Helicobacter pylori infection
Reading File
Finding Sources
Searching PubMed
"Helicobacter pylori"[MeSH Terms] AND treatment
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
I now have comprehensive information to compose a thorough answer. Let me compile it.
Helicobacter pylori Infection
Overview
H. pylori is a curved, microaerophilic, gram-negative rod that colonizes the gastric mucosa of roughly 50% of the world's population. Barry Marshall and Robin Warren confirmed its causal role in gastritis in the early 1980s and received the Nobel Prize in Physiology or Medicine in 2005. It is classified by the WHO as a Group 1 (definite) carcinogen.
Microbiology
- Curved gram-negative rod, urease-positive
- Produces urease at very high levels - a hallmark exploited by multiple diagnostic tests
- Key virulence factors:
- CagA (cytotoxin-associated gene A) and VacA (vacuolating cytotoxin A): these proteins drive greater mucosal inflammation and are strongly associated with peptic ulceration and gastric cancer risk
- The cag pathogenicity island induces high cytokine production
- Outer membrane proteins BabA and OipA mediate enhanced epithelial adhesion
- The s1m1 VacA genotype correlates with higher pathogenicity
(Medical Microbiology 9e; Goldman-Cecil Medicine)
Pathophysiology
H. pylori hydrolyses urea to produce ammonia, a strong alkali that:
- Disrupts the gastric mucous barrier
- Acts on antral G cells to cause gastrin release via disrupted negative feedback → modest hypergastrinaemia → inappropriate acid hypersecretion
The organisms also trigger a classical inflammatory cascade: neutrophil migration and degranulation, followed by macrophage and lymphocyte accumulation. This leads to:
- Chronic type B (antral) gastritis: the near-universal result of infection
- Duodenal ulceration: H. pylori cannot colonize normal duodenum, but excess acid causes duodenal gastric metaplasia, which can be colonized, producing duodenitis and eventual ulceration
- Gastric ulceration: direct mucosal breakdown by enzymatic disruption
- Hypochlorhydria and gastric cancer: corpus-dominant gastritis (more common in developing countries) leads to gland atrophy → intestinal metaplasia → dysplasia → adenocarcinoma
(Bailey & Love's Short Practice of Surgery 28th ed.)
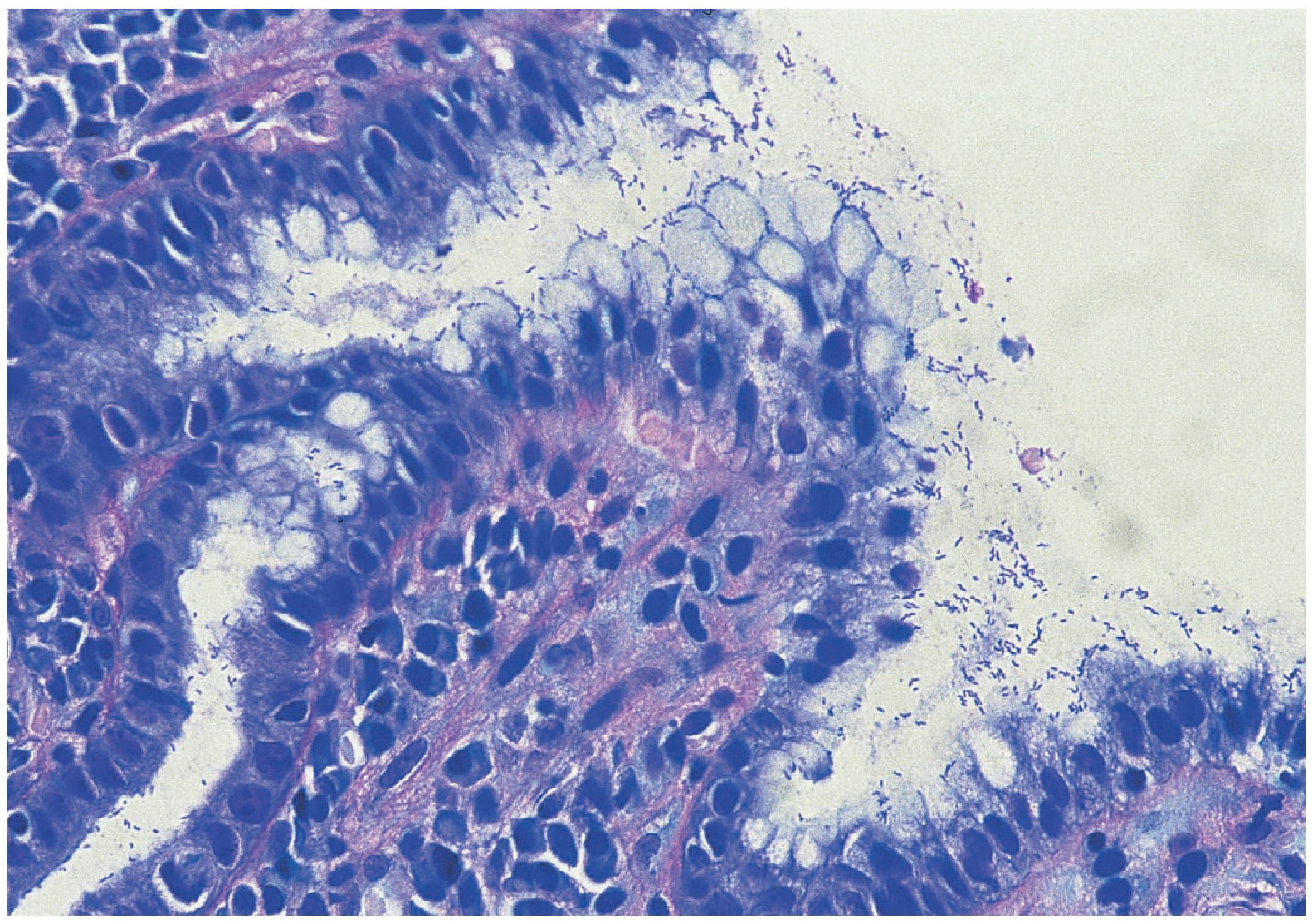
Figure: Antral mucosa colonised with H. pylori (modified Giemsa stain) - Bailey & Love's, p. 1176
Epidemiology
- Affects up to 50% of the world's population; prevalence is up to 80-90% in some developing nations
- Infection is predominantly acquired in childhood; inversely related to socioeconomic status
- Fecal-oral spread is the most likely route; organism found in feces, not saliva/dental plaque
- Humans are the primary reservoir; no seasonal incidence
- Risk for developing ulcer disease during persistent colonization: 5-15% (3-8x higher than uninfected individuals)
(Medical Microbiology 9e; Goldman-Cecil Medicine)
Associated Diseases
| Condition | Notes |
|---|---|
| Chronic gastritis (type B) | Near-universal in infected individuals |
| Duodenal ulcer | >90% of duodenal ulcers are H. pylori-related |
| Gastric ulcer | ~70-75% associated |
| Gastric adenocarcinoma | WHO Group 1 carcinogen; corpus gastritis → atrophy → metaplasia → cancer |
| MALT lymphoma | Low-grade B-cell lymphoma; eradication alone can induce remission in early disease |
| Functional dyspepsia | Eradication produces modest symptomatic benefit in a subset |
Diagnosis
Non-invasive (preferred in community/test-and-treat):
- ¹³C or ¹⁴C urea breath test (UBT): exploits urease activity; highly sensitive and specific; recommended for both pretreatment diagnosis and post-treatment confirmation
- Stool antigen test (SAT): sensitive and specific; useful for diagnosis and confirming eradication
- Serology (IgG ELISA): demonstrates exposure, not necessarily active infection; cannot confirm eradication; role is limited to non-invasive test-and-treat strategies
Invasive (endoscopy-based):
- Rapid urease test (CLO test): performed on gastric biopsy; rapid, relatively sensitive, highly specific
- Histology: modified Giemsa or Warthin-Starry silver stain; sensitive and specific
- Culture: microaerophilic conditions required; slow growth; relatively insensitive unless multiple biopsies taken; important for susceptibility testing
Note: PPIs, bismuth, and antibiotics suppress H. pylori and cause false-negative non-invasive tests; stop PPIs ≥2 weeks and antibiotics ≥4 weeks before testing.
(Medical Microbiology 9e; Bailey & Love's, p. 1176; Goldman-Cecil, p. 1445)
Treatment - Eradication Regimens
Post-treatment confirmation must be done at least 4 weeks after completing therapy (to avoid false negatives from suppression). UBT or SAT are the tests of choice.
First-line: Choice Based on Local Clarithromycin Resistance
Maastricht V/Florence Consensus classifies regions into:
- Low resistance (<15% clarithromycin resistance): triple therapy remains acceptable
- High resistance (>15%): quadruple therapy preferred
Standard Triple Therapy (14 days, low-resistance areas)
| Regimen | Drugs | Dose |
|---|---|---|
| PAC | PPI + Amoxicillin + Clarithromycin | PPI (standard dose BD), Amoxicillin 1g BD, Clarithromycin 500mg BD |
| PCM (penicillin allergy) | PPI + Clarithromycin + Metronidazole | PPI BD, Clarithromycin 250-500mg BD, Metronidazole 400mg BD |
- Double-dose PPI (omeprazole 40mg BD equivalent) raises eradication rates by ~10%
- Vonoprazan 20mg BD is an emerging alternative to PPI with strong acid suppression
- Clarithromycin resistance is rising globally; cure rates in many countries have fallen to <80% (some <50%)
Bismuth-based Quadruple Therapy (14 days, high-resistance areas or first-line)
PPI + Bismuth compound + Tetracycline + Nitroimidazole (metronidazole)
- Achieves eradication in ~85-90% of patients
- First-line preference when clarithromycin resistance is high
Non-bismuth Quadruple Therapies
| Type | Regimen | Notes |
|---|---|---|
| Concomitant | PPI + Amoxicillin + Clarithromycin + Metronidazole (all together, 14 days) | Most effective non-bismuth quadruple; PPI 40mg BD preferred |
| Sequential | PPI + Amoxicillin x5 days → PPI + Clarithromycin + Nitroimidazole x5 days | Equivalent to 14-day triple therapy |
| Hybrid | PPI + Amoxicillin x5 days → PPI + Amoxicillin + Clarithromycin + Metronidazole x5 days | Intermediate approach |
Rescue/Second-line Therapy
- Levofloxacin-based quadruple (PPI + levofloxacin + amoxicillin ± bismuth) - if first-line fails
- Susceptibility-guided therapy: increasingly recommended in regions with high resistance; culture with antibiogram determines optimal regimen
- Reinfection post-successful eradication is rare (<0.5%), but incomplete eradication is a common clinical problem
(Yamada's Gastroenterology 7e; Goldman-Cecil Medicine, Table 125-4; Bailey & Love's, p. 1177)
Indications for Eradication
- All peptic ulcers (gastric and duodenal) - mandatory
- Gastric MALT lymphoma (can achieve complete remission in early-stage disease)
- Functional dyspepsia (modest benefit in a subset)
- Early gastric cancer post-resection (reduces metachronous cancer risk)
- Before long-term NSAID or aspirin therapy
- First-degree relatives of gastric cancer patients
- H. pylori-positive patients requesting treatment (test-and-treat strategy)
Recent Evidence (2024-2026)
- A 2025 systematic review and meta-analysis in Gastroenterology (Ford et al., PMID 39824392) confirms that H. pylori eradication significantly reduces gastric cancer risk in positive individuals, reinforcing current guidelines for universal treatment of confirmed infection.
- Globally, clarithromycin resistance continues to rise, supporting the shift toward bismuth quadruple or concomitant regimens as preferred first-line therapy in most regions.
Key Points Summary
- H. pylori is the most common human infection worldwide and the primary cause of peptic ulcer disease
- Urease production is its defining biochemical feature and the basis of the urea breath test and CLO test
- Virulence factors (CagA, VacA, cag PAI) determine disease severity; most infections are asymptomatic
- Diagnosis: UBT or stool antigen for non-invasive; CLO test or histology if endoscopy is performed
- Treatment requires combination therapy (PPI + ≥2 antibiotics); choice depends on local resistance patterns
- Clarithromycin resistance is rising globally, making bismuth quadruple or concomitant therapy increasingly preferred
- Post-eradication testing (≥4 weeks post-therapy) by UBT or SAT is mandatory to confirm success
This is a shared conversation. Sign in to Orris to start your own chat.