Explain me 10 common heart diseases with ECG changes and ECG images of those diseases
Reading File
Finding Sources
Finding Sources
Searching the Web
common heart diseases ECG changes findings with ECG images cardiology
Finding Sources
Finding Sources
Finding Sources
Searching the Web
ECG images STEMI atrial fibrillation heart block WPW hypertrophic cardiomyopathy pericarditis ECG findings
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
ECG images atrial fibrillation ventricular tachycardia pericarditis WPW syndrome heart failure LVH site:litfl.com OR site:ecgwaves.com
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading Web Page
https://litfl.com/atrial-fibrillation-ecg-library
Searching the Web
ECG images ventricular tachycardia left ventricular hypertrophy bundle branch block Wolff Parkinson White site:litfl.com
Loading Image
Loading Image
Loading Image
I now have excellent ECG images and comprehensive information. Let me compile the full answer with all 10 heart diseases, their ECG changes, and the images from the textbooks.
10 Common Heart Diseases: ECG Changes with Images
1. ST-Elevation Myocardial Infarction (STEMI)
What it is: Acute occlusion of a coronary artery causing full-thickness myocardial necrosis.
ECG Changes:
- ST-segment elevation ≥1 mm in ≥2 contiguous limb leads, or ≥2 mm in ≥2 contiguous precordial leads
- Hyperacute T waves (tall, peaked) in the very early phase
- Q waves (pathological) develop within hours - indicating necrosis
- Reciprocal ST depression in mirror leads
- T-wave inversion in later stages
Regional localisation (from Rosen's Emergency Medicine):
| Territory | Leads with STE | Culprit Artery |
|---|---|---|
| Anterior | V1-V4 | LAD |
| Anterolateral | V2-V6, I, aVL | LAD / diagonal |
| Inferior | II, III, aVF | RCA / LCx |
| Lateral | I, aVL, V5-V6 | LCx |
| Posterior | V8-V9 (elevation); V1-V3 (depression) | RCA / LCx |
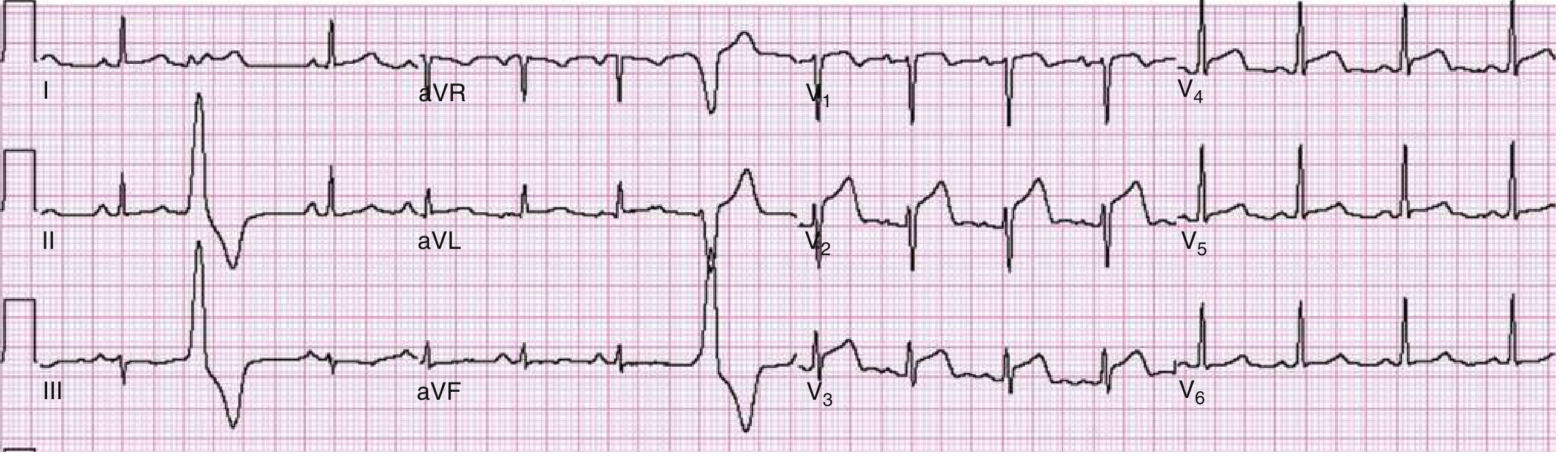
ECG - Anterior Wall STEMI (ST elevation V1-V4, Rosen's Emergency Medicine):
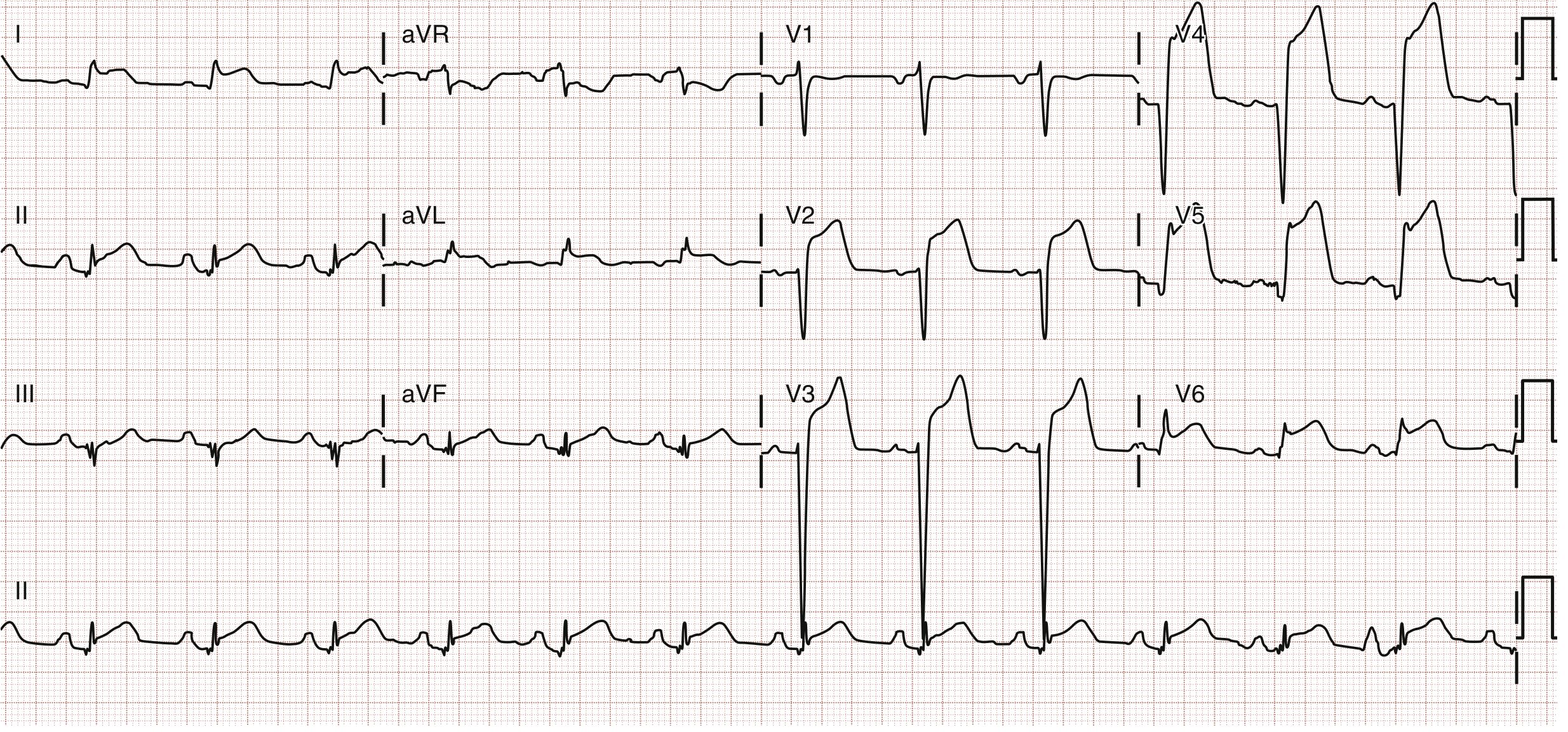
ECG - Anterolateral STEMI (STE in V2-V6, I, aVL - in-stent thrombosis):
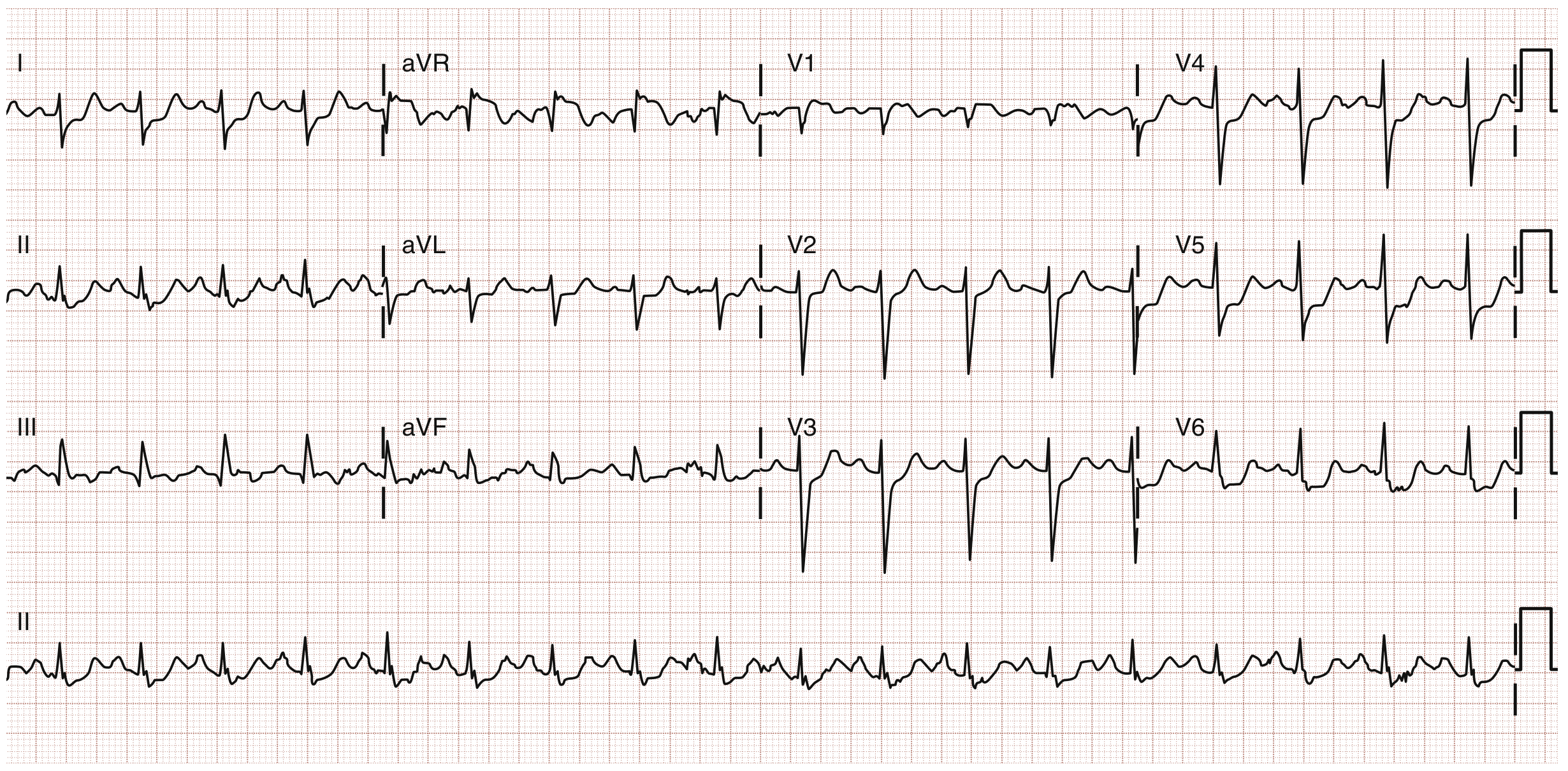
ECG - Left Main / aVR STE (ST elevation in aVR with widespread depression elsewhere):
Source: Rosen's Emergency Medicine, 10e
2. Atrial Fibrillation (AF)
What it is: The most common sustained cardiac arrhythmia, caused by multiple disorganized electrical wavelets in the atria, producing chaotic atrial activity with no coordinated contraction. Risk factors include hypertension, older age, valvular disease, and heart failure.
ECG Changes (Guyton & Hall, Frameworks for Internal Medicine):
- Absent P waves - replaced by fine, irregular fibrillatory (f) waves at 350-600/min
- Irregularly irregular R-R intervals - the hallmark finding
- Narrow QRS complexes (unless aberrant conduction)
- Ventricular rate typically 100-160 bpm when uncontrolled
- Baseline appears chaotic/undulating rather than flat
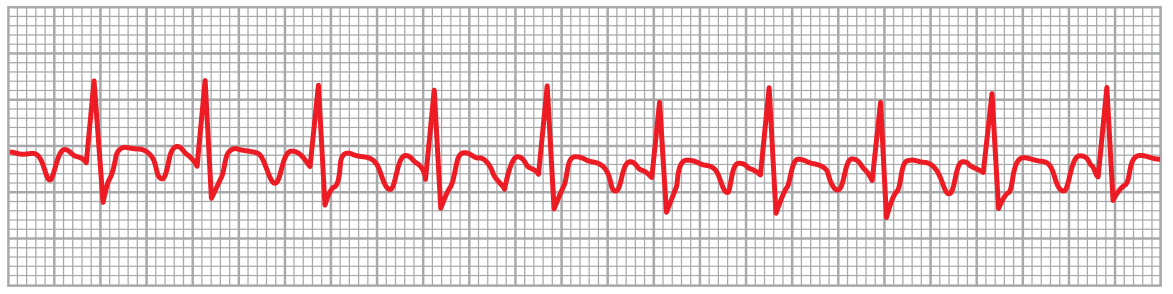
ECG - Atrial Fibrillation (Lead II - note absent P waves, irregular QRS spacing):

Source: Guyton and Hall Textbook of Medical Physiology, Frameworks for Internal Medicine
3. Atrial Flutter
What it is: A macro-reentrant arrhythmia in which a single large electrical wavefront circulates around the tricuspid annulus at 250-350/min.
ECG Changes:
- Sawtooth flutter waves (F waves) at ~300/min, best seen in leads II, III, aVF, and V1
- Regular atrial rate (unlike AF) - typically 300/min
- Variable ventricular rate depending on AV conduction ratio (usually 2:1 = 150 bpm, or 3:1, 4:1)
- No discrete P waves
- Regular ventricular rhythm in fixed conduction ratios, irregular in variable ratios
ECG - Atrial Flutter (from Guyton & Hall - sawtooth F waves visible):
Source: Guyton and Hall Textbook of Medical Physiology
4. AV Block (Heart Block)
What it is: Impaired conduction at the AV node or His-Purkinje system, ranging from prolonged conduction to complete dissociation.
ECG Changes (Harrison's, Washington Manual, Goldman-Cecil):
| Type | ECG Finding |
|---|---|
| 1st degree | PR interval >200 ms (>5 small squares); every P conducts |
| 2nd degree Mobitz I (Wenckebach) | Progressive PR prolongation → dropped QRS; then cycle repeats |
| 2nd degree Mobitz II | Fixed PR interval with sudden non-conducted P waves; wide QRS |
| 3rd degree (complete) | Complete AV dissociation - P waves and QRS complexes are independent; escape rhythm (junctional at 40-60/min or ventricular at 20-40/min) |
- Complete heart block shows AV dissociation with slow, wide ventricular escape rhythm
- Mobitz II has a higher risk of progression to complete block
Source: Harrison's Principles of Internal Medicine 22E, Washington Manual of Medical Therapeutics
5. Ventricular Tachycardia (VT)
What it is: A potentially life-threatening arrhythmia arising from ventricular ectopic foci, typically seen in the context of ischemic heart disease or cardiomyopathy.
ECG Changes:
- Wide QRS complexes (≥120 ms / 3 small squares)
- Rate 100-250 bpm, regular or slightly irregular
- AV dissociation - P waves march through independently (when visible)
- Concordance across precordial leads (all positive or all negative)
- Capture beats and fusion beats (pathognomonic when present)
- Axis deviation (often extreme left or right)
- Morphology criteria: LBBB or RBBB pattern with atypical features
Distinguishing VT from SVT with aberrancy: AV dissociation, fusion beats, and concordance all favor VT.
Source: Tintinalli's Emergency Medicine, Braunwald's Heart Disease
6. Wolff-Parkinson-White (WPW) Syndrome
What it is: A pre-excitation syndrome caused by an accessory pathway (Bundle of Kent) between atria and ventricles that bypasses the AV node, allowing early ventricular depolarization.
ECG Changes (Tintinalli's Emergency Medicine):
- Short PR interval (<120 ms / 3 small squares) - because conduction bypasses the slow AV node
- Delta wave - slurred upstroke at the start of the QRS (initial slow conduction through myocardium before normal His-Purkinje takes over)
- Wide QRS complex (≥120 ms) due to fusion of accessory and normal conduction
- Secondary ST-T changes (discordant to QRS)
- In AF with WPW: irregular, very rapid wide-complex rhythm (life-threatening - can degenerate to VF)
ECG - WPW with delta waves and Wolff-Parkinson-White pattern (note visible delta wave slurring on the QRS upstroke):

Source: Tintinalli's Emergency Medicine, Cleveland Clinic Journal of Medicine
7. Left Ventricular Hypertrophy (LVH)
What it is: Increased left ventricular wall thickness, most commonly from chronic hypertension or aortic stenosis.
ECG Changes:
- High QRS voltage (Sokolow-Lyon criterion: S in V1 + R in V5 or V6 ≥35 mm; or Cornell criterion: R in aVL + S in V3 ≥28 mm in men, ≥20 mm in women)
- Tall R waves in left precordial leads (V5-V6) and lateral limb leads (I, aVL)
- Deep S waves in right precordial leads (V1-V2)
- Left axis deviation
- LV strain pattern: asymmetric ST depression and T-wave inversion in V5-V6, I, aVL (the "strain" pattern)
- Left atrial enlargement often coexists (broad, notched P waves in II; biphasic P in V1)
Source: Goldman-Cecil Medicine, Harrison's Principles of Internal Medicine 22E
8. Right Heart Strain / Pulmonary Embolism (PE)
What it is: Acute or chronic right ventricular pressure overload, classically from massive pulmonary embolism.
ECG Changes:
- Classic S1Q3T3 pattern: S wave in lead I, Q wave and T-wave inversion in lead III
- Right axis deviation
- New RBBB (right bundle branch block) pattern - wide QRS with RSR' in V1
- Sinus tachycardia (most common finding in PE overall)
- T-wave inversions in V1-V4 (right precordial leads)
- P pulmonale: tall peaked P waves >2.5 mm in II, III, aVF (in chronic cor pulmonale)
Note: The ECG in PE is often non-specific. S1Q3T3 is seen in only ~20% of cases, but the combination of findings helps.
Source: Harrison's Principles, Tintinalli's Emergency Medicine
9. Acute Pericarditis
What it is: Inflammation of the pericardial sac, most commonly viral (Coxsackievirus B). Causes pleuritic chest pain that is worse lying down and relieved by sitting forward.
ECG Changes (from ecgwaves.com, Tintinalli's):
- Diffuse ST elevation in almost all leads (I, II, III, aVF, V2-V6) - concave upward ("saddle-shaped")
- PR depression (below baseline) - a hallmark finding distinguishing it from STEMI
- No reciprocal changes (unlike STEMI where mirror leads show ST depression)
- No Q waves, no T-wave inversion concurrent with ST elevation
- Sparing of aVR and V1 (or ST elevation in aVR with PR elevation - mirror change)
Distinguishing from STEMI:
- Pericarditis: diffuse elevation, concave ST, PR depression, no reciprocal changes
- STEMI: regional elevation, convex ST, reciprocal changes, Q waves
ECG Stages of pericarditis:
| Stage | Timing | ECG |
|---|---|---|
| 1 | Days 1-2 | ST elevation + PR depression |
| 2 | Days 3-7 | ST returns to baseline, T waves flatten |
| 3 | Week 2 | T-wave inversions |
| 4 | Weeks-months | Normalization |
Source: ecgwaves.com (ECG Waves), Tintinalli's Emergency Medicine
10. Dilated Cardiomyopathy (DCM)
What it is: Dilation and impaired systolic function of one or both ventricles. Causes include ischemia, viral myocarditis, alcohol, genetic factors, and idiopathic causes.
ECG Changes (Tintinalli's Emergency Medicine):
- Left bundle branch block (LBBB) - very common; broad notched QRS, RS' in V6, QS in V1
- Nonspecific ST-T changes - diffuse flattening or inversion
- Left ventricular hypertrophy voltage criteria
- Left atrial enlargement (bifid P wave)
- Pathological Q waves if ischemic etiology
- Sinus tachycardia compensatory
- Ventricular ectopy / NSVT due to myocardial scarring
- Low voltage (<5 mm in all limb leads) if associated with pericardial effusion
- Right bundle branch block (RBBB) in some cases
LBBB criteria: QRS ≥120 ms, broad notched R in I, aVL, V5-V6; absence of septal Q waves; QS or rS in V1.
Source: Tintinalli's Emergency Medicine
Quick Reference Summary Table
| # | Condition | Key ECG Feature | Rate | Rhythm |
|---|---|---|---|---|
| 1 | STEMI | ST elevation (regional) + Q waves | Variable | Regular |
| 2 | Atrial Fibrillation | No P waves, irregular RR | 100-160 | Irregularly irregular |
| 3 | Atrial Flutter | Sawtooth F waves ~300/min | 75-150 | Regular (usually) |
| 4 | AV Block | PR prolongation / dropped beats / AV dissociation | Slow | Variable |
| 5 | Ventricular Tachycardia | Wide QRS ≥120 ms, AV dissociation | 100-250 | Regular |
| 6 | WPW Syndrome | Short PR, delta wave, wide QRS | Variable | Variable |
| 7 | LVH | High voltage (S V1 + R V5 ≥35 mm), strain | Normal | Regular |
| 8 | Pulmonary Embolism | S1Q3T3, RBBB, sinus tachycardia | Fast | Regular |
| 9 | Acute Pericarditis | Diffuse ST elevation + PR depression (no reciprocal) | Normal-fast | Regular |
| 10 | Dilated Cardiomyopathy | LBBB, low voltage, nonspecific ST-T changes | Normal-fast | Regular |
Sources:
- Rosen's Emergency Medicine (10e) - STEMI ECG localisation and images
- Guyton and Hall Textbook of Medical Physiology - AF and atrial flutter ECG images
- Harrison's Principles of Internal Medicine (22E, 2025) - AV block, LVH
- Tintinalli's Emergency Medicine - VT, WPW, dilated cardiomyopathy
- Frameworks for Internal Medicine - AF differential diagnosis
- Washington Manual of Medical Therapeutics - AV conduction disturbances
- Goldman-Cecil Medicine - LVH, AV block
Explain me 10 common heart diseases with ECG changes and ECG images of those diseases
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the textbook ECG images confirmed and the clinical content. I can now write the comprehensive answer.
10 Common Heart Diseases: ECG Changes with Images
All ECG images below are sourced directly from authoritative medical textbooks in the library.
1. ST-Elevation Myocardial Infarction (STEMI)
What it is: Complete occlusion of a coronary artery producing full-thickness (transmural) myocardial injury and necrosis. The most time-critical cardiac emergency - "time is muscle."
Pathophysiology: Plaque rupture triggers thrombus formation, abruptly blocking coronary flow. Ischemia progresses from subendocardium outward ("wavefront phenomenon"), and necrosis is irreversible if untreated beyond ~6 hours.
ECG Changes (Rosen's Emergency Medicine):
| Phase | ECG Finding |
|---|---|
| Hyperacute (minutes) | Tall, peaked "hyperacute" T waves |
| Acute (hours) | ST-segment elevation ≥1 mm in ≥2 contiguous limb leads, or ≥2 mm in ≥2 contiguous precordial leads |
| Evolving (hours-days) | Pathological Q waves (>40 ms wide, >25% of R height), T-wave inversion |
| Old (weeks-months) | Persistent Q waves, T-wave inversion or resolution |
Regional Localization:
| Territory | Elevated Leads | Culprit |
|---|---|---|
| Anterior | V1-V4 | LAD |
| Anterolateral | V2-V6, I, aVL | LAD/diagonal |
| Inferior | II, III, aVF | RCA (80%) / LCx |
| Lateral | I, aVL, V5-V6 | LCx |
| Posterior | ST depression V1-V3 (mirror) | RCA/LCx |
| Left Main | ST elevation in aVR + widespread depression | LM coronary |
ECG - Anterior STEMI (ST elevation in V1-V4, 90% LAD stenosis confirmed at cath - Rosen's):
ECG - Anterolateral STEMI (STE in V2-V6, I, aVL - in-stent thrombosis - Rosen's):
ECG - Left Main Occlusion / aVR pattern (ST elevation aVR + widespread ST depression elsewhere - Rosen's):
Rosen's Emergency Medicine, 10e - Figs. 64.6, 64.7, 64.8
2. Atrial Fibrillation (AF)
What it is: The most common sustained cardiac arrhythmia. Multiple disorganized electrical wavelets fire chaotically throughout the atria at 350-600/min, producing no effective atrial contraction. Lifetime risk over age 40 is ~25%. Major complications include stroke, cardiomyopathy, and heart failure.
Pathophysiology: Triggered by ectopic foci (often from the pulmonary vein ostia) in a substrate of atrial fibrosis or dilation. The AV node acts as a gatekeeper, allowing only a fraction of impulses through - but at variable intervals.
ECG Changes (Guyton & Hall, Frameworks for Internal Medicine):
- Absent P waves - replaced by fine, chaotic fibrillatory (f) waves at 350-600/min
- Irregularly irregular R-R intervals - the defining hallmark (no two R-R intervals are the same)
- Narrow QRS unless aberrant conduction or bundle branch block coexists
- Uncontrolled ventricular rate typically 100-160 bpm
- Baseline appears undulating/fibrillatory rather than flat
ECG - Atrial Fibrillation (Lead II - Guyton & Hall Physiology. Note: absent P waves, irregular QRS spacing, undulating baseline):
Guyton and Hall Textbook of Medical Physiology - Fig. 13.20
3. Atrial Flutter
What it is: A macro-reentrant atrial arrhythmia where a single large electrical wavefront circulates continuously around the tricuspid annulus (typical flutter) at 250-350/min. More organized than AF but still causes loss of effective atrial contraction.
Pathophysiology: A stable reentry circuit in the right atrium, rotating counter-clockwise around the tricuspid valve. The AV node blocks most impulses, typically allowing 2:1 conduction (giving a ventricular rate of ~150 bpm).
ECG Changes (Guyton & Hall):
- Classic sawtooth flutter waves (F waves) at ~300/min - best seen in II, III, aVF (negative flutter waves) and V1
- No discrete P waves - replaced entirely by F waves
- Regular ventricular rate in fixed ratios (2:1, 3:1, 4:1) - e.g., 300/2 = 150 bpm at 2:1
- Narrow QRS unless aberrant conduction
- The sawtooth baseline is the key diagnostic feature
ECG - Atrial Flutter (Guyton & Hall - note irregular sawtooth F-wave pattern between QRS complexes):
Guyton and Hall Textbook of Medical Physiology
4. AV Block (Heart Block)
What it is: Impaired conduction between atria and ventricles at the AV node or His-Purkinje system. Ranges from benign conduction delay (1st degree) to life-threatening complete dissociation (3rd degree). Causes include ischemia, drugs, degenerative disease, and infection (e.g., Lyme disease).
ECG Changes (Harrison's 22E, Washington Manual):
| Type | ECG Pattern | Clinical Risk |
|---|---|---|
| 1st Degree | PR interval >200 ms (>5 small squares); every P conducts | Benign |
| 2nd Degree Mobitz I (Wenckebach) | Progressive PR prolongation until a QRS drops; cycle resets | Usually benign; within AV node |
| 2nd Degree Mobitz II | Fixed PR interval, sudden non-conducted P wave; often wide QRS | Dangerous; may progress to complete block |
| 3rd Degree (Complete) | Complete AV dissociation - independent P and QRS rates; escape rhythm (junctional 40-60/min or ventricular 20-40/min) | Life-threatening |
Key detail from Harrison's 22E: "Type II block has more serious implications, including a risk of sudden death. It is infranodal in location and associated with a less reliable escape rhythm, and thus permanent pacing is required even in the absence of symptoms."
ECG - Five Types of AV Block (Washington Manual - A: 1st degree; B: Mobitz I Wenckebach; C: Mobitz II; D: High-degree/Advanced; E: 3rd degree complete block):

Washington Manual of Medical Therapeutics - Fig. 7-5
5. Ventricular Tachycardia (VT)
What it is: A potentially lethal arrhythmia arising from a ventricular ectopic focus or reentry circuit, firing at ≥100 bpm. Most common in the setting of ischemic heart disease, cardiomyopathy, or electrolyte disturbance. Sustained VT (>30 seconds) is a medical emergency.
Pathophysiology: In ischemic heart disease, scar tissue creates slow conduction zones that support reentry circuits. The ventricle depolarizes from an abnormal site, producing a wide, bizarre QRS.
ECG Changes (Symptom to Diagnosis, Goldman-Cecil):
- Wide QRS ≥120 ms (often >160 ms)
- Rate 100-250 bpm, usually regular
- AV dissociation - P waves and QRS complexes are independent (P rate < QRS rate)
- Fusion beats - hybrid QRS between normal and VT morphology (pathognomonic)
- Capture beats - a narrow QRS appearing within VT (pathognomonic)
- Precordial concordance - all chest leads point the same direction (all positive or all negative)
- QRS duration >160 ms has LR+ of 22.9 for VT (from Symptom to Diagnosis)
Critical rule: "All wide complex tachycardias should be assumed to be VT unless there is conclusive evidence of a supraventricular tachycardia."
ECG - Ventricular Tachycardia (Symptom to Diagnosis - monomorphic VT, regular wide-complex tachycardia):
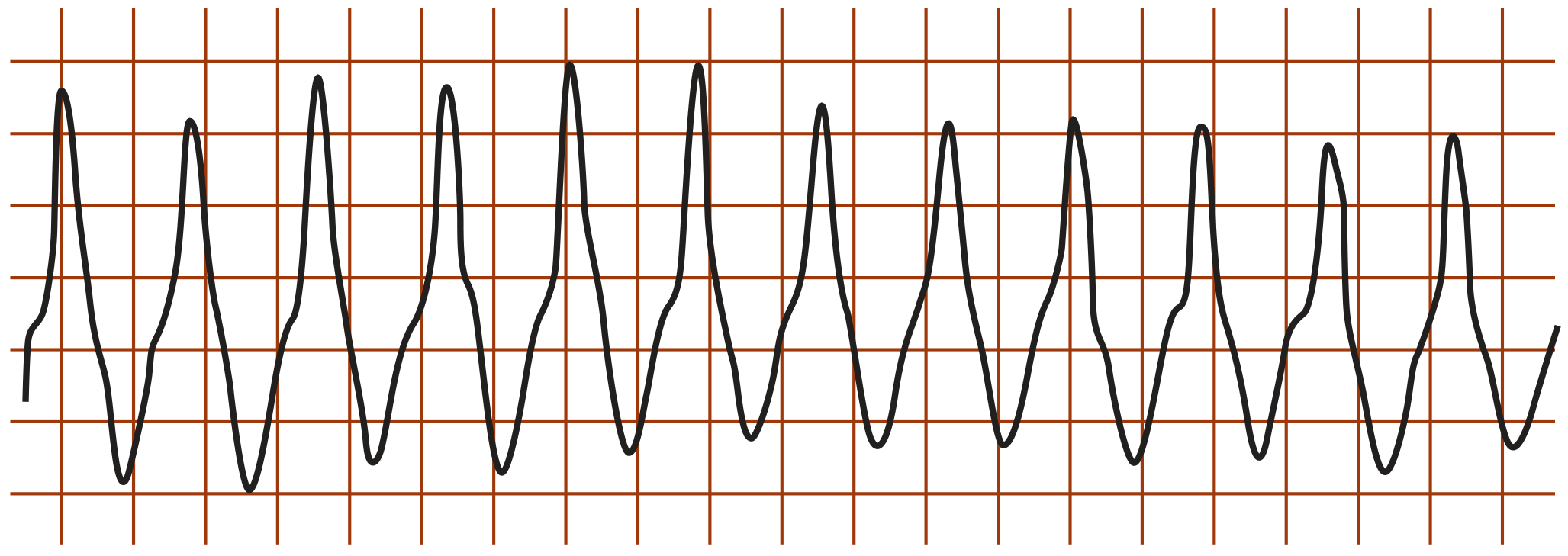
ECG - Positive Concordance in VT (Symptom to Diagnosis / LITFL - all precordial leads point upward, confirming VT):
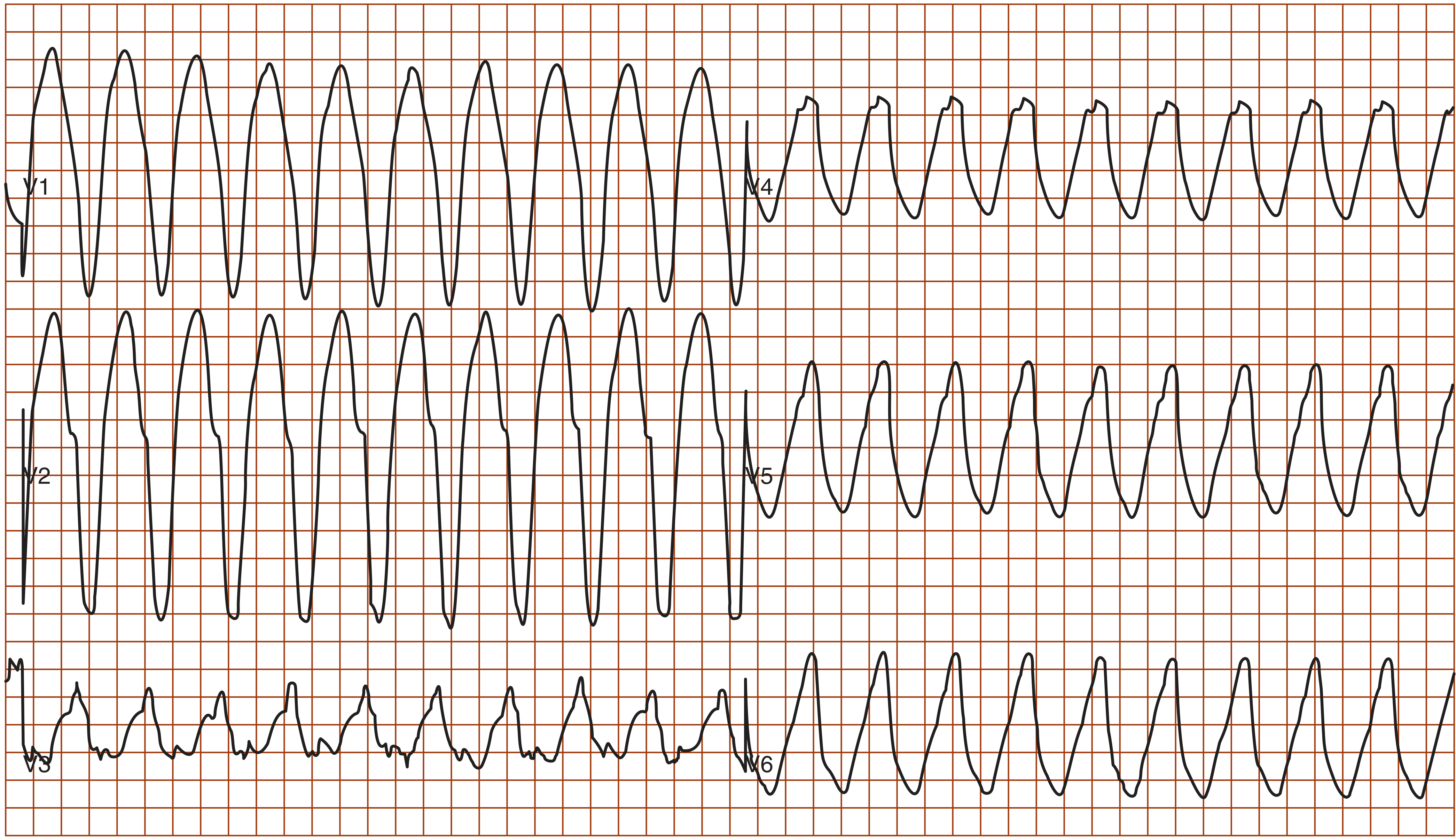
Symptom to Diagnosis, 4th Edition - Figs. 31-6 & 31-7
6. Wolff-Parkinson-White (WPW) Syndrome
What it is: A congenital pre-excitation syndrome caused by an accessory pathway (Bundle of Kent) connecting the atria and ventricles, bypassing the AV node. The ventricle gets depolarized early ("pre-excited") via this pathway. The classic presentation is episodic palpitations or SVT in a young person.
Pathophysiology: The accessory pathway conducts faster than the AV node (no intrinsic delay), so part of the ventricle depolarizes early via slow cell-to-cell conduction (producing the delta wave), and then the rest is rapidly activated through the normal His-Purkinje system (producing the narrow terminal QRS).
ECG Changes (Symptom to Diagnosis, Goldman-Cecil):
- Short PR interval (<120 ms / 3 small squares) - AV node delay bypassed
- Delta wave - slurred initial upstroke of the QRS (slow cell-to-cell conduction before His-Purkinje takes over)
- Widened QRS (≥120 ms) - fusion of accessory and normal conduction
- Secondary ST-T changes discordant to the QRS direction
- During SVT (AVRT): narrow complex regular tachycardia at 150-250 bpm
- During AF with WPW: irregular, very rapid wide-complex tachycardia - potentially fatal (can reach 300 bpm, may degenerate to VF)
ECG - WPW Syndrome (Symptom to Diagnosis - Leads I, II, V1 - note the short PR, delta wave slurring on QRS upstroke, and widened QRS):
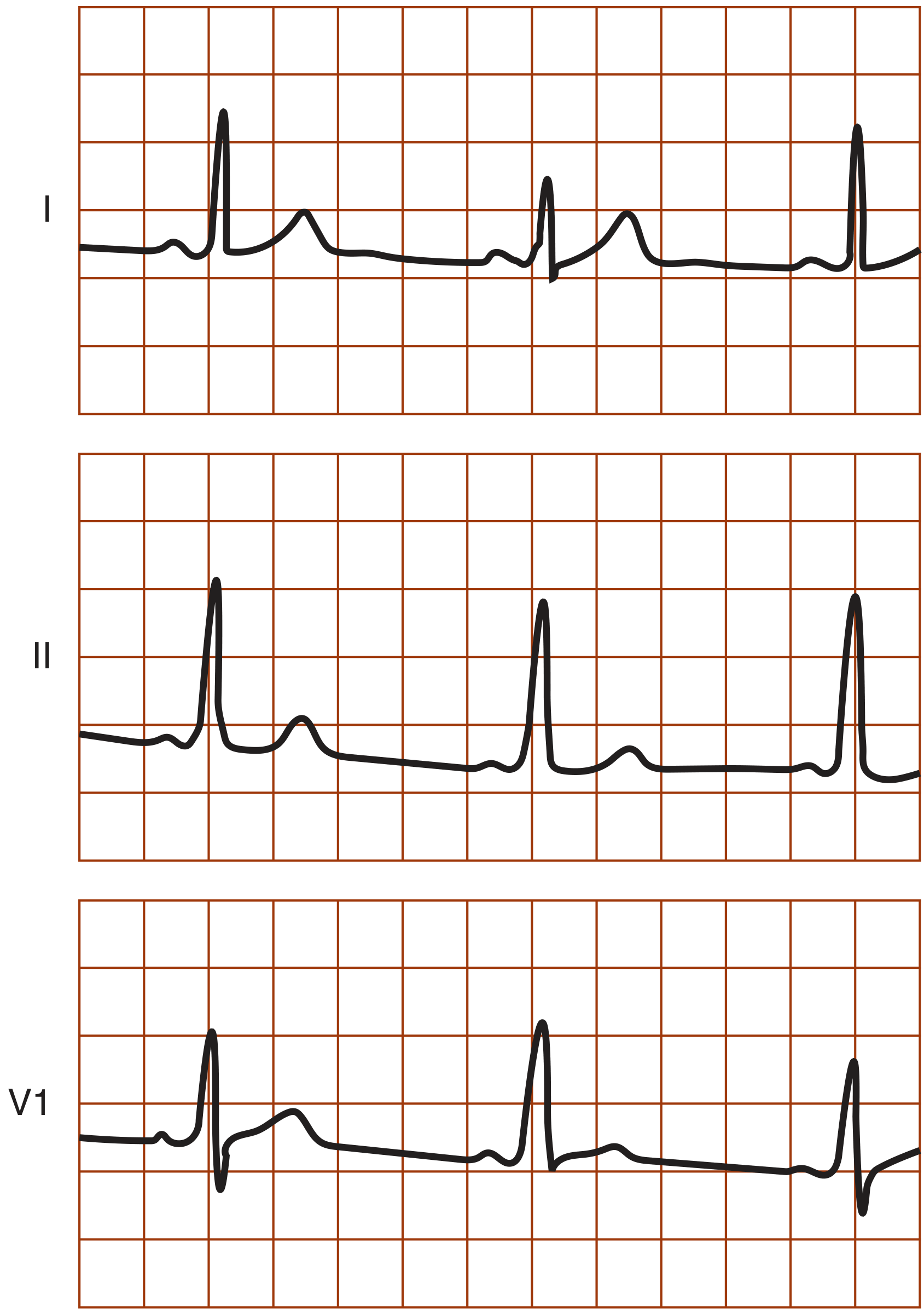
Symptom to Diagnosis, 4th Edition - Fig. 31-11 (Reproduced from Hurst's The Heart)
7. Acute Pericarditis
What it is: Inflammation of the pericardial sac, most commonly viral (Coxsackievirus B, Echovirus). Presents with sharp, pleuritic chest pain that is worse lying flat and relieved by sitting forward. The main diagnostic challenge is distinguishing it from STEMI.
Pathophysiology: Inflammation of the pericardium (which has no myocardial cells) causes a generalized current of injury near the epicardial surface of the ventricles and atria, producing diffuse ST changes and PR depression (atrial injury).
ECG Changes (Fuster & Hurst's The Heart, 15th Ed.):
- Diffuse, concave ("saddle-shaped") ST elevation in most leads (I, II, III, aVF, V2-V6) - not regional
- PR segment depression in the same leads - atrial injury; this is the most specific finding
- No reciprocal ST depression (unlike STEMI)
- No Q waves, no concurrent T-wave inversion during the ST-elevation phase
- aVR is the mirror image: ST depression + PR elevation in aVR
4 ECG Stages of Pericarditis:
| Stage | Timing | ECG |
|---|---|---|
| Stage 1 | Day 1-2 | Diffuse ST elevation + PR depression |
| Stage 2 | Days 3-7 | ST resolves, T waves flatten |
| Stage 3 | Week 2 | Diffuse T-wave inversions |
| Stage 4 | Weeks-months | ECG normalizes |
Note: 90% of pericarditis patients have some ECG abnormality, but less than 60% progress through all 4 stages (Fuster & Hurst's).
ECG - Acute Pericarditis Stage 1 (Fuster & Hurst's The Heart - diffuse ST elevation with PR depression in non-territory-specific distribution; aVR shows the mirror pattern):
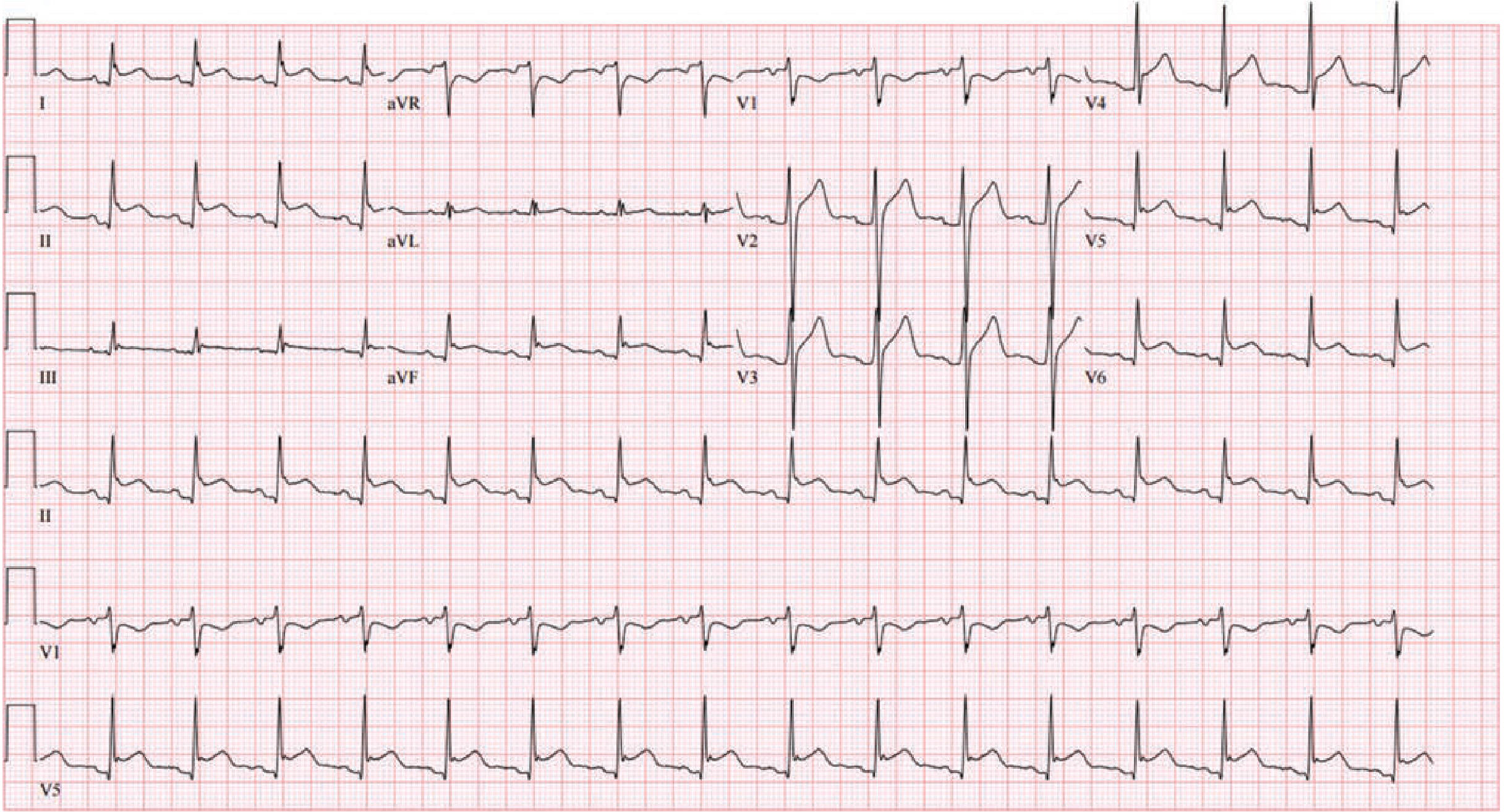
Fuster and Hurst's The Heart, 15th Edition - Fig. 53-3
8. Ventricular Fibrillation (VF)
What it is: Completely disorganized, chaotic electrical activity throughout the ventricles with no effective contraction - causes immediate cardiac arrest. The most common initial rhythm in sudden cardiac death. Without immediate defibrillation, death occurs within minutes.
Pathophysiology: Multiple simultaneous reentry circuits fire chaotically throughout the ventricular myocardium, producing no coordinated contraction. Cardiac output drops to zero.
ECG Changes:
- Completely chaotic, irregular waveforms with no discernible P waves, QRS complexes, or T waves
- Baseline undulates wildly at a variable frequency
- Coarse VF: larger amplitude waves (more recent onset, more likely to respond to defibrillation)
- Fine VF: very low amplitude waves (prolonged arrest, poorer prognosis)
- No organized cardiac electrical activity whatsoever
Immediate management: Unsynchronized defibrillation + CPR + epinephrine (ACLS protocol).
9. Left Ventricular Hypertrophy (LVH)
What it is: Pathological thickening of the left ventricular myocardium, most commonly from chronic pressure overload (hypertension, aortic stenosis). Increases the risk of arrhythmia, heart failure, and sudden death.
ECG Changes:
- High QRS voltage - the most sensitive finding:
- Sokolow-Lyon criterion: S in V1 + R in V5 or V6 ≥35 mm
- Cornell criterion: R in aVL + S in V3 ≥28 mm (men) / ≥20 mm (women)
- Tall R waves in left precordial (V5-V6) and lateral limb leads (I, aVL)
- Deep S waves in right precordial leads (V1-V2)
- Left axis deviation (QRS axis < -30°)
- LV strain pattern: asymmetric ST depression and T-wave inversion in V5-V6, I, aVL (indicating subendocardial ischemia from the hypertrophied muscle outstripping its blood supply)
- Left atrial enlargement: broad, notched "P mitrale" in II; biphasic P wave in V1
10. Pulmonary Embolism (PE) - Right Heart Strain
What it is: Obstruction of the pulmonary arterial tree by thrombus, causing acute right ventricular pressure overload and strain. Massive PE causes acute cor pulmonale and can lead to right heart failure and hemodynamic collapse.
Pathophysiology: Sudden increase in pulmonary vascular resistance dilates the right ventricle, shifts the interventricular septum leftward, and compresses the left ventricle - reducing cardiac output. Right heart strain is reflected in the ECG.
ECG Changes (Harrison's 22E, Tintinalli's):
- Sinus tachycardia - the most common ECG finding in PE (~50% of cases)
- S1Q3T3 pattern - S wave in lead I, Q wave + T-wave inversion in lead III (~20% of cases, but specific)
- New RBBB or incomplete RBBB - from right ventricular strain causing delayed RV conduction
- T-wave inversions in V1-V4 (right precordial leads) - RV ischemia/strain
- Right axis deviation
- Sinus tachycardia with or without atrial fibrillation
- P pulmonale (tall peaked P waves >2.5 mm in II, III, aVF) in chronic cor pulmonale
Note: The ECG in PE is often non-specific or normal. A normal ECG does not exclude PE - CT pulmonary angiography remains the gold standard.
Quick Reference Summary
| # | Disease | Rhythm | Key ECG Feature | Rate |
|---|---|---|---|---|
| 1 | STEMI | Regular | Regional ST elevation + Q waves | Variable |
| 2 | Atrial Fibrillation | Irregularly irregular | Absent P waves, chaotic baseline | 100-160 uncontrolled |
| 3 | Atrial Flutter | Regular (usually) | Sawtooth F waves ~300/min | ~150 at 2:1 |
| 4 | AV Block | Regular/irregular | PR prolongation / dropped beats / AV dissociation | Slow |
| 5 | Ventricular Tachycardia | Regular | Wide QRS ≥120 ms, AV dissociation | 100-250 |
| 6 | WPW Syndrome | Variable | Short PR + delta wave + wide QRS | Variable |
| 7 | Acute Pericarditis | Regular | Diffuse ST elevation + PR depression (no reciprocal changes) | Normal/fast |
| 8 | Ventricular Fibrillation | None | Completely chaotic - no QRS | None |
| 9 | LVH | Regular | High voltage (SV1+RV5 ≥35mm) + strain pattern | Normal |
| 10 | Pulmonary Embolism | Regular/fast | S1Q3T3, RBBB, sinus tachycardia, T inversions V1-V4 | Fast |
Sources:
- Rosen's Emergency Medicine, 10e - STEMI ECG images and localization table
- Guyton and Hall Textbook of Medical Physiology - AF and atrial flutter ECG images
- Harrison's Principles of Internal Medicine, 22E (2025) - AV block classification
- Washington Manual of Medical Therapeutics - AV block ECG image (all 5 types)
- Symptom to Diagnosis, 4th Edition - VT criteria, VT ECG images, WPW ECG image
- Fuster and Hurst's The Heart, 15th Edition - Pericarditis ECG stages and image
- Goldman-Cecil Medicine - WPW, VT, arrhythmia evaluation
This is a shared conversation. Sign in to Orris to start your own chat.