Pulmonary tuberculosis
Reading File
Finding Sources
Searching PubMed
"pulmonary tuberculosis"[MeSH Terms] AND "diagnosis AND treatment"
Reading File
Reading File
Searching PubMed
"tuberculosis"[MeSH Terms] AND "treatment"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information to provide a thorough answer on pulmonary tuberculosis. Let me compose the full response.
Pulmonary Tuberculosis
Overview
Pulmonary tuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis, a slow-growing, obligate aerobic, acid-fast bacillus. It remains one of the leading infectious disease killers globally, primarily affecting the lungs but capable of disseminating to nearly any organ system. TB occurs in two main forms: latent TB infection (LTBI) and active TB disease.
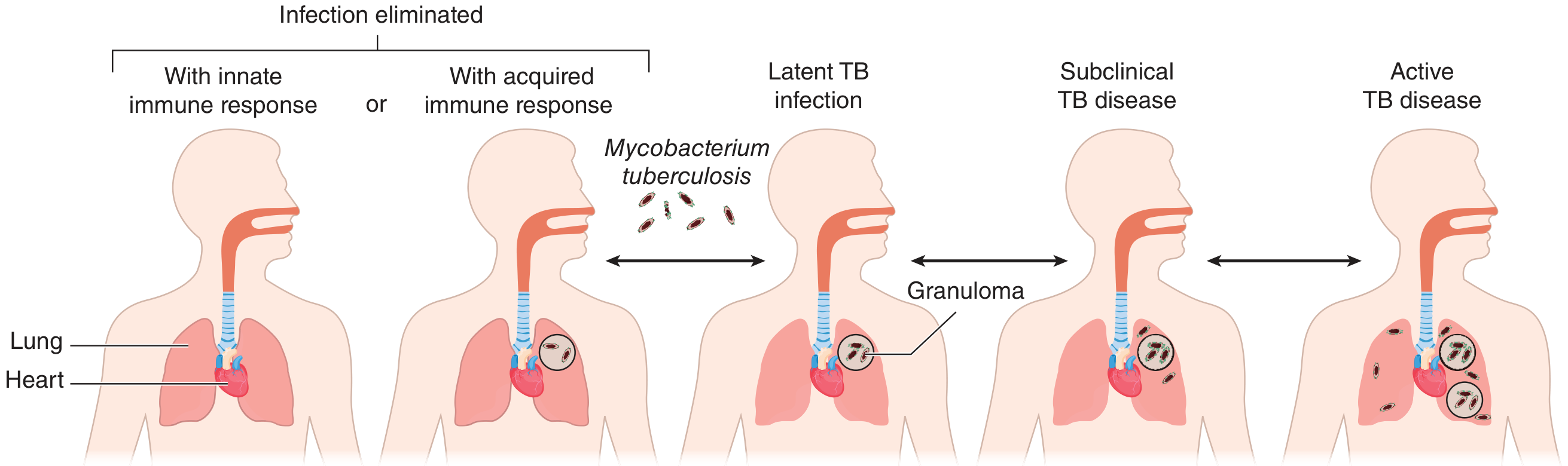
Spectrum of TB Infection
After inhaling M. tuberculosis, several outcomes are possible depending on the host immune response:
| State | TST/IGRA | Culture | Smear | Symptoms | Treatment |
|---|---|---|---|---|---|
| No infection | Negative | Negative | Negative | None | None |
| Latent TB infection | Positive | Negative | Negative | None | Preventive therapy |
| Subclinical TB | Positive | Intermittently + | Usually - | Mild/none | Multidrug therapy |
| Active TB disease | Usually + | Positive | + or - | Mild to severe | Multidrug therapy |
Pathogenesis
- Inhalation - Droplet nuclei carrying M. tuberculosis are inhaled and reach the alveoli.
- Macrophage uptake - Alveolar macrophages phagocytose the bacilli, but the organism resists intracellular killing by inhibiting phagosome-lysosome fusion.
- Granuloma formation - T-cell mediated immunity triggers formation of granulomas (caseating necrosis at center, surrounded by epithelioid macrophages, Langhans giant cells, and lymphocytes). This is the hallmark lesion - the tubercle.
- Ghon focus - The primary parenchymal lesion, typically in the lower/middle lung zones where ventilation is highest.
- Ghon complex - Ghon focus + ipsilateral hilar lymph node enlargement.
- Reactivation - If cell-mediated immunity wanes (HIV, malnutrition, diabetes, TNF-alpha inhibitors, aging), dormant organisms reactivate, typically in the upper lobes (high oxygen tension).
Clinical Features
Symptoms
Active pulmonary TB commonly presents with:
- Cough (most common symptom - productive or dry; up to 25% of culture-confirmed cases have no cough)
- Fever and night sweats
- Weight loss and anorexia
- Fatigue and malaise
- Hemoptysis - occurs with more extensive or cavitary disease; may also result from a Rasmussen aneurysm (dilated vessel in an old cavity wall) or aspergilloma in a residual cavity
Physical Examination
Findings are non-specific and may include:
- Post-tussive rales in the upper lung zones
- Amphoric breath sounds (suggesting a cavity)
- Lymphadenopathy (more common in HIV-infected patients)
- Laboratory: leukocytosis and anemia may be present
Disease Classification
- Progressive primary TB - Active disease occurring within the first year of initial infection
- Reactivation (post-primary) TB - Disease arising from dormant organisms, typically in the apical-posterior segments of upper lobes
Radiology
Chest X-ray and CT Findings
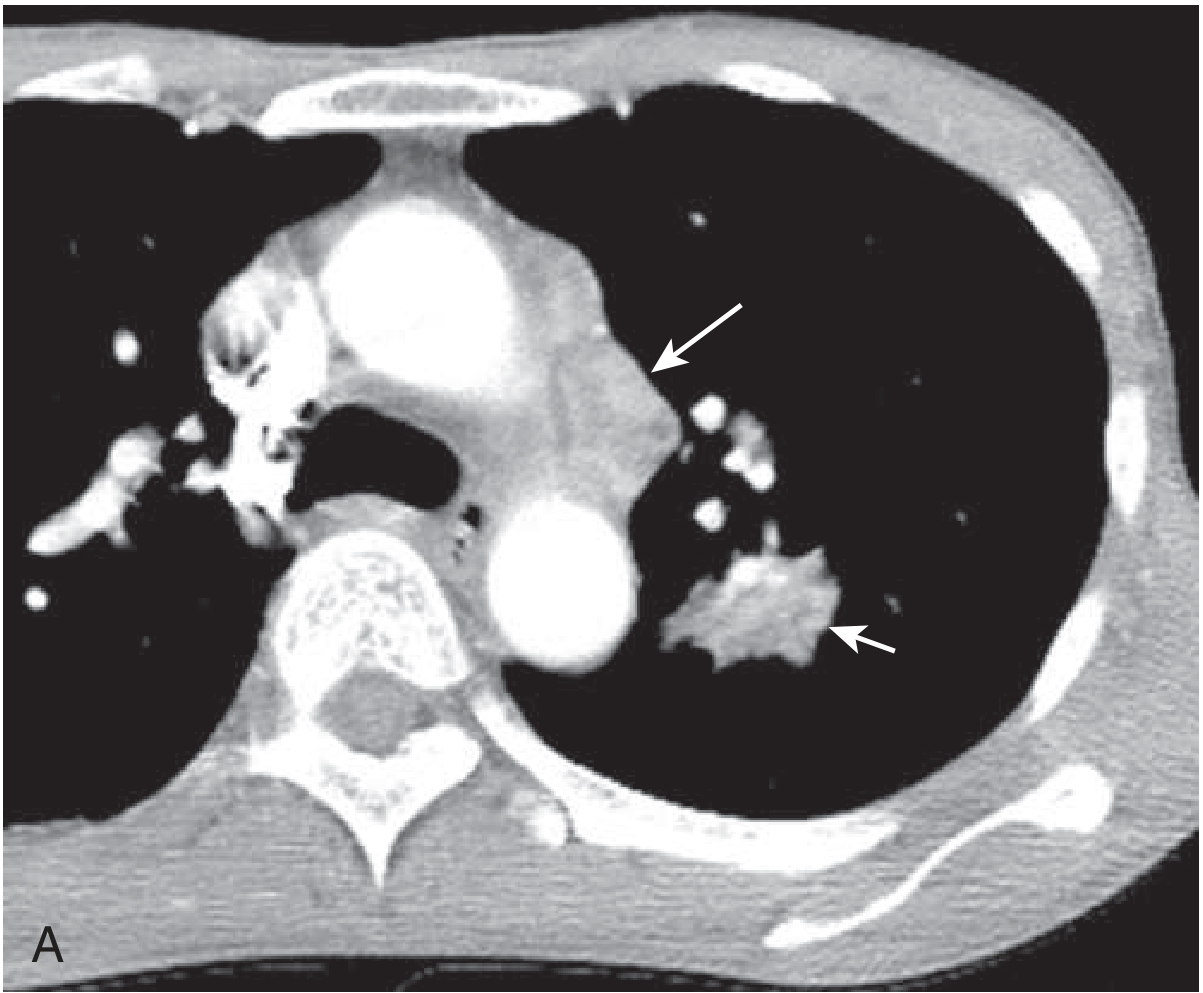
- Primary TB: Middle/lower zone infiltrates, hilar lymphadenopathy (Ghon complex), pleural effusion
- Reactivation TB: Upper lobe infiltrates, cavitation (apical-posterior segments), fibrosis, calcified nodules
- Miliary TB: Diffuse 1-2 mm nodules throughout both lung fields (classic "millet seed" pattern, seen in ~85%)
- Cavitation indicates high bacillary burden and increased infectivity
CT chest showing primary TB with mediastinal lymphadenopathy and parenchymal infiltrate:
TB in HIV-Infected Patients
- Manifestations depend on degree of immune dysfunction
- Less likely to be smear-positive or have cavitary disease
- More likely to develop disseminated infection
- May have normal chest X-ray despite smear-positive disease - CT is more sensitive
- In advanced AIDS with miliary TB, blood cultures may be positive in 20-40% of cases
Extrapulmonary Manifestations
Pleural TB
- Occurs 3-6 months after primary infection
- Exudative unilateral pleural effusion
- Cough, pleuritic chest pain, systemic symptoms
Miliary TB
- 1-2 mm granulomatous nodules in lungs, liver, bone marrow, kidneys, adrenal glands, spleen
- Choroidal tubercles on fundoscopy (pathognomonic when seen)
- Fever, weight loss, night sweats without localizing symptoms
Diagnosis
1. Sputum Examination
- At least two sputum specimens for AFB smear + mycobacterial culture (three is standard in the US)
- At least one specimen for Nucleic Acid Amplification Testing (NAAT)
AFB Smear Microscopy: Quick and inexpensive but sensitivity is only ~50-80% in pulmonary TB; does not distinguish M. tuberculosis from NTM.
Mycobacterial Culture: Gold standard for definitive diagnosis; takes 2-6 weeks for solid media, 1-3 weeks for liquid (BACTEC).
2. Nucleic Acid Amplification Testing (NAAT)
- Xpert MTB/RIF (GeneXpert): Automated, self-contained real-time PCR that simultaneously detects M. tuberculosis DNA and rifampin resistance in 90 minutes
- WHO-recommended as the preferred initial test for HIV-infected patients, suspected drug-resistant TB, and seriously ill patients
- Sensitivity ~89% for smear-positive, ~67% for smear-negative pulmonary TB
- A negative NAAT does not exclude active disease - culture is still required in smear-negative suspects
NAAT result interpretation:
- Smear-positive + NAAT-positive: Rapid confirmation of TB
- Smear-positive + NAAT-negative: Suggests NTM (not TB)
- Smear-negative + NAAT-positive (intermediate-high clinical probability): Presumptive TB
- Smear-negative + NAAT-negative: Does not exclude TB; culture still required
3. Testing for Latent TB Infection (LTBI)
Tuberculin Skin Test (TST/Mantoux):
- Intradermal injection of 5 tuberculin units PPD; read at 48-72 hours
- Cut-points for positivity based on risk:
- ≥5 mm: HIV infection, close contacts of active TB, organ transplant/immunosuppressed, fibrotic changes on CXR
- ≥10 mm: Recent immigrants from high-incidence countries, injection drug users, healthcare workers, prisoners, clinical conditions (diabetes, silicosis, CKD)
- ≥15 mm: Low-risk persons
- Limitations: False-positive with BCG vaccination or NTM exposure; false-negative in immunosuppressed patients; booster phenomenon with serial testing
Interferon-Gamma Release Assays (IGRA):
- QuantiFERON-TB Gold Plus and T-SPOT.TB
- Blood-based; measures IFN-γ release in response to TB-specific antigens (ESAT-6, CFP-10)
- Preferred over TST in persons with BCG vaccination history
- Not affected by BCG; more specific than TST
When to screen for LTBI:
- Birth/residence in high-incidence country (>10/100,000/year)
- Close contact with infectious TB case
- HIV infection
- Planned immunosuppression (organ transplant, TNF-alpha antagonists, corticosteroids ≥15 mg/day for ≥1 month)
- Homelessness, incarceration, healthcare workers
Treatment
Infectivity and Isolation
Pulmonary TB patients are considered infectious until they have had:
- At least 2 weeks of therapy
- Clinical improvement (reduced cough, weight gain, fever resolution)
- No detectable AFB on three sputum specimens at least 8 hours apart
Drug-Susceptible TB (Standard Regimen)
Total duration: 6 months (for most cases)
| Phase | Duration | Drugs |
|---|---|---|
| Intensive phase | 8 weeks (2 months) | Isoniazid (H) + Rifampin (R) + Pyrazinamide (Z) + Ethambutol (E) |
| Continuation phase | 16 weeks (4 months) | Isoniazid (H) + Rifampin (R) |
Mnemonic: 2HRZE / 4HR
If cavitary disease + positive sputum culture at 2 months → extend continuation phase to 7 months (total 9 months)
First-Line Drug Doses (Adults)
| Drug | Daily Dose | Thrice-Weekly Dose |
|---|---|---|
| Isoniazid | 5 mg/kg (typically 300 mg) | 15 mg/kg (typically 900 mg) |
| Rifampin | 10 mg/kg (typically 600 mg) | 10 mg/kg (typically 600 mg) |
| Pyrazinamide | Weight-based (1000-2000 mg) | Weight-based |
| Ethambutol | Weight-based (800-1600 mg) | Weight-based |
Important Ancillary Points
- Pyridoxine (Vitamin B6) 25-50 mg/day should be given with isoniazid to prevent peripheral neuropathy (especially in diabetics, alcoholics, HIV-positive, pregnant women, malnourished patients)
- Rifampin: potent CYP inducer - significant drug interactions (oral contraceptives, anticoagulants, antiretrovirals)
- Ethambutol: causes dose-dependent optic neuritis - baseline and monthly visual acuity/color vision testing required
- Pyrazinamide: causes hyperuricemia and hepatotoxicity; avoid in severe hepatic disease
- Drug susceptibility testing should be performed on all isolates
Follow-Up
- Monthly clinical assessment + sputum examination until two consecutive negative cultures
- 75-80% of pulmonary TB patients are sputum culture-negative by 2 months
- ~95% are culture-negative by 3 months
- Positive culture at 4 months = treatment failure (rare in properly treated drug-sensitive disease) - prompts expert consultation
- Never add a single drug to a failing regimen - this promotes further resistance
Latent TB Infection (LTBI) Treatment Regimens
| Regimen | Duration | Drugs |
|---|---|---|
| 3HP (preferred) | 3 months | Isoniazid + Rifapentine (weekly) |
| 4R | 4 months | Rifampin (daily) |
| 6H | 6 months | Isoniazid (daily) |
| 9H | 9 months | Isoniazid (daily) |
Drug-Resistant TB
Definitions
| Category | Definition |
|---|---|
| MDR-TB (Multi-drug resistant) | Resistant to at least isoniazid AND rifampin |
| XDR-TB (Extensively drug resistant) | MDR-TB + resistant to any fluoroquinolone + at least one injectable drug (amikacin, kanamycin, or capreomycin) |
| Pre-XDR TB (revised 2021 WHO definition) | MDR/RR-TB + resistant to any fluoroquinolone |
- Rifampin resistance on Xpert MTB/RIF strongly correlates with MDR-TB
- MDR-TB and XDR-TB require longer regimens (18-24+ months) using second-line drugs including bedaquiline, linezolid, clofazimine, cycloserine, delamanid, and pretomanid
Complications
- Massive hemoptysis (Rasmussen aneurysm rupture)
- Pneumothorax (from subpleural cavity rupture)
- Aspergilloma (fungus ball in old residual cavity)
- Bronchiectasis (from fibrosis and airway distortion)
- Cor pulmonale (from extensive pulmonary fibrosis)
- Disseminated/miliary TB (hematogenous spread)
- ARDS (in severe disease)
Public Health Considerations
- TB is a notifiable disease - local health departments must be notified
- Contact tracing and testing of close contacts is mandatory
- Directly Observed Therapy (DOT) is the standard of care to ensure adherence
- In the US, expert guidance is available through the 4 regional TB Centers of Excellence (CDC-funded) covering all 50 states
Sources: Goldman-Cecil Medicine, International Edition; Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume; Tietz Textbook of Laboratory Medicine, 7th Edition
This is a shared conversation. Sign in to Orris to start your own chat.