Male reproductive system normal physiology and pathology
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive material to write a thorough, well-illustrated answer. Let me compose it.
Male Reproductive System: Normal Physiology and Pathology
PART 1 — NORMAL PHYSIOLOGY
1. Anatomy and Components
The male reproductive system has two functional divisions:
Gonads (Testes): Produce gametes (spermatozoa) and secrete hormones (primarily testosterone).
Sex Accessory Organs: Epididymides, vas deferens, seminal vesicles, ejaculatory ducts, prostate, bulbourethral glands (Cowper's glands), urethra, and penis - collectively store and transport spermatozoa.
The testes are normally maintained at 35-36°C (1-2°C below body temperature), essential for normal spermatogenesis. This is achieved by a countercurrent heat exchange arrangement between testicular arteries and veins in the spermatic cord. - Costanzo Physiology 7th Edition
Testicular composition:
- 80% seminiferous tubules - the site of spermatogenesis (convoluted loops, 120-300 µm diameter, arranged in lobules)
- 20% connective tissue + interstitial Leydig cells
2. Key Testicular Cell Types
Sertoli Cells (FSH-responsive)
Located within seminiferous tubule epithelium, Sertoli cells serve four major functions:
- Nutrient supply to differentiating sperm (which are isolated from blood)
- Blood-testis barrier - tight junctions between Sertoli cells create selective permeability, protecting developing sperm from noxious substances while allowing testosterone access
- Fluid secretion into the tubule lumen to transport sperm to the epididymis
- Androgen-binding protein (ABP) secretion - keeps local testosterone levels high near developing sperm cells
- Also produce inhibin (suppresses FSH) and aromatase (converts testosterone → estradiol)
Leydig Cells (LH-responsive)
Located in the interstitium between tubules; synthesize and secrete testosterone from cholesterol via P-450 enzyme pathways. The testes lack 21β-hydroxylase and 11β-hydroxylase (so cannot make glucocorticoids/mineralocorticoids) but have 17β-hydroxysteroid dehydrogenase to convert androstenedione → testosterone. - Costanzo Physiology 7th Edition
3. Hypothalamic-Pituitary-Gonadal (HPG) Axis
The HPG axis is the central regulator of male reproductive function:
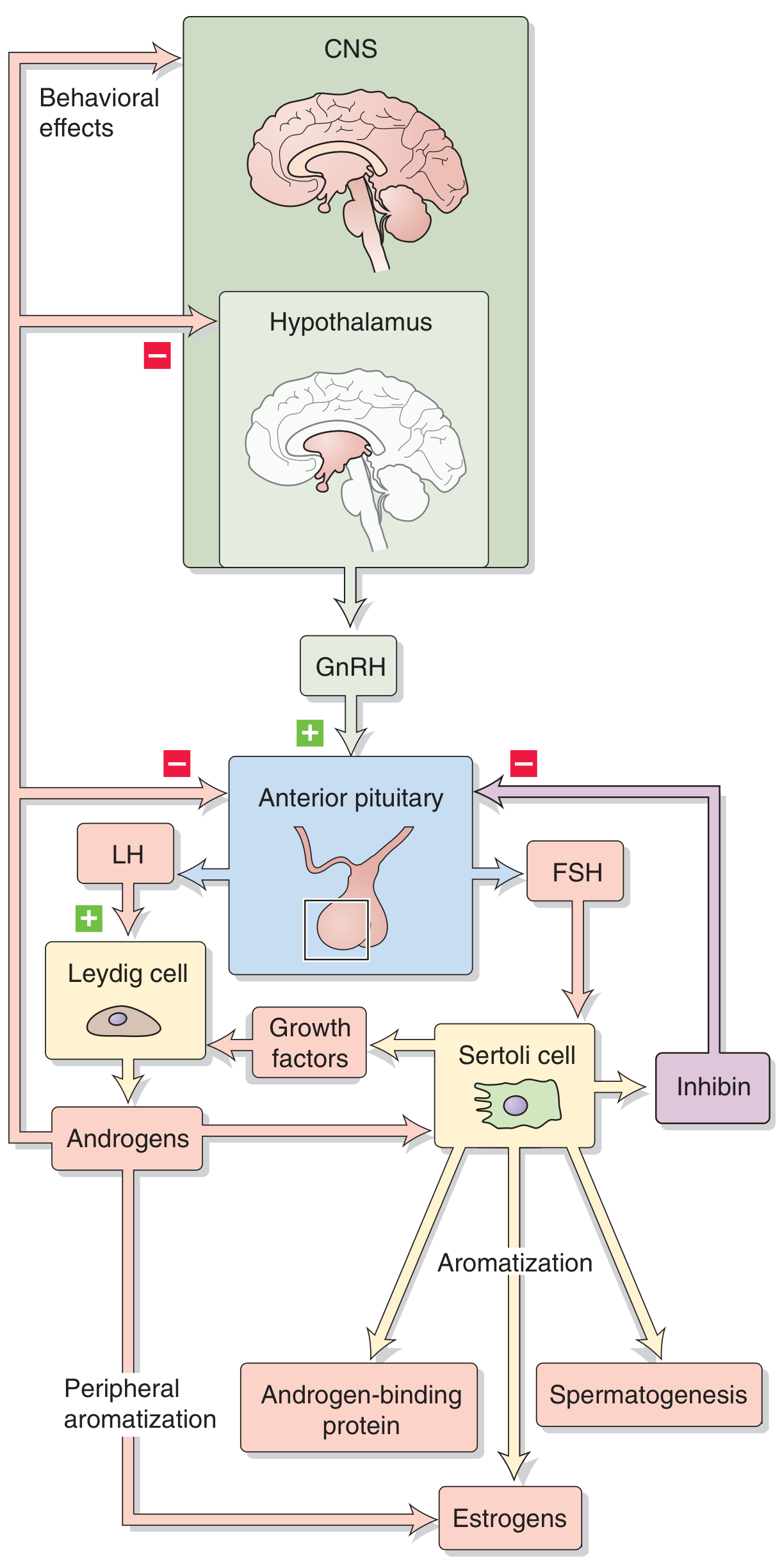
Figure: HPG axis. GnRH from the arcuate nucleus/preoptic area stimulates anterior pituitary gonadotrophs to release LH (acts on Leydig cells) and FSH (acts on Sertoli cells). Negative feedback occurs via testosterone and inhibin. - Medical Physiology (Boron & Boulpaep)
GnRH (Gonadotropin-Releasing Hormone):
- Decapeptide from hypothalamic arcuate nucleus and preoptic area neurons
- GnRH neurons originate embryologically in the olfactory placode, then migrate to hypothalamus
- Acts on gonadotroph cells via GPCR (Gαq) → PLC → IP3/DAG → Ca²⁺ release → LH and FSH secretion
- Secretion is pulsatile: ~8-14 LH pulses per 24 hours
- Continuous GnRH causes receptor downregulation and gonadotropin suppression (basis for GnRH agonist therapy in prostate cancer)
LH → Leydig cells → Testosterone
FSH → Sertoli cells → ABP, aromatase, inhibin, growth factors
Negative feedback:
- Testosterone inhibits both hypothalamus (↓GnRH) and anterior pituitary (↓LH sensitivity)
- Inhibin selectively suppresses FSH at the pituitary level
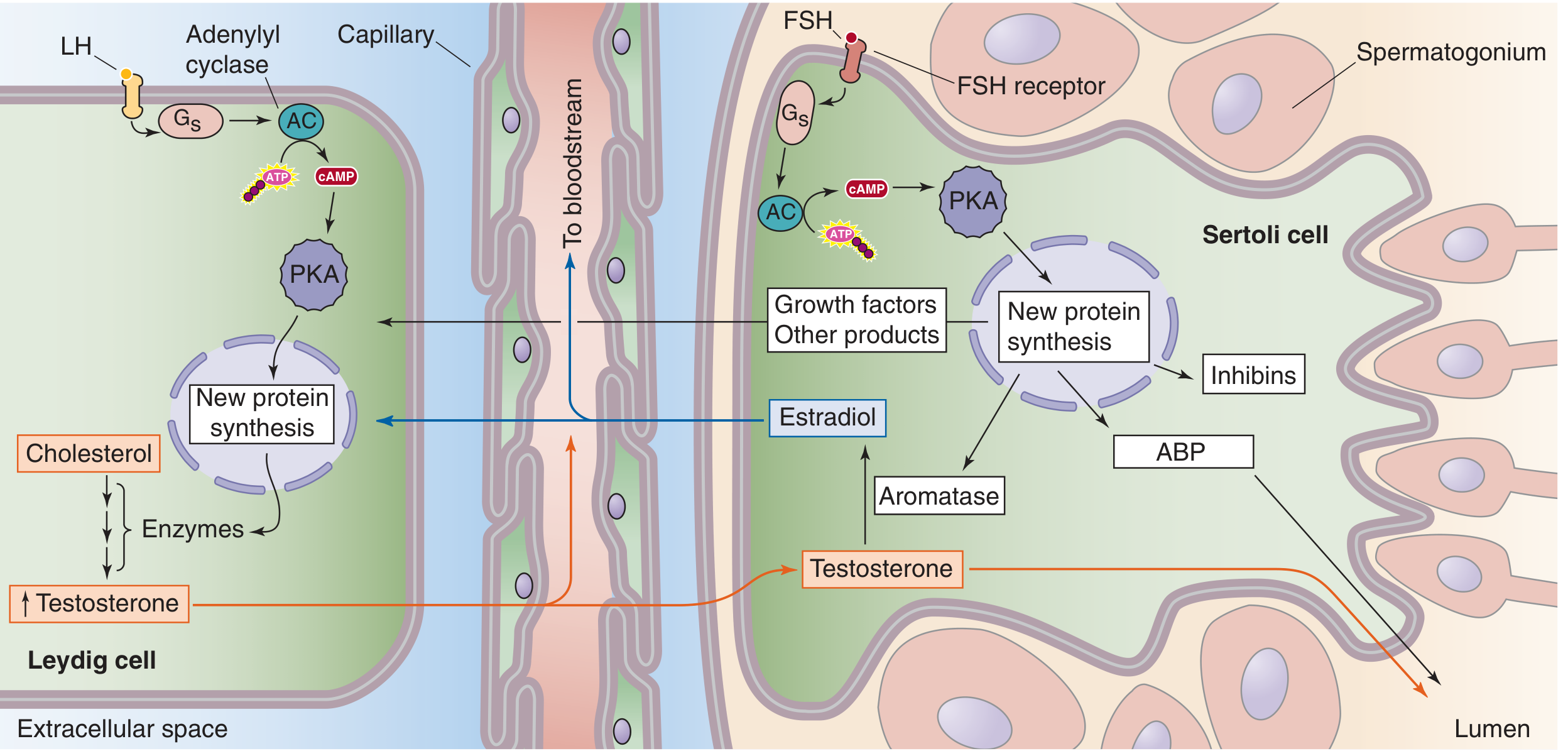
Figure: Leydig cell (left) - LH binding via cAMP/PKA → cholesterol → testosterone. Sertoli cell (right) - FSH binding → ABP, aromatase, growth factors, inhibin. Note cross-talk: Sertoli cells aromatize testosterone to estradiol, which feeds back on Leydig cells. - Medical Physiology (Boron & Boulpaep)
4. Spermatogenesis
Spermatogenesis occurs continuously from puberty to senescence along the length of the seminiferous tubules. The full cycle takes approximately 64 days. Two million spermatogonia begin this process daily, each giving rise to 64 spermatozoa → ~128 million sperm produced per day. - Costanzo Physiology 7th Edition
Three phases:
| Phase | Process | Cells Involved | Ploidy |
|---|---|---|---|
| 1. Mitotic divisions | Spermatogonia divide to generate spermatocytes | Spermatogonia (stem cells) | Diploid (2n) |
| 2. Meiosis | Two meiotic divisions reduce chromosome number | Primary → secondary spermatocytes → spermatids | 2n → n (haploid) |
| 3. Spermiogenesis | Cytodifferentiation of spermatids into spermatozoa | Round spermatids → spermatozoa | Haploid (n) |
Spermiogenesis involves: loss of excess cytoplasm, development of the flagellum (middle piece + tail), formation of the acrosome (containing hydrolytic enzymes), and nuclear condensation.
Spatial organization: Spermatogonia sit at the basal compartment (outside blood-testis barrier); primary spermatocytes and beyond are in the adluminal compartment (inside barrier, immunologically privileged).
Spermatogenic wave: A temporal organization ensuring mature spermatozoa are produced continuously rather than in batches.
Requirements for optimal spermatogenesis:
- Two cell types: Leydig cells + Sertoli cells
- Two gonadotropins: LH + FSH
- One androgen: Testosterone
- Temperature: 35-36°C (1-2°C below body temperature)
5. Testosterone: Synthesis, Transport, and Actions
Synthesis: Leydig cells → cholesterol → pregnenolone → via multiple P-450 steps → testosterone
Transport: ~98% bound to proteins in blood (Sex hormone-binding globulin [SHBG] + albumin); ~2% free (biologically active)
5α-reductase conversion: In many target tissues (prostate, skin, external genitalia), testosterone → dihydrotestosterone (DHT) via 5α-reductase. DHT binds the androgen receptor with much higher affinity.
Actions by mediator (Table 10.1 - Costanzo):
| Mediated by Testosterone | Mediated by DHT |
|---|---|
| Differentiation of epididymis, vas deferens, seminal vesicles | Differentiation of penis, scrotum, prostate |
| Increased muscle mass | Male hair pattern |
| Pubertal growth spurt | Male pattern baldness |
| Epiphyseal closure | Sebaceous gland activity |
| Growth of penis and seminal vesicles | Prostate growth |
| Deepening of voice | |
| Spermatogenesis | |
| Negative feedback on pituitary | |
| Libido |
Plasma testosterone across the lifespan:
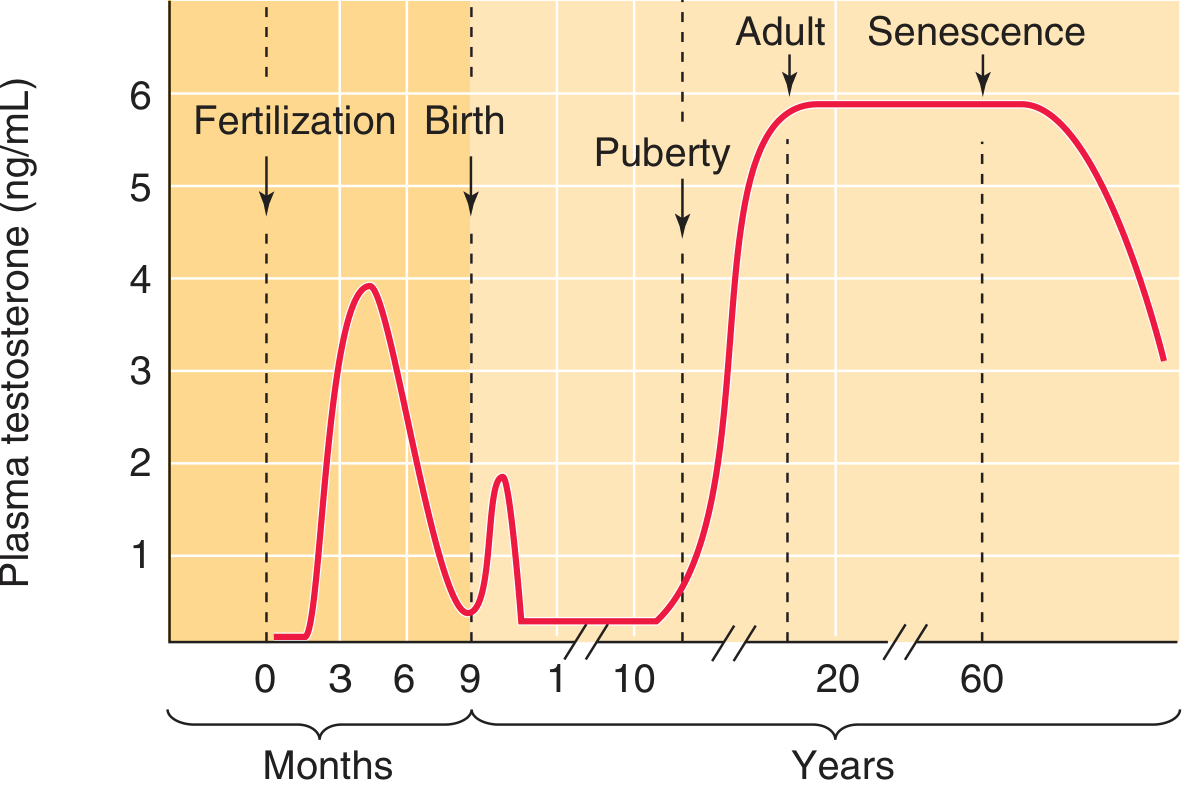
Figure: Testosterone peaks twice in fetal life (stimulating male genital differentiation), shows a brief neonatal surge, remains low throughout childhood, rises sharply at puberty (~5.5-6 ng/mL), is stable in adulthood, then declines progressively with senescence. - Medical Physiology (Boron & Boulpaep)
6. Sex Accessory Glands: Functions and Secretions
| Structure | Contribution to Semen | Function |
|---|---|---|
| Epididymis | Maturation site | Sperm maturation and storage (viable for months); gains motility and fertilizing capacity here |
| Vas deferens / Ampulla | Citrate, fructose-rich fluid | Storage; nutrition for sperm |
| Seminal vesicles | ~60% of semen volume; fructose, citrate, prostaglandins, fibrinogen | Nutrition; prostaglandins make cervical mucus penetrable and stimulate female tract peristalsis |
| Prostate | ~20-30% of semen volume; citrate, calcium, enzymes, slightly alkaline | Neutralizes acidic vaginal secretions; increases sperm motility |
| Bulbourethral (Cowper's) glands | Alkaline mucus | Lubrication; neutralize urethral acidity before ejaculation |
The accessory glands compose ~90% of semen volume; sperm account for only ~10%. - Costanzo Physiology 7th Edition
7. Capacitation and the Acrosomal Reaction
After ejaculation, sperm must reside in the female reproductive tract for 4-6 hours for capacitation to occur:
- Inhibitory seminal fluid factors are washed off
- Cholesterol withdrawn from sperm membrane
- Surface proteins redistributed
- Ca²⁺ influx increases sperm motility (whip-like movement)
- Acrosomal reaction: Acrosomal membrane fuses with outer sperm membrane → pores release hydrolytic/proteolytic enzymes → penetrate zona pellucida of ovum
8. Puberty
During early puberty, pulsatile GnRH increases, driving FSH and LH rises → Leydig cell proliferation → surging plasma testosterone. Key secondary sexual characteristics develop: growth spurt, muscle mass, voice deepening, pubic/axillary hair, penile/testicular growth, and initiation of spermatogenesis.
PART 2 — PATHOLOGY
1. Erectile Dysfunction (ED)
Definition: Inability to attain or maintain an erection sufficient for satisfactory sexual performance.
Classification:
| Type | Mechanism |
|---|---|
| Psychogenic | CNS/limbic inhibition of spinal erection centers; depression, performance anxiety |
| Neurogenic | Failure to initiate (spinal cord injury, multiple sclerosis, radical prostatectomy neuropraxia) |
| Arterial/Vasculogenic | Failure to fill - atherosclerosis, hypertension, diabetes mellitus |
| Venous (corporal veno-occlusive) | Failure to store - venous leak |
| Hormonal | Hypogonadism, hyperprolactinemia |
| Drug-induced | Antihypertensives, antidepressants, antipsychotics, alcohol |
Risk factors: Vascular disease, metabolic syndrome, diabetes mellitus, hypertension, smoking, neurological disease, hormonal disorders, psychiatric conditions, substance abuse. A unifying theme of biologic risk factors is endothelial/vascular dysfunction. Previously up to 90% were attributed to psychogenic causes, but most experts now recognize ED is predominantly a functional/physical disorder. - Campbell Walsh Wein Urology
Prevalence: International studies show age-standardized prevalence of 6-33%; the most common risk factors are consistent across geographic regions.
2. Testicular Cancer (Germ Cell Tumors - GCTs)
Epidemiology: ~9,610 new cases/year in the US; most common malignancy in men aged 15-35. Risk factors: cryptorchidism (most significant), prior contralateral testicular cancer, Klinefelter syndrome. - Washington Manual of Medical Therapeutics
Pathological classification:
| Type | % of GCTs | Tumor Markers |
|---|---|---|
| Seminoma (pure) | ~50% | β-hCG (elevated in ~15%), LDH; AFP is NOT elevated (key distinguisher) |
| Nonseminomas | ~50% | |
| - Embryonal carcinoma | AFP, β-hCG | |
| - Choriocarcinoma | β-hCG (markedly elevated) | |
| - Yolk sac tumor | AFP | |
| - Teratoma | Variable | |
| - Mixed GCT |
GCTs account for ~95% of all testicular tumors; sex cord tumors (Sertoli cell tumor, Leydig cell tumor) = ~5%.
Clinical presentation: Painless testicular mass (most common); testicular pain, hydrocele, gynecomastia. Advanced disease: back/flank pain, B symptoms (fever, night sweats, weight loss).
Diagnostic workup:
- Testicular ultrasound: heterogeneous, hypoechoic, vascular intratesticular lesion
- Tumor markers: AFP, β-hCG, LDH
- Unilateral radical orchiectomy (trans-scrotal biopsy is contraindicated - risk of local/atypical recurrence)
- Staging CT abdomen/pelvis; CXR (CT chest if abdominal nodes enlarged or CXR abnormal in seminoma)
Staging (TNM + Serum Markers "S"):
- Stage I: Confined to scrotum (T1-4)
- Stage II: Lymph node involvement (N1-3)
- Stage III: Visceral/distant metastases (M1)
- Serum markers: S0 (normal), S1 (LDH <1.5×ULN, hCG <5,000, AFP <1,000), S2/S3 (progressive elevation)
Treatment:
- Seminoma Stage I: Orchiectomy → surveillance, single-agent carboplatin, or radiation
- Seminoma Stages IIA/IIB: Chemotherapy (BEP: bleomycin, etoposide, cisplatin) or radiation
- Nonseminoma Stage I: Orchiectomy → surveillance, RPLND, or BEP
- Sperm banking offered before treatment (fertility preservation)
3. Benign Prostatic Hyperplasia (BPH)
Pathophysiology: Nodular hyperplasia of stromal and glandular elements in the transition zone/periurethral zone of the prostate. DHT (via 5α-reductase) is the primary driver - hence 5α-reductase inhibitors (finasteride, dutasteride) are used therapeutically.
Symptoms (Lower Urinary Tract Symptoms - LUTS):
- Obstructive: hesitancy, poor stream, straining, incomplete emptying
- Irritative/storage: urgency, frequency, nocturia
Complications: Urinary retention, recurrent UTIs, bladder diverticula, hydronephrosis/renal insufficiency.
Treatment: α-blockers (tamsulosin - relax smooth muscle), 5α-reductase inhibitors (reduce gland size), TURP (surgical gold standard), laser procedures.
4. Prostate Cancer
The most common visceral malignancy in men. Arises predominantly in the peripheral zone of the prostate (unlike BPH in the transition zone). Androgen-dependent growth. Screening: PSA (prostate-specific antigen) + digital rectal examination. Graded by Gleason score (histological grade 1-5, most + second most common pattern). Treatment ranges from active surveillance (low-grade), radical prostatectomy, radiation, to androgen deprivation therapy (ADT) for advanced/metastatic disease. Bone metastases (osteoblastic) are characteristic.
5. Male Hypogonadism
Primary hypogonadism (hypergonadotropic): Testicular failure → low testosterone + high LH/FSH.
- Causes: Klinefelter syndrome (47,XXY - most common genetic cause), orchitis (mumps), chemotherapy/radiation, cryptorchidism, trauma
Secondary hypogonadism (hypogonadotropic): Hypothalamic/pituitary failure → low testosterone + low/normal LH/FSH.
- Causes: Kallmann syndrome (GnRH neuron migration failure + anosmia), hyperprolactinemia, pituitary tumors, systemic illness, opioid use
Clinical features: Reduced libido, erectile dysfunction, infertility, decreased muscle mass, osteoporosis, fatigue, anemia, loss of secondary sexual characteristics (if prepubertal - eunuchoid proportions).
6. Cryptorchidism (Undescended Testis)
Failure of one or both testes to descend into the scrotum. Present in ~3-4% of full-term male newborns; most descend spontaneously in the first year of life. Complications:
- Infertility (elevated scrotal temperature → spermatogenic damage - especially bilateral)
- Testicular malignancy risk increased 3-5× (risk partially persists even after orchiopexy)
- Torsion risk Treatment: Hormonal (hCG/GnRH) or orchiopexy (surgical) before 12-18 months.
7. Male Infertility
Affects ~15% of couples trying to conceive; male factor contributes in ~50% of cases.
| Category | Examples |
|---|---|
| Pre-testicular (endocrine) | Hypogonadotropic hypogonadism, hyperprolactinemia |
| Testicular | Sertoli-cell-only syndrome, maturation arrest, cryptorchidism, varicocele, Klinefelter syndrome |
| Post-testicular (obstructive) | Vas deferens obstruction (post-vasectomy, CF mutations), epididymal obstruction, ejaculatory duct obstruction |
Semen analysis: First-line investigation. WHO reference values: volume ≥1.5 mL, concentration ≥16 million/mL, total motility ≥42%, normal morphology ≥4% (Kruger strict criteria).
Varicocele: Dilation of pampiniform plexus veins; most common correctable cause of male infertility (more common on the left due to left spermatic vein draining at right angles into the left renal vein).
8. Testicular Torsion
Twisting of the spermatic cord; surgical emergency. Presents with sudden severe testicular pain, nausea/vomiting, and a high-riding testis with absent cremasteric reflex. Bell-clapper deformity (abnormal tunica vaginalis attachment) predisposes. Requires surgical detorsion within 6 hours (viability approaches 100% if <6 hours; ~50% at 12 hours; near 0% at 24 hours). Bilateral fixation (orchiopexy) is performed.
Key Regulatory Summary
Hypothalamus (arcuate nucleus)
↓ GnRH (pulsatile)
Anterior Pituitary
↓ LH ↓ FSH
Leydig cells Sertoli cells
↓ ↓
Testosterone ABP, Inhibin, Aromatase
↓ ↓
Spermatogenesis ← Testosterone (local paracrine)
Inhibin → ⊖ FSH (pituitary)
Testosterone → ⊖ LH + GnRH (negative feedback)
Sources: Costanzo Physiology 7th Edition | Medical Physiology (Boron & Boulpaep) | The Washington Manual of Medical Therapeutics | Campbell Walsh Wein Urology, 3-Volume Set | Smith and Tanagho's General Urology, 19th Edition | Tietz Textbook of Laboratory Medicine, 7th Edition
This is a shared conversation. Sign in to Orris to start your own chat.