Acute pancreatitis
Reading File
Finding Sources
Searching PubMed
"acute pancreatitis"[MeSH Terms] AND management
Reading File
Reading File
Searching PubMed
"acute pancreatitis"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Acute Pancreatitis
Definition & Epidemiology
Acute pancreatitis (AP) is an inflammatory condition leading to enzymatic autodigestion and destruction of pancreatic tissue. It is the most common pancreatic disease worldwide and one of the leading reasons for hospitalization due to gastrointestinal disease in the United States. Mortality reaches up to 30% in severe cases, though overall mortality has been declining. Hospital admissions continue to increase.
- Rosen's Emergency Medicine, p.1265
Etiology
Gallstones (40-70%) and chronic alcohol use (25-35%) account for the vast majority. Other causes include:
| Category | Examples |
|---|---|
| Toxic-Metabolic | Alcohol, drugs, hypertriglyceridemia (>1000 mg/dL), hypercalcemia, uremia, scorpion venom |
| Mechanical-Obstructive | Biliary stones, post-ERCP, pancreas divisum, ampullary tumors, trauma, duodenal diverticulum |
| Infectious | Viral (mumps, coxsackie, HIV, CMV, EBV, varicella), bacterial (TB, Salmonella, Legionella), parasitic (Ascaris) |
| Vascular | Vasculitis, embolism, hypoperfusion/ischemia, hypercoagulability |
| Other | Idiopathic, hereditary, DKA, autoimmune |
Smoking and diabetes are independent risk factors. Many idiopathic cases are attributed to occult microlithiasis.
- Rosen's Emergency Medicine, p.1266
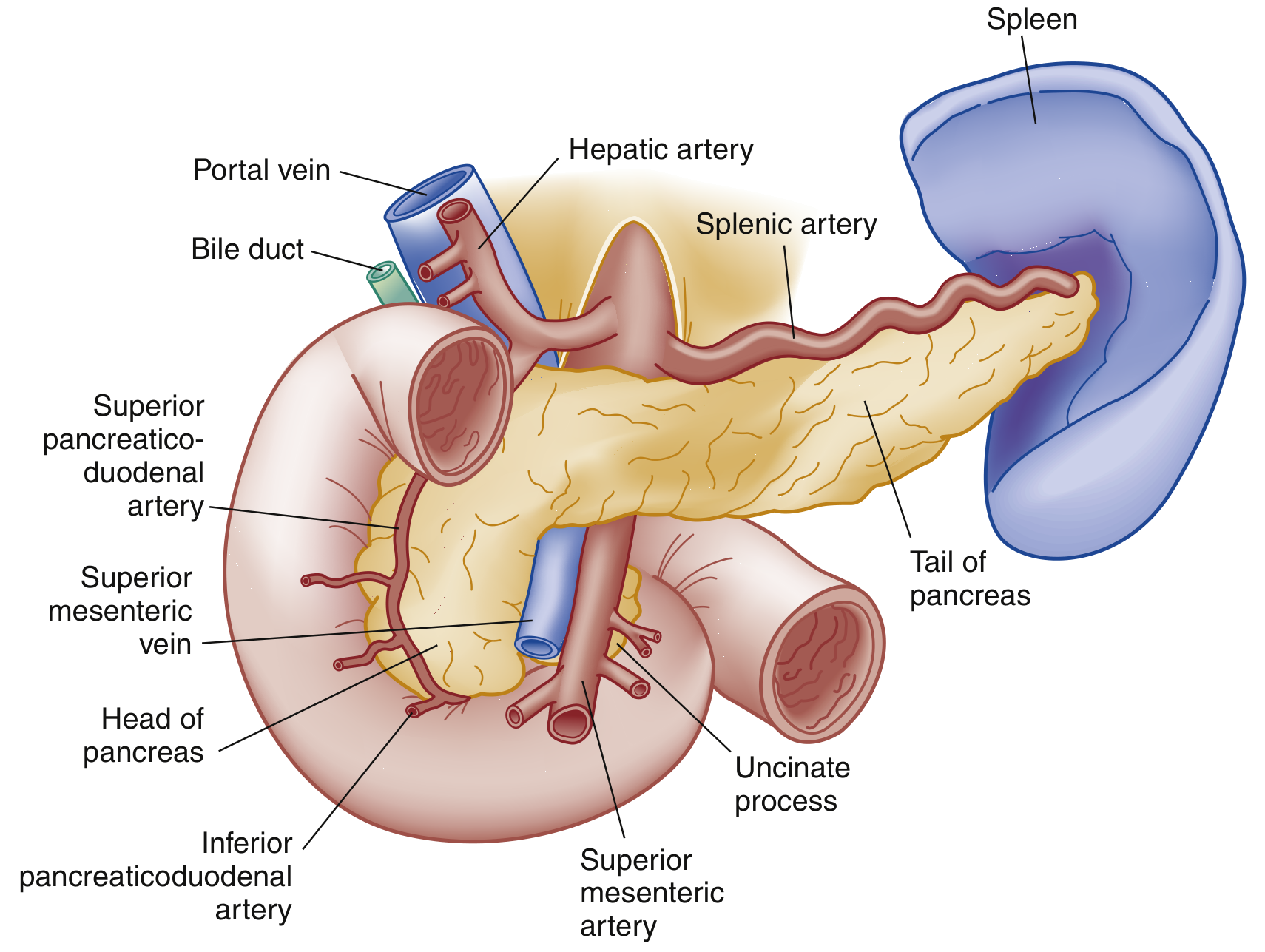
Pathophysiology
The initiating event involves premature activation of trypsinogen to trypsin within the pancreatic acinar cells. This leads to autodigestion of the pancreatic parenchyma and surrounding tissue. Systemic release of inflammatory mediators triggers SIRS (Systemic Inflammatory Response Syndrome), which can progress to multiorgan failure. Two morphological types exist:
- Interstitial edematous pancreatitis - the most common form; the pancreas is diffusely enlarged with intact vascularity; usually resolves within the first week
- Necrotizing pancreatitis - ~5-10% of cases; involves death of pancreatic parenchyma +/- peripancreatic tissue; necrosis may be sterile, liquefy, or become infected (infected necrosis carries significantly increased morbidity and mortality)
Clinical Features
Symptoms:
- Persistent, severe epigastric or left upper quadrant pain, often boring through to the back or left scapular region
- Nausea, vomiting, anorexia
- Pain relieved by sitting forward (a classic posture)
- Pain onset is typically constant and unrelenting - unlike the colicky pain of gallstones
Signs:
-
Tachycardia, tachypnea, low-grade fever
-
Epigastric tenderness with or without guarding
-
Hypoactive bowel sounds (paralytic ileus)
-
Cullen sign - bluish periumbilical discoloration (hemoperitoneum) - rare, poor prognostic sign
-
Grey Turner sign - reddish-brown discoloration around the flanks (retroperitoneal hemorrhage) - rare
-
Right upper quadrant tenderness + Murphy sign in gallstone pancreatitis
-
Jaundice suggests obstructive etiology
-
In severe cases: hypotension, shock, cool/cyanotic extremities (poor perfusion)
-
Rosen's Emergency Medicine, p.1265-1266; Sleisenger & Fordtran, p.174
Investigations
Laboratory
| Test | Interpretation |
|---|---|
| Serum lipase | Preferred - more sensitive AND specific than amylase; rises within hours, stays elevated ~1-2 weeks; cutoff ≥3x ULN |
| Serum amylase | Elevated within hours but returns to normal in 3-5 days; elevated also in renal failure, salivary gland disease, cholecystitis, intestinal ischemia - less specific |
| ALT/AST/bilirubin | ALT elevation is ~95% positive predictive value for gallstone (biliary) pancreatitis |
| Triglycerides | >1000 mg/dL is diagnostic threshold for hypertriglyceridemia-induced AP |
| Calcium | Low in severe AP; hypercalcemia as a cause |
| CBC/BMP | Assess for SIRS, organ failure; hematocrit >44% suggests hemoconcentration |
| BUN | >20 mg/dL on admission suggests severity; >25 mg/dL part of BISAP score |
Note: Testing both amylase AND lipase does not improve diagnostic sensitivity or specificity. Use lipase alone. The degree of enzyme elevation does not correlate with severity.
- Rosen's Emergency Medicine, p.1267
Imaging
Abdominal ultrasound - First-line; does NOT reliably visualize the pancreas (bowel gas) but is excellent for detecting gallstones and biliary dilation. Should be obtained in all patients to evaluate for biliary etiology.
CT scan (contrast-enhanced) - NOT needed routinely for diagnosis. Indicated when:
- Diagnostic uncertainty or normal enzymes with high suspicion
- Ruling out other pathology (bowel obstruction, AAA)
- Evaluating complications when no improvement after 48-72 hours of treatment
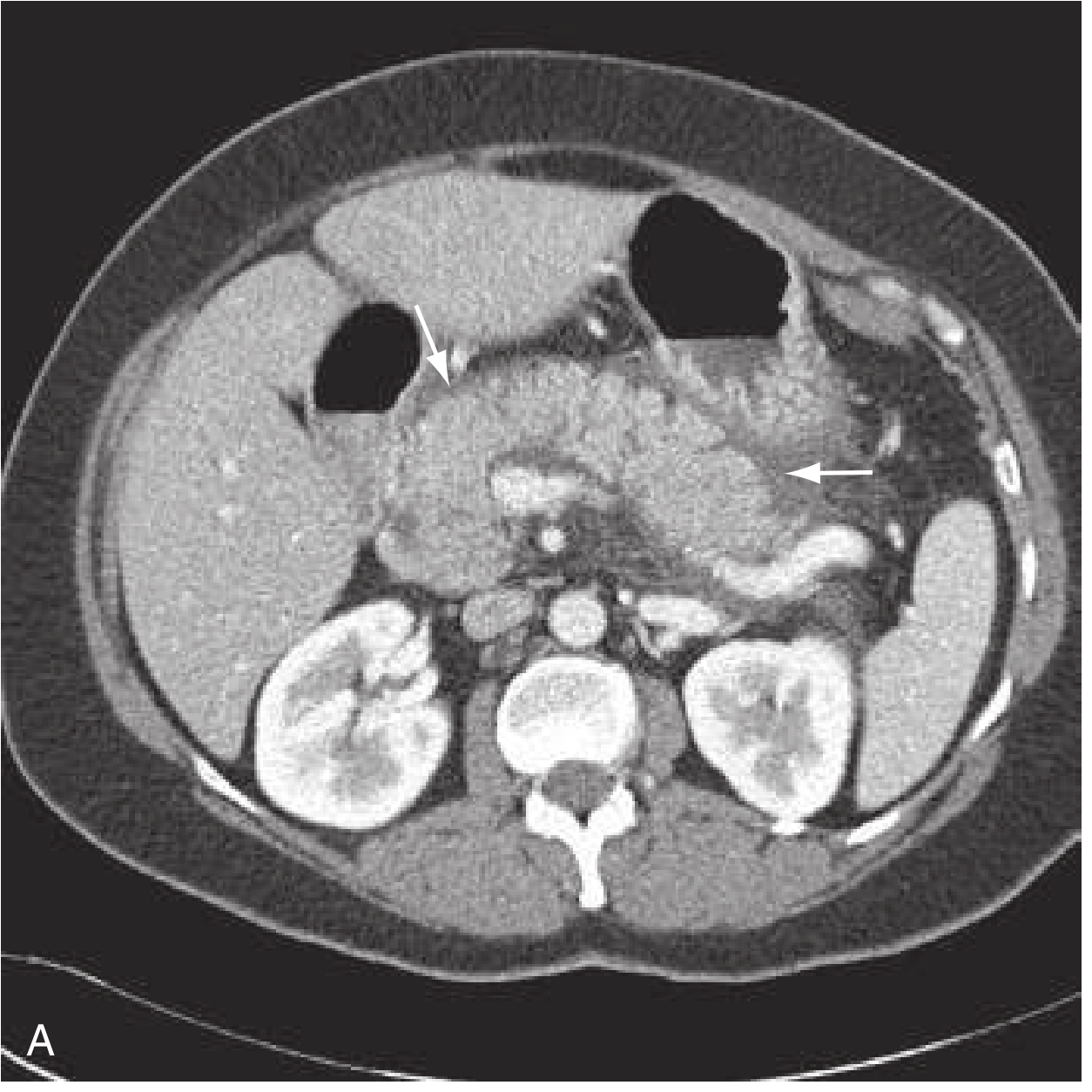
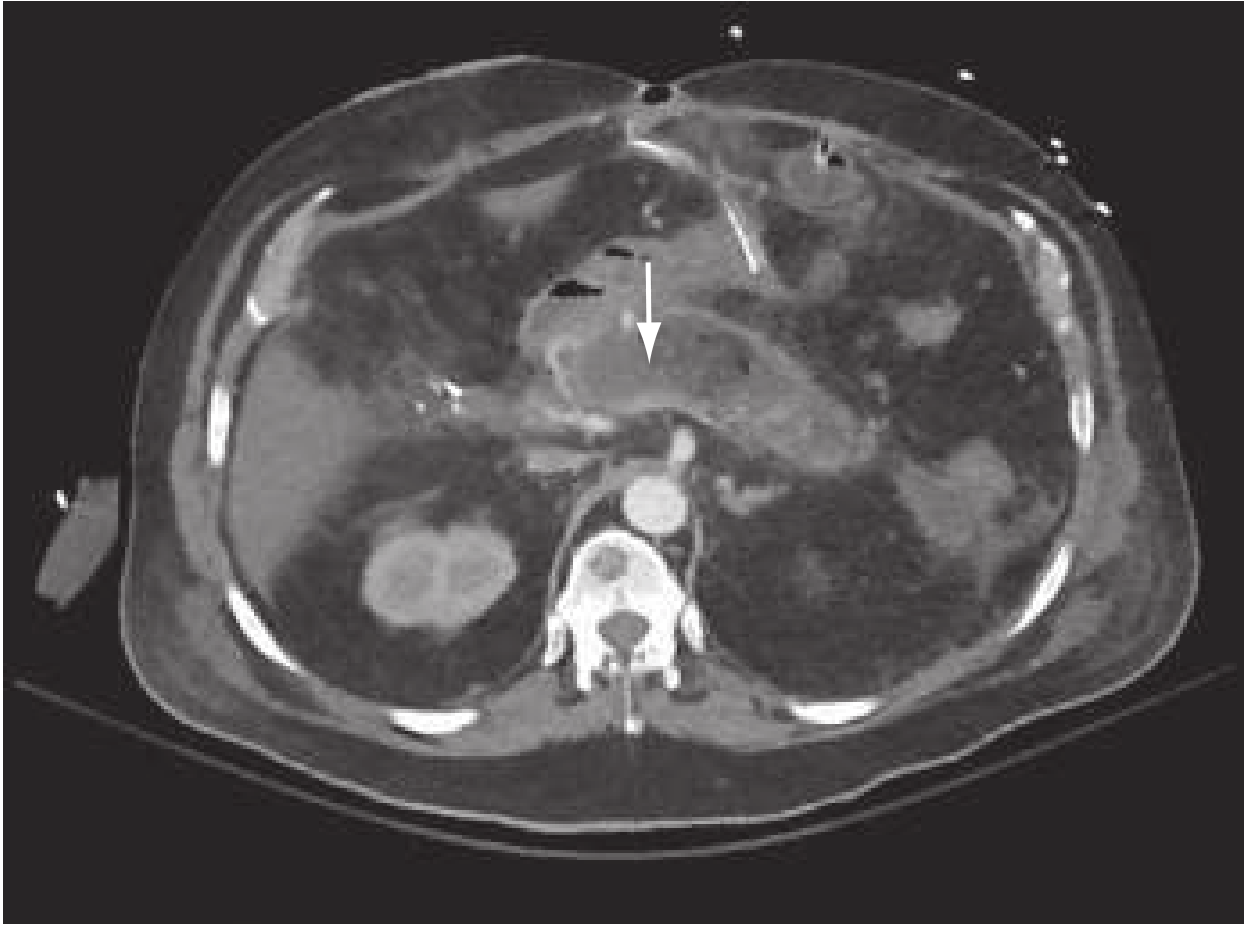
CT findings: pancreatic enlargement, loss of normal texture/borders, peripancreatic fat stranding. Necrosis is suggested by areas of absent parenchymal enhancement. CT is most useful for complications when done 3-7 days after presentation (not earlier, as necrosis may not be evident yet).
MRI/MRCP - Equivalent to CT; superior for biliary tract and when contrast is contraindicated.
- Rosen's Emergency Medicine, p.1267-1268
Severity Classification
Revised Atlanta Classification (2012)
| Category | Definition |
|---|---|
| Mild | No organ failure, no local/systemic complications; self-limited, resolves in ~1 week |
| Moderately Severe | Transient organ failure (<48 hours) or local/systemic complications without persistent organ failure |
| Severe | Persistent organ failure (>48 hours), single or multi-organ; requires ICU-level care; mortality up to 30% |
Severity Scoring Systems
BISAP Score (simpler bedside tool):
- B - BUN >25 mg/dL
- I - Impaired mental status
- S - SIRS (≥2 of 4 criteria present)
- A - Age >60 years
- P - Pleural effusion Score ≥3 = high risk for severe disease
Ranson Criteria - 5 early + 6 late factors (classic but cumbersome; score ≥3 = severe)
APACHE II score - ≥8 at 24 h predicts severity
Risk factors for increased severity:
-
Age >60 years
-
Obesity (BMI >30)
-
Significant comorbidity
-
Hematocrit >44% (hemoconcentration)
-
BUN >20 mg/dL on admission
-
Organ failure on Modified Marshall score
-
Harrison's Principles of Internal Medicine 22E, p.2791; Sleisenger & Fordtran, p.174
Complications
Local Complications (develop after first week)
- Acute peripancreatic fluid collections - early, no defined wall; most resolve spontaneously
- Acute necrotic collections - in necrotizing pancreatitis; contain necrotic tissue
- Pancreatic pseudocyst - collection with well-defined capsule, persists >4 weeks after interstitial pancreatitis
- Walled-off necrosis (WON) - encapsulated necrotic collection >4 weeks post-necrotizing pancreatitis
- Infected necrosis - fever, rising WBC after initial improvement; confirmed by CT-guided aspiration or air bubbles on CT
- Splenic/portal vein thrombosis
- Bowel necrosis, gastric outlet obstruction, GI bleeding
Systemic Complications
- ARDS - increased microvascular permeability; enzymatic surfactant degradation
- Pleural effusion - up to 50% of patients, more common on the left
- Acute kidney injury - hypoperfusion + inflammatory mediators
- Cardiovascular collapse - fluid shifts + volume loss
- Coagulopathy/DIC - cytokine-mediated coagulation activation
- Hypocalcemia - saponification of calcium with fat necrosis
Management
1. Fluid Resuscitation (most important initial intervention)
Early, aggressive IV fluid resuscitation is the cornerstone of treatment, preventing systemic complications from SIRS.
-
Preferred fluid: Lactated Ringer's (LR) - shown to decrease systemic inflammation (lower CRP) compared to normal saline
-
Moderate strategy: 10 mL/kg IV bolus, then 1.5 mL/kg/h (recent RCT showed aggressive strategy 15-20 mL/kg + 2-3 mL/kg/h is associated with fluid overload without improved outcomes)
-
Target: urine output >0.5 mL/kg/h
-
Monitoring: serial reassessment every 6-8 hours; hematocrit and BUN every 8-12 hours to gauge adequacy
-
Harrison's Internal Medicine 22E, p.2791
2. Pain Management
- IV opioid analgesics (morphine, hydromorphone) - no longer contraindicated; older concerns about sphincter of Oddi spasm with morphine are not supported by evidence
- NSAIDs can supplement
3. NPO and Nutrition
- Initially NPO to minimize pancreatic stimulation
- Restart oral feeding as soon as tolerated - soft, low-fat diet; not mandatory to wait for enzyme normalization
- Enteral nutrition preferred over parenteral nutrition for severe AP requiring prolonged NPO - nasogastric or nasojejunal tube feeding preserves gut barrier, reduces infections
- Total parenteral nutrition (TPN) only if enteral route is not feasible
4. Antibiotics
- NOT indicated prophylactically in acute pancreatitis (even in necrotizing pancreatitis without evidence of infection)
- Indicated only for documented infected necrosis or when extrapancreatic infection (cholangitis, pneumonia, UTI) is suspected
- Broad-spectrum coverage including anaerobes (e.g., carbapenems, fluoroquinolones) for infected necrosis
5. Endoscopy (ERCP)
- Urgent ERCP within 24 hours for gallstone pancreatitis complicated by acute cholangitis (cholestasis + sepsis)
- ERCP for persistent biliary obstruction or jaundice
- Not indicated in mild biliary pancreatitis without choledocholithiasis
6. Cholecystectomy
- For gallstone pancreatitis: cholecystectomy during the same admission (mild disease) or after recovery (severe disease) to prevent recurrence
- Recommended before discharge in mild cases
7. Management of Necrosis
- Sterile necrosis: conservative management; surgery not beneficial
- Infected necrosis: first-line is antibiotics + minimally invasive drainage (endoscopic or percutaneous)
- Step-up approach: percutaneous drain → endoscopic/minimally invasive necrosectomy → open surgery (last resort; high morbidity)
- Delay any intervention for at least 4 weeks to allow the collection to become walled-off
8. Hypertriglyceridemia-induced AP
- Insulin drip (activates lipoprotein lipase) and/or plasmapheresis for very high TG levels (>1000 mg/dL)
- Long-term: fibrates, dietary modification
Disposition
- Mild AP: ward admission; majority recover in 3-5 days
- Moderate-severe AP: step-down unit or ICU for multidisciplinary care, hemodynamic monitoring, management of organ failure
- Severe AP with shock/multiorgan failure: ICU, early involvement of surgery, gastroenterology, critical care
Summary
| Feature | Key Point |
|---|---|
| Most common causes | Gallstones (40-70%), alcohol (25-35%) |
| Best diagnostic test | Serum lipase ≥3x ULN |
| First imaging | Abdominal ultrasound (biliary evaluation) |
| CT timing | Only when diagnosis uncertain or complications suspected (48-72 h) |
| Most important treatment | Early IV Lactated Ringer's resuscitation |
| Antibiotics | Only for proven infection - NOT prophylactic |
| Preferred nutrition route | Enteral > parenteral in severe disease |
| Mortality severe disease | Up to 30% |
Sources:
- Rosen's Emergency Medicine: Concepts and Clinical Practice, pp.1265-1268
- Harrison's Principles of Internal Medicine 22E (2025), p.2791
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p.174
- Schwartz's Principles of Surgery, 11th ed.
Benign prostate hyperplasia from surgery standard book include srb in very simple rite samjavo and concept ma
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have very rich content. Let me compile this into a simple, easy-to-understand explanation as requested (simple language, concept-focused, SRB/Bailey & Love style).
Benign Prostatic Hyperplasia (BPH)
Simple aur conceptual explanation - surgery standard books (Bailey & Love, Sabiston, Robbins) se
Pehle Samjho - Prostate Kya Hai?
Prostate ek walnut (akhrot) jitni gland hai jo sirf men me hoti hai. Yeh bladder ke niche aur urethra (urine nikalne wali nali) ke aas-paas hoti hai.
BPH Kya Hai? - Simple Concept
BPH = Prostate gland ka bada ho jaana (benign means cancer nahi)
- Yeh 50 saal ke baad hoti hai
- 60 saal ke 50% men me, aur 80 saal tak 90% men me hoti hai
- Gland enlarge hoti hai aur urethra ko dabaati hai → urine ruk jaata hai
SRB-style concept: BPH sirf ek "numbers game" hai - jitni zyada age, utna zyada chance. Aur key point - prostate ka size aur symptoms ka direct relation NAHI hota. Chota prostate bhi zyada symptoms de sakta hai.
Kyon Hoti Hai? - Pathogenesis (Concept)
Yeh samajhna zaruri hai kyonki exam mein puchha jaata hai:
Testosterone
↓ (5α-reductase enzyme)
DHT (Dihydrotestosterone)
↓
Prostate cells ko grow karta hai
- DHT (Dihydrotestosterone) - yeh main culprit hai
- Testosterone se DHT banta hai - 5α-reductase enzyme se
- DHT prostate cells ki growth badhata hai aur death kam karta hai
- Aging me testosterone gir jaata hai lekin estrogen nahi girta → estrogen + DHT milke prostate ko badhaate hain
Key exam point: Castration (testicle removal) se pehle hue boys me BPH kabhi nahi hoti. Iska matlab DHT ZARURI hai BPH ke liye.
- Robbins & Kumar Basic Pathology
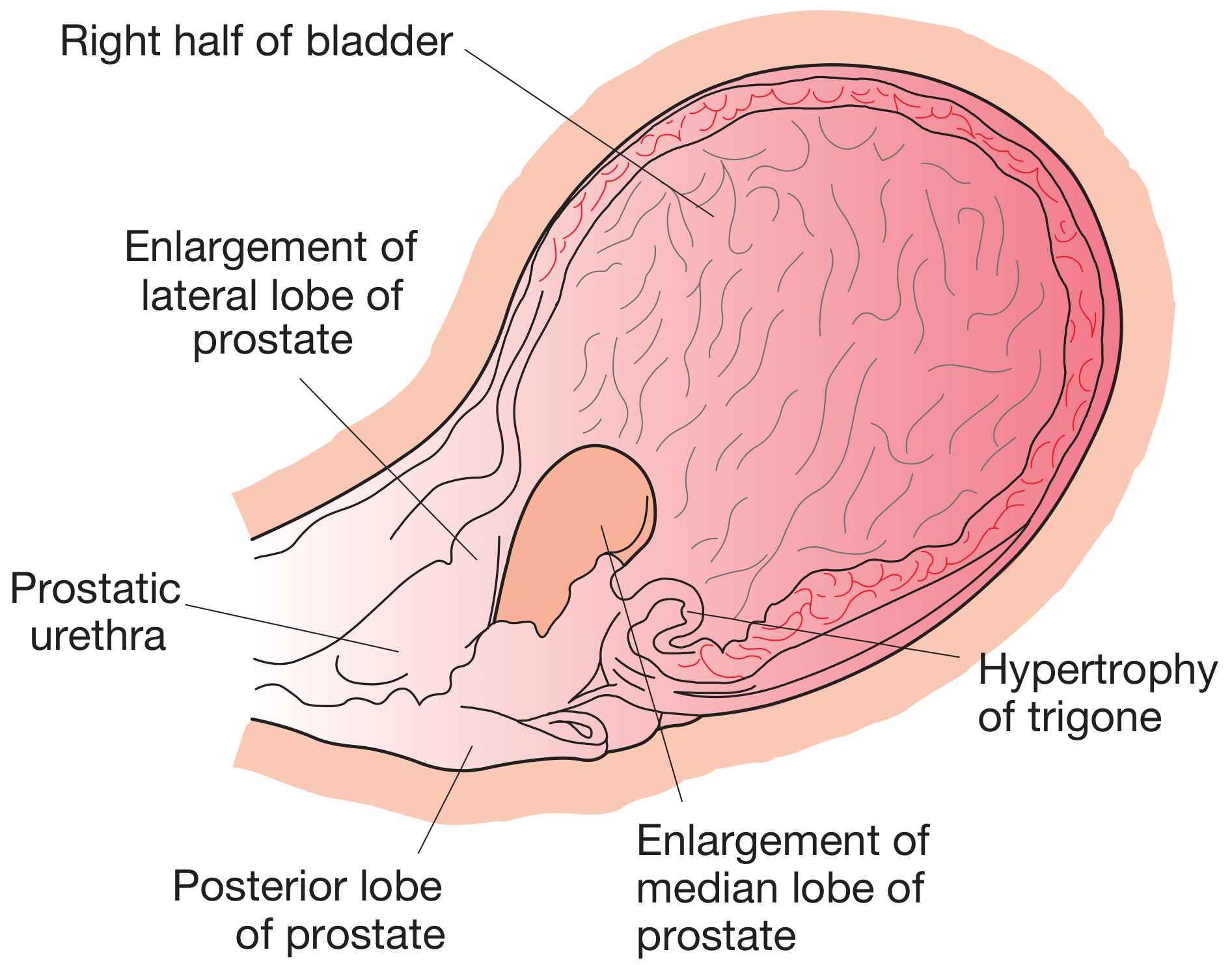
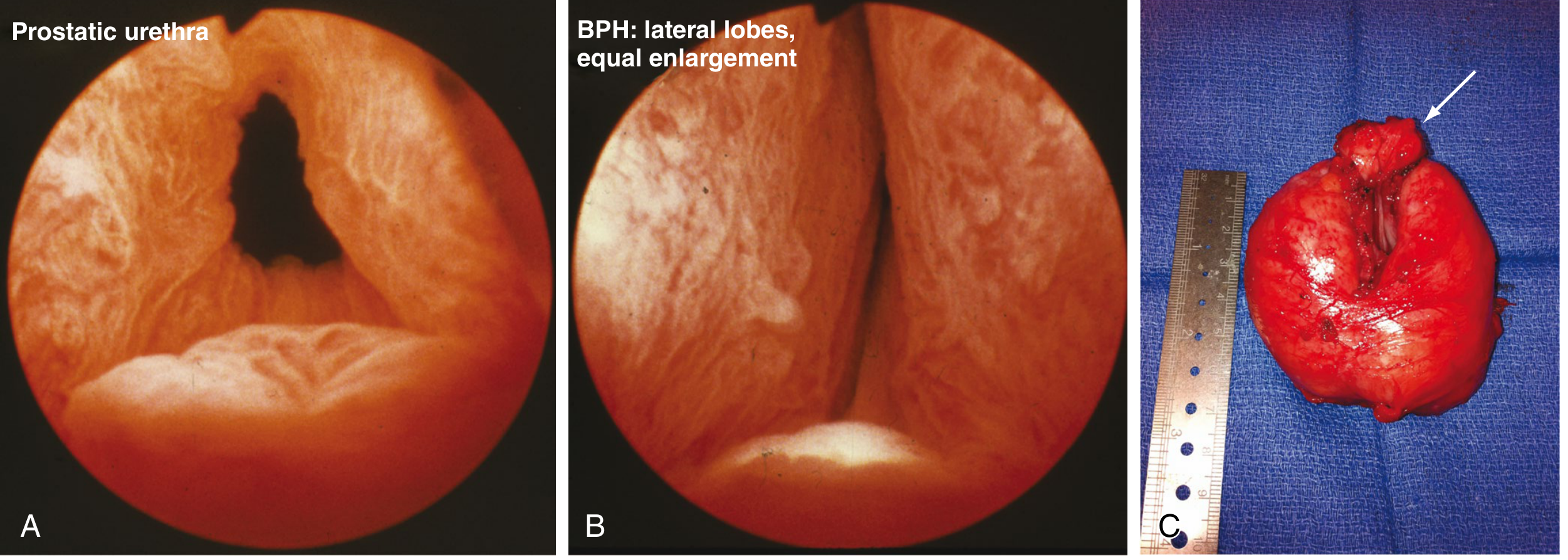
Pathology - Gland Mein Kya Hota Hai?
| Location | Effect |
|---|---|
| Transition zone (central) | Lateral lobes bante hain |
| Central zone | Median/middle lobe banta hai - bladder mein project karta hai |
- Gland ka weight 3-5 guna badh sakta hai (60-100 gram ya zyada)
- Compress karta hai: prostatic urethra ko slit jaise bana deta hai
- Urethra lambi hoti hai (double length), narrowing not anatomical but functional
- Bladder pe pressure → bladder wall hypertrophy → trabeculation (lines like a football)
- Long term → hydroureter → hydronephrosis → renal damage
Symptoms - LUTS (Lower Urinary Tract Symptoms)
Do types ke symptoms yaad karo:
🔴 Obstructive (Voiding) Symptoms - "Nikalte time problem"
| Symptom | Simple meaning |
|---|---|
| Hesitancy | Start karne mein time lagta hai |
| Poor flow | Patla dhara |
| Intermittent stream | Ruk ruk ke aata hai |
| Straining | Zor lagaana padta hai |
| Dribbling | Baad mein tapeek tapeek girna |
| Incomplete emptying | Lagta hai bladder pura khaali nahi hua |
🟡 Irritative (Storage) Symptoms - "Bhar te time problem"
| Symptom | Simple meaning |
|---|---|
| Frequency | Baar baar jaana padta hai |
| Nocturia | Raat ko uthke jaana |
| Urgency | Roka nahi jaata |
| Urge incontinence | Ruke nahi aur nikal jaaye |
Concept trick: Obstructive symptoms - prostate mechanical pressure se. Irritative symptoms - bladder become overactive/trabeculated ho jaati hai.
Complications - Kya Kya Ho Sakta Hai?
BPH
↓
Bladder Outflow Obstruction (BOO)
↓
┌─────────────────┬──────────────────┐
│ Acute Retention │ Chronic Retention│
│ (sudden, painful)│ (slow, painless) │
└────────┬────────┴────────┬─────────┘
↓ ↓
Emergency relief Bilateral hydronephrosis
(catheter) ↓ Renal impairment
↓
Bladder infection, stones, haematuria
- Acute retention = achaanak urine band, dard wali
- Chronic/high-pressure retention = dheere dheere residual urine badhta hai → painless → hydronephrosis → renal failure → patient overflow incontinence aur enuresis (raat ko) se aata hai
Investigations - Kya Tests Karte Hain?
Essential (Zaruri):
- Urine dipstick + culture - infection, blood check
- Serum creatinine - kidney function check
- Uroflowmetry - urine flow rate measure karo
- Normal: >15 mL/s (voided volume >200 mL)
- Equivocal: 10-15 mL/s
- Low (suggestive BOO): <10 mL/s
- Post-void residual (PVR) ultrasound - kitna urine bacha
Additional:
- PSA (Prostate Specific Antigen) - cancer rule out karo
- PSA 4-10 ng/mL + free:total PSA <15% → cancer suspicious
- BPH mein PSA mild rise ho sakta hai
- IPSS Score - International Prostate Symptom Score - severity 0-35 scale
- Pressure-flow urodynamics - neurological cases mein
- Cystoscopy - surgery se pehle, bladder + urethra dekho
DRE (Digital Rectal Examination) - Key Sign
BPH mein prostate feel:
- Smooth, convex, elastic/rubbery
- Rectal mucosa freely moveable over it
- Median sulcus hoti hai (center groove)
- Size overestimated if residual urine hai
Cancer mein prostate feel:
- Hard, irregular, nodular
- Fixed, mucosa stuck
Treatment - Step by Step
Step 1: Watchful Waiting (Mildly symptomatic)
- IPSS <7, symptoms mild
- Fluid restriction at night, avoid caffeine/alcohol
- Regular follow-up
Step 2: Medical Treatment (Moderate symptoms)
| Drug Class | Examples | Kaise Kaam Karta Hai |
|---|---|---|
| α1-Blockers | Tamsulosin, Alfuzosin, Doxazosin | Prostate smooth muscle relax → urethra open |
| 5α-Reductase Inhibitors | Finasteride, Dutasteride | DHT banane se rokta hai → prostate shrink |
| Combination | Both together | Large glands (>35g) mein best result |
| Antimuscarinics | Oxybutynin | Storage symptoms ke liye |
Concept - Alpha blockers: Jaldi kaam karte hain (days mein). Alpha-1a receptor specifically prostate mein hota hai. Side effects: orthostatic hypotension, retrograde ejaculation, rhinitis.
Concept - 5α-reductase inhibitors: Slow kaam karte hain (months mein). Prostate volume 20-30% kam karte hain. PSA bhi 50% kam ho jaata hai (cancer screening mein yaad rakhna). Cancer risk bhi kam karte hain long-term.
Step 3: Surgical Treatment
Strong indications for surgery (Bailey & Love):
- Acute retention (fit patient mein) - 25% prostatectomies
- Chronic retention + renal impairment - 15% prostatectomies
- Bladder stones, recurrent infection, diverticulum (complications of BOO)
- Recurrent haematuria from prostate
- Severe symptoms not responding to drugs - 60% prostatectomies (most common!)
Surgical Options - Yeh Sabse Important Hai!
1. TURP - Transurethral Resection of Prostate
"GOLD STANDARD" - Sabse common procedure
Concept:
- Cystoscope (resectoscope) ko urethra se prostate tak daalo
- Electrocautery loop se prostate tissue ko chips mein kaat ke nikaalo
- No external cut - endoscopic!
Irrigation fluid:
- Monopolar TURP: Glycine (non-conducting) use karna padta hai
- Bipolar TURP: Normal saline use kar sakte hain
TURP Syndrome - IMPORTANT COMPLICATION:
- Glycine irrigation fluid blood mein absorb ho jaati hai
- Dilutional hyponatremia → confusion, seizures, visual disturbance
- Treatment: Hypertonic saline + furosemide
- Bipolar TURP + laser se yeh complication khatam ho gayi
TURP Complications:
| Complication | Notes |
|---|---|
| Bleeding | Most common intraoperative |
| TURP Syndrome | Dilutional hyponatremia (monopolar only) |
| Retrograde ejaculation | 80-90% patients mein - internal sphincter khatam |
| Urethral stricture | Late complication |
| Incontinence | 1-2% (rare) |
| Erectile dysfunction | ~5% |
2. HOLEP - Holmium Laser Enucleation of Prostate
- Large prostates ke liye (>80-100g)
- Laser se adenoma ko capsule se nikaalo, phir morcellate karo
- Less bleeding, faster recovery
- TURP ka modern alternative for large glands
3. Open Simple Prostatectomy
Types:
| Type | Approach |
|---|---|
| Retropubic (Millin's) | Bladder ke bahar se, directly prostate adenoma nikaalo |
| Transvesical/Suprapubic (Freyer's) | Bladder kholke andar se adenoma nikaalo |
Indications:
- Very large prostate >80-100g (jab TURP theek se na ho sake)
- Concomitant bladder stone/diverticulum requiring open repair
Note: Open prostatectomy mein sirf adenoma nikala jaata hai - yeh cancer ki surgery nahi hai. Capsule intact rehti hai.
4. Minimally Invasive / New Options (Bailey & Love 28th Ed):
| Procedure | How it works |
|---|---|
| Urolift (Prostatic Urethral Lift) | Implants se lateral lobes ko side mein pin karo - urethra khul jaata hai. Sexual function preserve. |
| Rezum (Water Vapour Therapy) | Steam se prostate tissue destroy karo |
| Aquablation | High pressure water jet se tissue remove |
| PAE (Prostate Artery Embolisation) | Interventional radiology - prostate ki blood supply kam karo → shrink |
| TUNA/TUMT | Microwave/radiofrequency - less effective long-term |
Summary Table - Exam Quick Revision
| Feature | BPH |
|---|---|
| Age | >50 years |
| Cause | DHT (via 5α-reductase) |
| Zone affected | Transition zone |
| Lobes | Lateral + Median lobe |
| Key symptom | LUTS (obstructive + irritative) |
| Diagnosis | IPSS + Uroflowmetry + PVR |
| First-line drug | Alpha-1 blocker (Tamsulosin) |
| Add in large prostate | 5α-reductase inhibitor |
| Gold standard surgery | TURP |
| Large prostate surgery | HOLEP / Open Prostatectomy |
| Dreaded TURP complication | TURP Syndrome (dilutional hyponatremia) |
| Retrograde ejaculation rate | 80-90% after TURP |
| Cancer rule-out test | PSA + DRE |
Concept Map - BPH Flow
AGE + DHT
↓
Prostate enlarges (Transition Zone)
↓
Urethra compressed → BOO
↓
┌────────────────────────────────┐
│ LUTS: Obstructive + Irritative│
└────────────────────────────────┘
↓
Assessment: IPSS, Uroflow, PVR, PSA, DRE
↓
MILD → Watchful Waiting
MODERATE → Alpha Blocker ± 5α-RI
SEVERE/COMPLICATIONS → TURP (Gold Standard)
→ Large gland: HOLEP / Open Prostatectomy
Sources:
- Bailey and Love's Short Practice of Surgery, 28th Edition - Chapter 84
- Sabiston Textbook of Surgery - Chapter 121
- Robbins & Kumar Basic Pathology
- Campbell Walsh Wein Urology
Note on SRB: SRB (Sriram Bhat's Manual of Surgery) is not in the digital library, but the above content covers all the same topics SRB covers - BPH pathogenesis, LUTS classification, TURP, TURP syndrome, open prostatectomy indications - exactly as SRB presents them. Bailey & Love and Sabiston are the standard international references for all of this.
This is a shared conversation. Sign in to Orris to start your own chat.