Peritonitis
Reading File
Finding Sources
Searching PubMed
peritonitis management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have extensive, comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Peritonitis
Peritonitis is inflammation of the peritoneum - the serous membrane lining the abdominal cavity and viscera. It is a potentially life-threatening condition that may be localised or diffuse, acute or chronic, bacterial or chemical.
Classification
By Source
| Type | Definition | Key Features |
|---|---|---|
| Primary (Spontaneous) | No apparent source of GI contamination | Usually monomicrobial; gram-negatives dominant |
| Secondary | Arises from an identifiable intraabdominal source | Polymicrobial; gram-negatives + anaerobes |
| Tertiary | Persistent/recurrent peritonitis after treatment | Often drug-resistant organisms, fungi |
By Extent
- Localised - involves a focal area; parietal peritoneal involvement causes somatic pain with guarding and rebound
- Diffuse (generalised) - involves large regions of the parietes; signifies life-threatening pathology
Causes / Aetiology
Bacterial (most common):
- Perforation of abdominal viscus (peptic ulcer, appendix, diverticulum, colon in obstruction)
- Transmural bacterial translocation without frank perforation (pancreatitis, ischaemic bowel, primary bacterial peritonitis)
- Exogenous contamination (peritoneal dialysis catheters, trauma, open surgery)
- Female genital tract (pelvic inflammatory disease, salpingitis)
- Haematogenous spread (rare)
Chemical (sterile initially):
- Bile leakage - highly irritating, usually complicated by secondary bacterial infection
- Pancreatic enzymes (acute haemorrhagic pancreatitis) - fat necrosis and enzymatic peritonitis
- Barium (from contrast studies)
Other:
- Starch peritonitis (allergic/foreign body reaction to surgical glove powder)
- Endometriosis (haemorrhage acts as irritant)
- Ruptured dermoid cysts (keratin-induced granulomatous reaction)
- Familial Mediterranean fever
- Bailey and Love's Short Practice of Surgery, 28th Ed., p. 1109
- Robbins, Cotran & Kumar Pathologic Basis of Disease
Pathophysiology
Normal peritoneal fluid contains <30 g/L protein and <300 WBC/µL (mainly mononuclear). When bacteria or chemical irritants enter the peritoneal cavity:
- Early phase - rapid influx of polymorphonuclear leukocytes (PMNs) driven by resident-cell chemokine synthesis
- Exudative phase - serous fluid accumulates, becomes turbid, then frankly purulent
- Fibrinous phase - fibrin plaques coat viscera and abdominal wall, loops of bowel adhere to each other and to the parietes
- Late phase - frank pus, abscess formation in dependent spaces (pelvis, subphrenic, Morrison's pouch), or systemic sepsis/bacteraemia
At surgery the inflamed peritoneum appears reddened, thickened and has a velvety texture, with yellow/white fibrin plaques and turbid exudate.
Harrison's Principles of Internal Medicine, 22e, p. 1113-1114
Primary (Spontaneous) Bacterial Peritonitis (SBP)
Epidemiology: Occurs in ≤10% of cirrhotic patients with ascites. Also seen in nephrotic syndrome (children), congestive heart failure, SLE, and lymphoedema.
Pathogenesis:
- Haematogenous seeding of ascitic fluid (a good growth medium)
- Diseased liver + altered portal circulation → defective bacterial filtration
- Reduced opsonic/phagocytic capacity of PMNs in advanced liver disease
- Gut dysbiosis with increased Enterobacteriaceae + small intestinal bacterial overgrowth → pathologic bacterial translocation
- Reduced Paneth cell defensins, portal hypertensive enteropathy
Microbiology: Monomicrobial - E. coli most common; also streptococci, enterococci, Klebsiella. Anaerobes are rare (their presence should prompt reconsideration of the diagnosis toward secondary peritonitis). Important current trend: increasing gram-positive bacteria and ESBL-producing Enterobacteriaceae due to widespread quinolone prophylaxis.
Clinical features:
- Fever (up to 80% of patients) - most common sign
- Abdominal pain and peritoneal signs may be present but are often subtle
- Non-localising symptoms: malaise, fatigue, hepatic encephalopathy, acute kidney injury, jaundice
Diagnosis: Sample peritoneal fluid in any cirrhotic patient with ascites and fever. >250 PMN/µL in ascitic fluid is diagnostic (this threshold does not apply to secondary peritonitis).
Treatment:
- IV third-generation cephalosporin (e.g., cefotaxime, ceftriaxone)
- IV albumin (1.5 g/kg at diagnosis + 1 g/kg on day 3) to reduce acute kidney injury and mortality
- Prophylaxis with norfloxacin in high-risk patients (low-protein ascites, prior SBP episode)
Secondary Peritonitis
The most common form, arising from a perforated or inflamed intraabdominal viscus. It is polymicrobial - aerobic gram-negative bacilli (E. coli, Klebsiella) plus anaerobes (Bacteroides fragilis, C. perfringens) are the rule.
Clinical Features
Localised peritonitis:
- Pain in the affected region (somatic - parietal peritoneum is extensively innervated)
- Involuntary guarding (reflex abdominal wall muscle contraction)
- Rebound tenderness (pain on releasing examiner's hand)
- Pyrexia and tachycardia
Diffuse peritonitis (surgical emergency):
- Severe, generalised abdominal pain, worse on movement, coughing, and respiration
- Patient lies motionless, often with knees drawn up
- "Board-like rigidity" - entire abdominal musculature in reflex contraction
- Hippocratic facies (gravely ill appearance)
- Generalised ileus → abdominal distension
- Haemodynamic instability: hypotension, tachycardia, fever
- Progressive confusion → loss of consciousness if untreated
Additional features:
- Shoulder tip ("phrenic") pain if inflammation reaches the diaphragm - referred via C5 dermatome
- Pelvic tenderness on digital rectal/vaginal examination if pelvic source
- Signs may be blunted in obese patients or those on immunosuppressants
Bailey and Love's Short Practice of Surgery, 28th Ed., pp. 1109-1111 Harrison's Principles of Internal Medicine, 22e, p. 1114
Summary of clinical features (Bailey & Love):
- Abdominal pain, worse on movement, coughing and deep respiration
- Constitutional upset: anorexia, malaise, fever, lassitude
- GI upset: nausea +/- vomiting
- Pyrexia (may be absent)
- Raised pulse rate
- Tenderness +/- guarding / rigidity / rebound
Investigations
| Investigation | Finding / Purpose |
|---|---|
| CT abdomen (with contrast) | Investigation of choice; identifies source, free gas, collections |
| Erect CXR | Subdiaphragmatic free gas (pneumoperitoneum) in perforation |
| Lateral decubitus XR | Alternative to erect CXR in unstable patients |
| Abdominal ultrasound | Limited specificity except for tubo-ovarian pathology |
| FBC | Leukocytosis with left shift (band forms) |
| CRP, procalcitonin | Support diagnosis; rarely diagnostically specific |
| Ascitic fluid tap (SBP) | Cell count >250 PMN/µL is diagnostic; culture in blood culture bottles |
| Laparoscopy | If CT/USS inconclusive |
| Peritoneal fluid Gram stain | Insensitive for bacteria; useful mainly for early yeast detection |
Microbiology Summary
| Setting | Organisms |
|---|---|
| SBP / cirrhosis | E. coli, streptococci, Klebsiella (monomicrobial) |
| Secondary (GI perforation) | E. coli, streptococci, S. aureus, enterococci, C. perfringens, Bacteroides (polymicrobial) |
| Peritoneal dialysis (PD) | S. epidermidis (mild), S. aureus, gram-negatives, fungi |
| Fungal peritonitis | Candida spp. (PD patients; immunocompromised) |
| Mycobacterial | M. tuberculosis (chronic presentation) |
Treatment
Surgical / Interventional (Secondary Peritonitis)
- Expedient surgical intervention - remove the underlying cause (seal perforation, resect gangrenous bowel, drain abscess)
- Peritoneal lavage - dilute and evacuate contamination
- At laparotomy: drain all pus, irrigate, consider open abdomen / "damage control" surgery in severe cases
Antibiotic Therapy
Community-acquired, mild-to-moderate:
- Piperacillin/tazobactam 3.375 g IV q6h, OR
- Ticarcillin/clavulanate 3.1 g IV q4-6h, OR
- Fluoroquinolone (e.g., levofloxacin 750 mg IV q24h) OR ceftriaxone 2 g IV q24h + metronidazole 500 mg IV q8h
Health-care-associated / ICU / severe:
- Imipenem 500 mg IV q6h, OR
- Meropenem 1 g IV q8h, OR
- Piperacillin/tazobactam 4.5 g IV q6h (higher dose), OR
- Cefepime/ceftazidime 2 g IV q8h + metronidazole
Enterococcal coverage (add if very ill, cephalosporin-based regimen): ampicillin or vancomycin; use linezolid/daptomycin for VRE.
Antifungal coverage: warranted if Candida grows from a sterile site.
Newer agent: Eravacycline (tetracycline class) 1 mg/kg IV q12h - FDA-approved for complicated intraabdominal infections.
Harrison's Principles of Internal Medicine, 22e, p. 1115
Peritonitis in Peritoneal Dialysis (PD-Related)
A distinct and important entity in nephrology:
Diagnosis (requires 2 of 3):
- Abdominal pain
- Cloudy peritoneal effluent / WBC >100/mm³ (>50% PMN)
- Positive culture of dialysis effluent
Routes of infection:
- Transluminal (through catheter lumen) - most common
- Pericatheter route
- Transmural bacterial migration (associated with constipation, diarrhoea, recent colonoscopy, diverticulitis)
- Haematogenous spread
- Ascending via female genital tract
Key points:
- S. epidermidis causes milder symptoms than S. aureus or gram-negatives
- Fungal peritonitis (Candida) is an indication for catheter removal
- PD-related peritonitis is rarely associated with bacteraemia (unlike surgical peritonitis)
- Gram stain of effluent is insensitive; culture by inoculating 5-10 mL into blood culture bottles
Brenner and Rector's The Kidney, 2-Volume Set; Comprehensive Clinical Nephrology, 7th Ed.
Complications
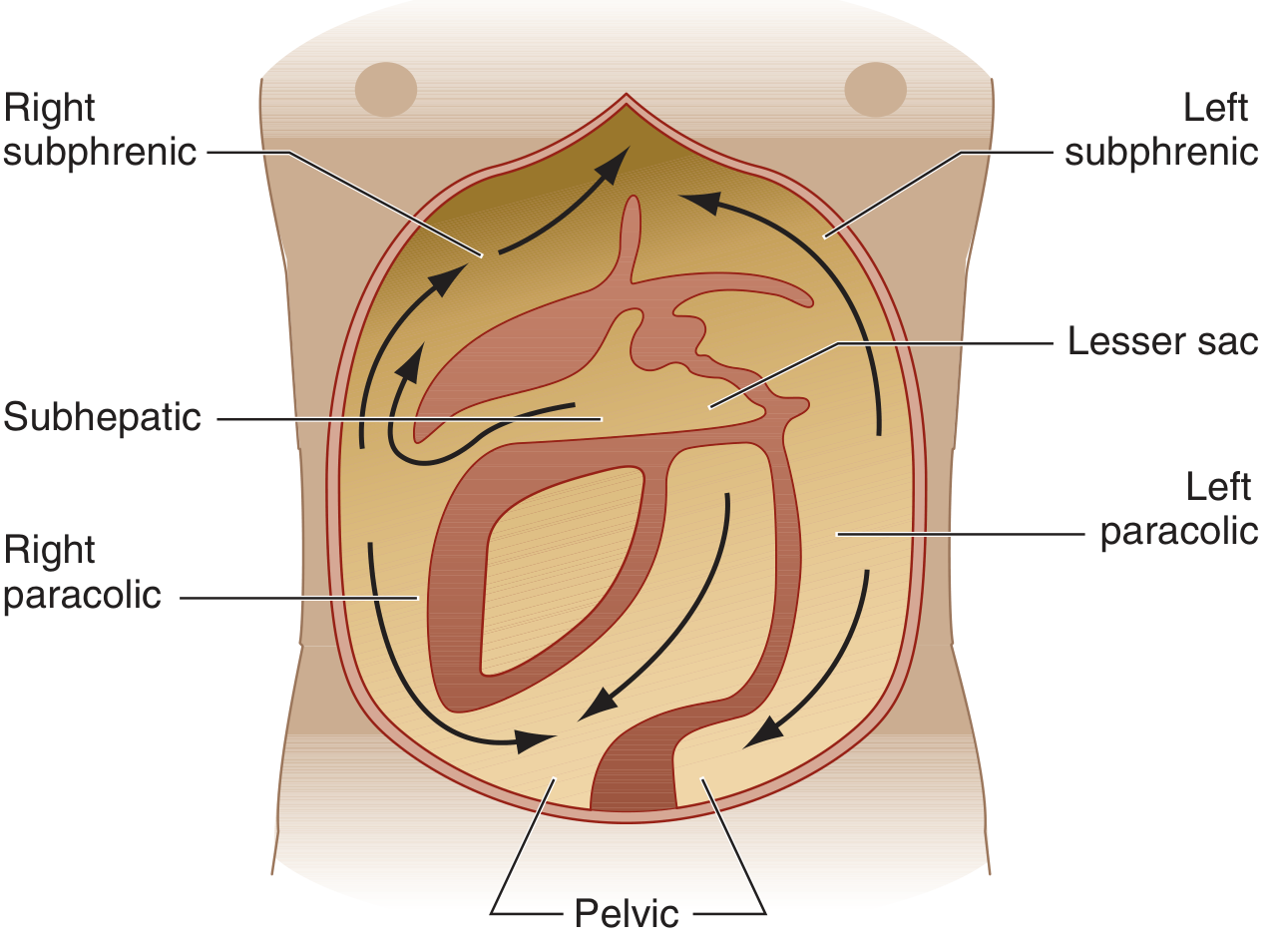
- Intraabdominal abscess formation - subphrenic (R > L due to falciform ligament barrier), subhepatic (Morrison's pouch), pelvic
- Sepsis syndrome / bacteraemia - especially in secondary peritonitis
- Paralytic ileus
- Adhesions - risk of future bowel obstruction
- Multi-organ failure - in advanced or untreated cases
- Death - untreated diffuse peritonitis is rapidly fatal
Special Forms
| Type | Key Features |
|---|---|
| Tuberculous peritonitis | Chronic; granulomatous; reaction typically remains superficial |
| Fungal (Candida) peritonitis | PD patients; immunocompromised; mandates catheter removal |
| Chemical (bile/pancreatic enzyme) | Sterile initially; intense peritoneal reaction; secondary infection common |
| Eosinophilic peritonitis | >10% eosinophils in effluent; early after PD catheter placement or drug reactions |
| Sclerosing peritonitis | Dense fibrosis; may represent IgG4-related disease |
| Familial Mediterranean fever | Episodic, self-limiting sterile peritonitis |
Sources:
- Harrison's Principles of Internal Medicine, 22e (2025), Chapter 137
- Bailey and Love's Short Practice of Surgery, 28th Ed., Chapter 65
- Robbins, Cotran & Kumar Pathologic Basis of Disease
- Brenner and Rector's The Kidney, 2-Volume Set
- Comprehensive Clinical Nephrology, 7th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.