════════════════════════════════════════════════════════════
ax_trans = fig.add_subplot(gs[4, :3])
add_panel(ax_trans, 'TRANSMISSION ROUTES', ORANGE)
# Transmission wheel / matrix
routes = [
('Fecal-Oral\n(Water/Food)', [True, False, False, False, True], HAV_C),
('Parenteral\n(Blood/IVDU)', [False, True, True, True, False], RED),
('Sexual', [True, True, True, True, False], PINK),
('Vertical\n(Mother→Child)', [False, True, True, True, False], PURPLE),
('Zoonotic\n(Pigs G3/G4)', [False, False, False, False, True], LIME),
]
viruses_t = ['HAV', 'HBV', 'HCV', 'HDV', 'HEV']
vcols_t = [HAV_C, HBV_C, HCV_C, HDV_C, HEV_C]
# Column headers (virus names)
xs_t = [0.32, 0.44, 0.56, 0.68, 0.80]
for xi, (v, vc) in enumerate(zip(viruses_t, vcols_t)):
bx = FancyBboxPatch((xs_t[xi] - 0.05, 0.87), 0.1, 0.055,
boxstyle="round,pad=0,rounding_size=0.015",
facecolor=vc, edgecolor='none', alpha=0.85,
transform=ax_trans.transAxes, zorder=3)
ax_trans.add_patch(bx)
ax_trans.text(xs_t[xi], 0.897, v, ha='center', va='center',
fontsize=8.5, fontweight='bold', color='#0D1B2A',
transform=ax_trans.transAxes, zorder=4)
# Rows
for ri, (route, flags, rc) in enumerate(routes):
ry = 0.83 - ri * 0.155
# Route label
rb = FancyBboxPatch((0.005, ry - 0.065), 0.28, 0.075,
boxstyle="round,pad=0,rounding_size=0.015",
facecolor=rc, edgecolor='none', alpha=0.8,
transform=ax_trans.transAxes, zorder=3)
ax_trans.add_patch(rb)
ax_trans.text(0.145, ry - 0.028, route, ha='center', va='center',
fontsize=7.5, fontweight='bold', color='#0D1B2A',
transform=ax_trans.transAxes, zorder=4, multialignment='center')
# Checkmarks
for xi, (flag, vc) in enumerate(zip(flags, vcols_t)):
sym = '✔' if flag else '✖'
col_sym = GREEN if flag else '#3A3A4A'
ax_trans.text(xs_t[xi], ry - 0.028, sym, ha='center', va='center',
fontsize=14, color=col_sym,
transform=ax_trans.transAxes, zorder=4)
# Risk note box
note_bx = FancyBboxPatch((0.005, 0.02), 0.99, 0.08,
boxstyle="round,pad=0,rounding_size=0.015",
facecolor='#1A0A00', edgecolor=ORANGE, linewidth=0.8,
transform=ax_trans.transAxes, zorder=3)
ax_trans.add_patch(note_bx)
ax_trans.text(0.5, 0.06, 'HDV ONLY infects when HBV is present | HBV has highest blood-borne transmissibility | HEV genotype 3/4 is zoonotic (pigs)',
ha='center', va='center', fontsize=7, color=YELLOW,
transform=ax_trans.transAxes, zorder=4)
# Clinical features panel
ax_clin = fig.add_subplot(gs[4, 3:])
add_panel(ax_clin, 'CLINICAL FEATURES & PHASES OF ACUTE HEPATITIS', CYAN)
# Clinical phases timeline
phases = ['Incubation', 'Prodrome\n(Pre-icteric)', 'Icteric\n(Jaundice)', 'Recovery\n(Convalescent)']
phase_colors = ['#1A3A56', '#2D4A1A', '#4A2D1A', '#1A4A2D']
phase_x = [0.05, 0.28, 0.55, 0.78]
phase_w = 0.2
for px_pos, ph, phc in zip(phase_x, phases, phase_colors):
pb = FancyBboxPatch((px_pos, 0.86), phase_w, 0.07,
boxstyle="round,pad=0,rounding_size=0.015",
facecolor=phc, edgecolor=CYAN, linewidth=0.8,
transform=ax_clin.transAxes, zorder=3)
ax_clin.add_patch(pb)
ax_clin.text(px_pos + phase_w/2, 0.895, ph, ha='center', va='center',
fontsize=7.5, fontweight='bold', color=WHITE,
transform=ax_clin.transAxes, zorder=4, multialignment='center')
if px_pos < 0.78:
ax_clin.annotate('', xy=(px_pos + phase_w + 0.025, 0.895),
xytext=(px_pos + phase_w, 0.895),
arrowprops=dict(arrowstyle='->', color=CYAN, lw=1.5),
xycoords='axes fraction', textcoords='axes fraction')
# Symptoms by phase
symp_data = [
('Incubation\nSymptoms', 'Often\nasymptomatic\nViral replication', '0.07'),
('Prodrome\nSymptoms', 'Fever, malaise\nAnorexia, nausea\nVomiting, RUQ pain\nArthralgia, rash\n(esp. HBV)', '0.065'),
('Icteric\nSymptoms', 'Jaundice (yellow\nsclera/skin)\nDark urine\n(bilirubin)\nPale/clay stools\nHepatomegaly', '0.065'),
('Recovery\nSigns', 'Jaundice fades\nAppetite returns\nEnergy improves\nLiver enzymes\nnormalise', '0.065'),
]
for si, (label, syms, fsize) in enumerate(symp_data):
sx = phase_x[si]
sb = FancyBboxPatch((sx, 0.55), phase_w, 0.285,
boxstyle="round,pad=0,rounding_size=0.012",
facecolor=CARD_BG, edgecolor=phase_colors[si], linewidth=0.8,
transform=ax_clin.transAxes, zorder=3)
ax_clin.add_patch(sb)
ax_clin.text(sx + phase_w/2, 0.822, label, ha='center', va='top',
fontsize=6.8, fontweight='bold', color=CYAN,
transform=ax_clin.transAxes, zorder=4, multialignment='center')
ax_clin.text(sx + phase_w/2, 0.785, syms, ha='center', va='top',
fontsize=float(fsize) - 0.01, color=CREAM,
transform=ax_clin.transAxes, zorder=4,
multialignment='center', linespacing=1.45)
# Lab findings
ax_clin.text(0.5, 0.52, 'KEY LAB FINDINGS IN ACUTE HEPATITIS', ha='center', va='center',
fontsize=7.5, fontweight='bold', color=CYAN, transform=ax_clin.transAxes)
labs = [
('↑↑↑ ALT & AST', 'Hepatocellular damage (ALT > AST)', GREEN),
('↑ Bilirubin', 'Direct + indirect; causes jaundice', YELLOW),
('↑ ALP/GGT', 'Cholestasis component', ORANGE),
('↑ PT/INR', 'Severe disease; liver synthetic failure', RED),
('↓ Albumin', 'Chronic disease or severe acute', RED),
]
lab_x_start = 0.01
lab_w = 0.195
for li, (lab, meaning, lc) in enumerate(labs):
lx = lab_x_start + li * (lab_w + 0.005)
lb = FancyBboxPatch((lx, 0.36), lab_w, 0.135,
boxstyle="round,pad=0,rounding_size=0.012",
facecolor=CARD_BG, edgecolor=lc, linewidth=0.9,
transform=ax_clin.transAxes, zorder=3)
ax_clin.add_patch(lb)
ax_clin.text(lx + lab_w/2, 0.435, lab, ha='center', va='center',
fontsize=8, fontweight='bold', color=lc,
transform=ax_clin.transAxes, zorder=4)
ax_clin.text(lx + lab_w/2, 0.385, meaning, ha='center', va='center',
fontsize=6.2, color=CREAM,
transform=ax_clin.transAxes, zorder=4, multialignment='center')
# Complications
ax_clin.text(0.5, 0.33, 'COMPLICATIONS', ha='center', va='center',
fontsize=7.5, fontweight='bold', color=RED, transform=ax_clin.transAxes)
comp_data = [
('Fulminant\nHepatic Failure', 'HBV (1%)\nHDV superinfect.\nHEV in pregnancy', RED),
('Cirrhosis', 'HBV chronic\nHCV chronic\nHDV chronic', ORANGE),
('Hepatocellular\nCarcinoma (HCC)', 'HBV, HCV, HDV\n(viral DNA integration\nor chronic inflam.)', PINK),
('Extrahepatic', 'HBV: PAN,\nglomerulopathy\nHCV: cryo-\nglobulinaemia', PURPLE),
('Chronic\nCarrier State', 'HBV, HCV, HDV\n(not HAV/HEV\n in normal hosts)', SLATE),
]
comp_x = lab_x_start
for ci, (comp, det, cc) in enumerate(comp_data):
cx = comp_x + ci * (lab_w + 0.005)
cb = FancyBboxPatch((cx, 0.05), lab_w, 0.255,
boxstyle="round,pad=0,rounding_size=0.012",
facecolor=CARD_BG2, edgecolor=cc, linewidth=0.8,
transform=ax_clin.transAxes, zorder=3)
ax_clin.add_patch(cb)
ax_clin.text(cx + lab_w/2, 0.275, comp, ha='center', va='top',
fontsize=7, fontweight='bold', color=cc,
transform=ax_clin.transAxes, zorder=4, multialignment='center', linespacing=1.3)
ax_clin.text(cx + lab_w/2, 0.195, det, ha='center', va='top',
fontsize=6.5, color=CREAM,
transform=ax_clin.transAxes, zorder=4, multialignment='center', linespacing=1.4)
# ═══════════════════════════════════════════════════════════════════════════════
# ROW 5 — SEROLOGY TIMELINES (left 3) + TREATMENT (right 3)
# ═══════════════════════════════════════════════════════════════════════════════
ax_time = fig.add_subplot(gs[5, :3])
add_panel(ax_time, 'HBV SEROLOGICAL TIMELINE (Acute vs. Chronic)', HBV_C)
# Simplified HBV timeline using curves
ax_time.set_xlim(0, 1); ax_time.set_ylim(0, 1)
t = np.linspace(0, 1, 300)
def bell(peak_x, peak_y, width, offset=0):
return peak_y * np.exp(-((t - peak_x)**2) / (2 * width**2)) + offset
def sigmoid_up(start, end, steep=20):
mid = (start + end) / 2
return 0.55 / (1 + np.exp(-steep * (t - mid)))
def sigmoid_down(start, end, steep=20):
mid = (start + end) / 2
return 0.55 * (1 - 1 / (1 + np.exp(-steep * (t - mid))))
# -- ACUTE HBV (left half)
ax_time.text(0.13, 0.93, 'ACUTE HBV (Resolves)', ha='center', va='top',
fontsize=7.5, fontweight='bold', color=HBV_C, transform=ax_time.transAxes)
ax_time.text(0.63, 0.93, 'CHRONIC HBV (Persists)', ha='center', va='top',
fontsize=7.5, fontweight='bold', color=ORANGE, transform=ax_time.transAxes)
ax_time.axvline(x=0.5, color=SLATE, lw=0.8, alpha=0.5, linestyle='--', transform=ax_time.transAxes)
# Acute side (t=0..0.5)
ta = np.linspace(0, 0.5, 200)
def acute_curve(center, height, width):
return height * np.exp(-((ta - center)**2) / (2*width**2))
curves_acute = [
('HBsAg', 0.18, 0.55, 0.07, HBV_C, '-'),
('HBeAg', 0.15, 0.45, 0.05, ORANGE, '-'),
('Anti-HBc\nIgM', 0.22, 0.50, 0.07, RED, '--'),
('Anti-HBc\nIgG', 0.30, 0.55, 0.12, SLATE, '-'),
('Anti-HBs', 0.42, 0.55, 0.06, GREEN, '-'),
('Anti-HBe', 0.35, 0.40, 0.06, YELLOW, '-'),
]
ax_time.axhline(y=0.18, xmin=0, xmax=0.5, color=SLATE, lw=0.4, alpha=0.3, transform=ax_time.transAxes)
for lbl, ctr, ht, wd, col, ls in curves_acute:
yv = acute_curve(ctr, ht, wd) + 0.15
ax_time.plot(ta, yv, color=col, lw=1.8, linestyle=ls, transform=ax_time.transAxes, zorder=3)
# label at peak
peak_i = np.argmax(yv)
ax_time.text(ta[peak_i], yv[peak_i] + 0.03, lbl, ha='center', va='bottom',
fontsize=5.5, color=col, transform=ax_time.transAxes, multialignment='center')
# X axis labels for acute
ax_time.text(0.02, 0.09, '0', ha='center', fontsize=6, color=SLATE, transform=ax_time.transAxes)
ax_time.text(0.15, 0.09, 'Exposure', ha='center', fontsize=6, color=SLATE, transform=ax_time.transAxes)
ax_time.text(0.25, 0.09, 'Acute\nSymptoms', ha='center', fontsize=6, color=SLATE, transform=ax_time.transAxes, multialignment='center')
ax_time.text(0.40, 0.09, 'Recovery', ha='center', fontsize=6, color=GREEN, transform=ax_time.transAxes)
ax_time.text(0.22, 0.04, '← Weeks to months →', ha='center', fontsize=6, color=SLATE, transform=ax_time.transAxes)
# Window period annotation
ax_time.annotate('', xy=(0.335, 0.20), xytext=(0.265, 0.20),
arrowprops=dict(arrowstyle='<->', color=YELLOW, lw=1),
xycoords='axes fraction', textcoords='axes fraction')
ax_time.text(0.30, 0.22, 'Window\nperiod', ha='center', va='bottom', fontsize=5.5,
color=YELLOW, fontweight='bold', transform=ax_time.transAxes, multialignment='center')
# Chronic side (t=0.5..1.0)
tc_arr = np.linspace(0.5, 1.0, 200)
def chronic_curve(start, ht, decay=0):
base = np.ones_like(tc_arr) * ht
if decay:
base = ht * np.exp(-decay * (tc_arr - 0.5))
return np.clip(base, 0, 1)
chronic_curves = [
('HBsAg\n(persists)', 0.55, 0, HBV_C, '-'),
('HBeAg', 0.42, 2.5, ORANGE, '-'),
('Anti-HBe', 0.35, -1.5, YELLOW, '-'),
('Anti-HBc\nIgG', 0.50, 0, SLATE, '--'),
('HBV DNA\n(varies)', 0.48, 0, CYAN, '-.'),
]
for lbl, ht, decay, col, ls in chronic_curves:
if decay < 0:
yv = 0.35 / (1 + np.exp(6 * (tc_arr - 0.65))) + 0.15
else:
yv = chronic_curve(0.5, ht, max(0, decay)) + 0.15
ax_time.plot(tc_arr, yv, color=col, lw=1.8, linestyle=ls, transform=ax_time.transAxes, zorder=3)
mid_i = len(tc_arr) // 2
ax_time.text(tc_arr[mid_i], yv[mid_i] + 0.03, lbl, ha='center', va='bottom',
fontsize=5.5, color=col, transform=ax_time.transAxes, multialignment='center')
ax_time.text(0.72, 0.05, 'HBsAg positive >6 months = CHRONIC', ha='center', fontsize=6.5,
fontweight='bold', color=RED, transform=ax_time.transAxes)
# Treatment panel
ax_tx = fig.add_subplot(gs[5, 3:])
add_panel(ax_tx, 'TREATMENT & PROPHYLAXIS', GREEN)
tx_data = [
('HAV', HAV_C,
'ACUTE: Supportive (rest, hydration, avoid hepatotoxins)\n'
'PROPHYLAXIS:\n'
' • Pre-exposure: Inactivated HAV vaccine (2 doses, 0 & 6–12 mo) — lifelong protection\n'
' • Post-exposure: ISG (immune serum globulin) within 2 weeks OR HAV vaccine'),
('HBV', HBV_C,
'ACUTE: Supportive; antivirals rarely needed\n'
'CHRONIC: Pegylated interferon-alfa-2a (48 wks) OR\n'
' Nucleoside/nucleotide analogues (NRTIs/NNRTIs):\n'
' • Tenofovir disoproxil (TDF) — first-line\n'
' • Entecavir — first-line; high barrier to resistance\n'
' • Lamivudine, Adefovir, Telbivudine (older, resistance risk)\n'
'PROPHYLAXIS: Recombinant HBsAg vaccine (3 doses: 0, 1, 6 mo)\n'
' HBIG: post-exposure + neonates of HBsAg+ mothers'),
('HCV', HCV_C,
'TREATMENT (ALL CHRONIC HCV):\n'
' Direct-Acting Antivirals (DAAs) — >95% SVR12 cure rate:\n'
' • Sofosbuvir + Ledipasvir (genotype 1,4,5,6)\n'
' • Sofosbuvir + Velpatasvir (pangenotypic)\n'
' • Glecaprevir + Pibrentasvir (pangenotypic)\n'
' Old: Peg-IFN + Ribavirin (≤50% response, many SEs)\n'
'PROPHYLAXIS: No vaccine available; avoid needle sharing'),
('HDV', HDV_C,
'TREATMENT: Pegylated interferon (partial response)\n'
' Bulevirtide (entry inhibitor, EU approved 2020) — reduces HDV RNA\n'
'KEY: Treating HBV reduces HDV (HDV needs HBsAg)\n'
'PROPHYLAXIS: HBV vaccination PREVENTS HDV entirely'),
('HEV', HEV_C,
'ACUTE (immunocompetent): Supportive only; self-limiting\n'
'CHRONIC (immunocompromised/transplant):\n'
' • Ribavirin (6 months) — reduce immunosuppression first\n'
'PREGNANCY: Intensive supportive care; ribavirin contraindicated\n'
'PROPHYLAXIS: Safe water/sanitation; no widely available vaccine'),
]
ty = 0.91
dty = 0.163
for abbr, col, text in tx_data:
tb = FancyBboxPatch((0.005, ty - dty + 0.005), 0.99, dty - 0.008,
boxstyle="round,pad=0,rounding_size=0.012",
facecolor=CARD_BG, edgecolor=col, linewidth=0.9,
transform=ax_tx.transAxes, zorder=2)
ax_tx.add_patch(tb)
ax_tx.text(0.03, ty - 0.025, abbr, ha='left', va='top', fontsize=9,
fontweight='bold', color=col, transform=ax_tx.transAxes, zorder=3)
ax_tx.text(0.085, ty - 0.015, text, ha='left', va='top', fontsize=6.4,
color=CREAM, transform=ax_tx.transAxes, zorder=3, linespacing=1.45)
ty -= dty
# ═══════════════════════════════════════════════════════════════════════════════
# ROW 6 — HAV/HEV SEROLOGY (left 3) + HDV PATTERNS (right 3)
# ═══════════════════════════════════════════════════════════════════════════════
ax_hav_sero = fig.add_subplot(gs[6, :3])
add_panel(ax_hav_sero, 'HAV · HCV · HEV SEROLOGICAL MARKERS', CYAN)
# HAV
ax_hav_sero.text(0.01, 0.93, 'HAV SEROLOGY', fontsize=8, fontweight='bold',
color=HAV_C, transform=ax_hav_sero.transAxes)
hav_rows = [
('Anti-HAV IgM + / Anti-HAV IgG −', 'Early acute HAV infection', GREEN, RED),
('Anti-HAV IgM + / Anti-HAV IgG +', 'Acute HAV (IgG appearing)', GREEN, GREEN),
('Anti-HAV IgM − / Anti-HAV IgG +', 'Past infection or vaccinated — IMMUNE', RED, GREEN),
('Anti-HAV IgM − / Anti-HAV IgG −', 'Susceptible — no immunity', RED, RED),
]
for ri, (pat, interp, c1, c2) in enumerate(hav_rows):
ry2 = 0.865 - ri * 0.085
rb2 = FancyBboxPatch((0.005, ry2 - 0.055), 0.99, 0.055,
boxstyle="round,pad=0,rounding_size=0.01",
facecolor='#0A1F30' if ri % 2 == 0 else '#0D2840',
edgecolor='none', transform=ax_hav_sero.transAxes, zorder=2)
ax_hav_sero.add_patch(rb2)
ax_hav_sero.text(0.35, ry2 - 0.027, pat, ha='center', va='center',
fontsize=7, color=CREAM, transform=ax_hav_sero.transAxes, zorder=3)
ax_hav_sero.text(0.73, ry2 - 0.027, interp, ha='center', va='center',
fontsize=7, color=YELLOW, fontweight='bold',
transform=ax_hav_sero.transAxes, zorder=3)
# HCV
ax_hav_sero.text(0.01, 0.500, 'HCV TESTING ALGORITHM', fontsize=8, fontweight='bold',
color=HCV_C, transform=ax_hav_sero.transAxes)
algo_steps = [
(0.12, 0.44, 'Screen:\nAnti-HCV ELISA', HCV_C),
(0.38, 0.44, 'Confirm:\nHCV RNA PCR', ORANGE),
(0.62, 0.44, 'Quantify:\nViral load + Genotype', YELLOW),
(0.87, 0.44, 'Monitor:\nSVR12 post-DAA', GREEN),
]
for xi2, yi2, step_txt, sc in algo_steps:
sb2 = FancyBboxPatch((xi2 - 0.1, yi2 - 0.075), 0.2, 0.09,
boxstyle="round,pad=0,rounding_size=0.015",
facecolor=CARD_BG, edgecolor=sc, linewidth=0.9,
transform=ax_hav_sero.transAxes, zorder=3)
ax_hav_sero.add_patch(sb2)
ax_hav_sero.text(xi2, yi2 - 0.03, step_txt, ha='center', va='center',
fontsize=7, fontweight='bold', color=sc,
transform=ax_hav_sero.transAxes, zorder=4, multialignment='center')
if xi2 < 0.87:
ax_hav_sero.annotate('', xy=(xi2 + 0.115, yi2 - 0.03),
xytext=(xi2 + 0.1, yi2 - 0.03),
arrowprops=dict(arrowstyle='->', color=CYAN, lw=1.5),
xycoords='axes fraction', textcoords='axes fraction')
ax_hav_sero.text(0.5, 0.32, 'Anti-HCV + = screen reactive | HCV RNA + = ACTIVE infection | HCV RNA − = Resolved | SVR12 = CURED',
ha='center', va='center', fontsize=7, color=CREAM,
transform=ax_hav_sero.transAxes)
# HEV
ax_hav_sero.text(0.01, 0.265, 'HEV SEROLOGY', fontsize=8, fontweight='bold',
color=HEV_C, transform=ax_hav_sero.transAxes)
hev_rows = [
('Anti-HEV IgM +', 'ACUTE HEV infection'),
('Anti-HEV IgG + / IgM −', 'Past infection; partial immunity (may wane)'),
('HEV RNA + (immunocompromised)', 'CHRONIC HEV — start ribavirin'),
('Both negative', 'Susceptible — no prior exposure'),
]
for ri3, (mark3, interp3) in enumerate(hev_rows):
ry3 = 0.225 - ri3 * 0.055
rbox3 = FancyBboxPatch((0.005, ry3 - 0.035), 0.99, 0.038,
boxstyle="round,pad=0,rounding_size=0.01",
facecolor='#1A1500' if ri3 % 2 == 0 else '#0F2030',
edgecolor='none', transform=ax_hav_sero.transAxes, zorder=2)
ax_hav_sero.add_patch(rbox3)
ax_hav_sero.text(0.28, ry3 - 0.016, mark3, ha='center', va='center',
fontsize=7, color=HEV_C, fontweight='bold',
transform=ax_hav_sero.transAxes, zorder=3)
ax_hav_sero.text(0.70, ry3 - 0.016, interp3, ha='center', va='center',
fontsize=7, color=CREAM, transform=ax_hav_sero.transAxes, zorder=3)
# HDV patterns panel
ax_hdv = fig.add_subplot(gs[6, 3:])
add_panel(ax_hdv, 'HDV CO-INFECTION vs. SUPERINFECTION + HIGH-YIELD PEARLS', PURPLE)
# Co vs Super table
ax_hdv.text(0.01, 0.93, 'HDV Co-infection vs Superinfection', fontsize=8, fontweight='bold',
color=PURPLE, transform=ax_hdv.transAxes)
hdv_cols = ['Feature', 'Co-infection', 'Superinfection']
hdv_rows_d = [
('Definition', 'HBV + HDV at same time', 'HDV in chronic HBV carrier'),
('Anti-HBc IgM', 'POSITIVE', 'Negative'),
('HBsAg', 'Positive', 'Positive'),
('Anti-HDV IgM', 'Positive (transient)', 'Positive (persists)'),
('Chronicity', 'Low (~5%)', '>80% — often severe'),
('Severity', 'Moderate; bimodal ALT peaks', 'SEVERE / fulminant'),
('Outcome', 'Usually resolves', 'Often cirrhosis / HCC'),
]
hx = [0.01, 0.36, 0.67]
hw = [0.33, 0.30, 0.32]
hy_start = 0.875
hrow_h = 0.073
for ci, (hd, xh, wh) in enumerate(zip(hdv_cols, hx, hw)):
hb = FancyBboxPatch((xh, hy_start - 0.038), wh - 0.005, 0.038,
boxstyle="round,pad=0,rounding_size=0.008",
facecolor=PURPLE if ci == 0 else (colors.to_rgba(HBV_C) if ci==1 else colors.to_rgba(RED)),
edgecolor='none', transform=ax_hdv.transAxes, zorder=3)
ax_hdv.add_patch(hb)
ax_hdv.text(xh + wh/2 - 0.003, hy_start - 0.019, hd, ha='center', va='center',
fontsize=7.5, fontweight='bold', color='#0D1B2A',
transform=ax_hdv.transAxes, zorder=4)
import matplotlib.colors as mcolors
def to_hex_approx(c):
return mcolors.to_hex(c)
for ri, (feat, co, su) in enumerate(hdv_rows_d):
ry_hdv = hy_start - 0.042 - ri * hrow_h - 0.002
bg_hdv = '#0D2040' if ri % 2 == 0 else '#0A1A30'
if 'SEVERE' in su or '>80%' in su:
bg_hdv = '#2D0A0A'
rb_hdv = FancyBboxPatch((0.01, ry_hdv - 0.048), 0.98, 0.048,
boxstyle="round,pad=0,rounding_size=0.007",
facecolor=bg_hdv, edgecolor='none',
transform=ax_hdv.transAxes, zorder=2)
ax_hdv.add_patch(rb_hdv)
for ci2, (val, xh2, wh2) in enumerate(zip([feat, co, su], hx, hw)):
tc2 = SLATE if ci2 == 0 else (RED if ('SEVERE' in val or '>80%' in val or 'POSITIVE' in val.upper()) else CREAM)
fw2 = 'bold' if ci2 == 0 or 'SEVERE' in val or '>80%' in val else 'normal'
ax_hdv.text(xh2 + wh2/2 - 0.003, ry_hdv - 0.024, val,
ha='center', va='center', fontsize=7, color=tc2, fontweight=fw2,
transform=ax_hdv.transAxes, zorder=3, multialignment='center')
# ═══════════════════════════════════════════════════════════════════════════════
# ROW 7 — HIGH-YIELD PEARLS (full width)
# ═══════════════════════════════════════════════════════════════════════════════
ax_pearls = fig.add_subplot(gs[7, :])
ax_pearls.set_facecolor('#061120')
ax_pearls.set_xlim(0, 1); ax_pearls.set_ylim(0, 1); ax_pearls.axis('off')
ax_pearls.text(0.5, 0.96, 'HIGH-YIELD CLINICAL PEARLS & EXAM FACTS',
ha='center', va='top', fontsize=9.5, fontweight='bold',
color=GOLD, transform=ax_pearls.transAxes)
pearls = [
('Only DNA hepatitis virus', 'HBV', HBV_C),
('Fecal-oral viruses', 'HAV & HEV', HAV_C),
('No carrier state', 'HAV & HEV\n(normal hosts)', TEAL),
('Worst in pregnancy', 'HEV → 20% mortality', HEV_C),
('Needs HBV to replicate', 'HDV', PURPLE),
('Highest chronicity', 'HCV: 70–85%', HCV_C),
('Smallest human DNA virus', 'HBV (~3,200 bp)', GREEN),
('Reverse transcriptase', 'HBV (unique DNA virus)', BLUE),
('Window period marker', 'Anti-HBc IgM only', RED),
('Vaccination → Anti-HBs only', 'Natural inf. → Anti-HBs + Anti-HBc IgG', YELLOW),
('Bimodal ALT peaks', 'HDV co-infection', PINK),
('No protective antibody after cure', 'HCV — reinfection possible', ORANGE),
]
pearl_w = 1.0 / 6
pearl_h = 0.36
pearl_x_list = [i * pearl_w for i in range(6)]
pearl_y_list = [0.60, 0.18]
for pi, (question, answer, pc) in enumerate(pearls):
row_pi = pi // 6
col_pi = pi % 6
px_p = pearl_x_list[col_pi] + 0.005
py_p = pearl_y_list[row_pi]
pw_p = pearl_w - 0.01
pb_p = FancyBboxPatch((px_p, py_p - 0.01), pw_p, pearl_h,
boxstyle="round,pad=0,rounding_size=0.025",
facecolor=CARD_BG, edgecolor=pc, linewidth=1.2,
transform=ax_pearls.transAxes, zorder=2)
ax_pearls.add_patch(pb_p)
stripe_p = FancyBboxPatch((px_p, py_p + pearl_h - 0.11), pw_p, 0.11,
boxstyle="round,pad=0,rounding_size=0",
facecolor=pc, edgecolor='none', alpha=0.25,
transform=ax_pearls.transAxes, zorder=3)
ax_pearls.add_patch(stripe_p)
ax_pearls.text(px_p + pw_p/2, py_p + pearl_h - 0.055, question,
ha='center', va='center', fontsize=6.8, color=CREAM,
transform=ax_pearls.transAxes, zorder=4, multialignment='center',
linespacing=1.3)
ax_pearls.text(px_p + pw_p/2, py_p + pearl_h * 0.3, answer,
ha='center', va='center', fontsize=8, color=pc,
fontweight='bold', transform=ax_pearls.transAxes, zorder=4,
multialignment='center', linespacing=1.3)
plt.savefig('/home/daytona/workspace/hepatitis-guide/Hepatitis_Comprehensive_Diagram.png',
dpi=180, bbox_inches='tight', facecolor=BG, edgecolor='none')
print("Diagram saved successfully.")
cd /home/daytona/workspace/hepatitis-guide && python generate_diagram.py 2>&1
~/hepatitis-guide/generate_diagram.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/hepatitis-guide/generate_diagram.py'
cd /home/daytona/workspace/hepatitis-guide && python generate_diagram.py 2>&1
~/hepatitis-guide/generate_diagram.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/hepatitis-guide/generate_diagram.py'
cd /home/daytona/workspace/hepatitis-guide && python generate_diagram.py 2>&1
grep -n "axhline\|axvline" /home/daytona/workspace/hepatitis-guide/generate_diagram.py
~/hepatitis-guide/generate_diagram.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/hepatitis-guide/generate_diagram.py'
cd /home/daytona/workspace/hepatitis-guide && python generate_diagram.py 2>&1
~/hepatitis-guide/generate_diagram.py
Error: String not found in file: ' facecolor=PURPLE if ci == 0 else (colors.to_rgba(HBV_C) if ci==1 else colors.to_rgba(RED)),'
~/hepatitis-guide/generate_diagram.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/hepatitis-guide/generate_diagram.py'
cd /home/daytona/workspace/hepatitis-guide && python generate_diagram.py 2>&1
ls -lh /home/daytona/workspace/hepatitis-guide/Hepatitis_Comprehensive_Diagram.png
Hepatitis Comprehensive Diagram
Image · PNG
| Row | Section | Content |
|---|---|---|
| Title | Header bar | Full title + source references |
| Row 1 | Virus identity cards (x5) | One card per virus - structure, transmission, outcome |
| Row 2 | Comparison table | All 5 viruses across 12 features side by side |
| Row 3L | HBV serology markers | All 7 markers explained + 6-pattern interpretation table |
| Row 3R | Pathogenesis | Per-virus mechanism of liver damage |
| Row 4L | Transmission matrix | 5 routes × 5 viruses with checkmarks |
| Row 4R | Clinical features | 4 phases of acute hepatitis + lab findings + complications |
| Row 5L | HBV timeline | Acute vs. chronic serological curves (window period annotated) |
| Row 5R | Treatment | Per-virus treatment and prophylaxis with drug names |
| Row 6L | HAV / HCV / HEV serology | Pattern tables + HCV testing algorithm |
| Row 6R | HDV co-infection vs superinfection | 7-feature comparison table |
| Row 7 | 12 Clinical pearls | Colour-coded exam fact cards |